
Abstract
We aimed to study the association between fasting plasma glucose, diabetes incidence and cardiovascular burden after 10–12 years. We evaluated diabetes and cardiovascular events incidences, carotid intima-media thickness and coronary artery calcium scores in ELSA-Brasil (the Brazilian Longitudinal Study of Adult Health) baseline (2008–2010) of 1536 adults without diabetes in 1998. We used regression models to estimate association with carotid intima-media thickness (in mm), coronary artery calcium scores (in Agatston points) and cardiovascular events according to fasting plasma glucose in 1998. Adjusted diabetes incidence rate was 9.8/1000 person-years (95% confidence interval: 7.7–13.6/1000 person-years). Incident diabetes was positively associated with higher fasting plasma glucose. Fasting plasma glucose levels 110–125 mg/dL were associated with higher carotid intima-media thickness (β = 0.028; 95% confidence interval: 0.003–0.053). Excluding those with incident diabetes, there was a borderline association between higher carotid intima-media thickness and fasting plasma glucose 110–125 mg/dL (β = 0.030; 95% confidence interval: −0.005 to 0.065). Incident diabetes was associated with higher carotid intima-media thickness (β = 0.034; 95% confidence interval: 0.015–0.053), coronary artery calcium scores ⩾400 (odds ratio = 2.84; 95% confidence interval: 1.17–6.91) and the combined outcome of a coronary artery calcium scores ⩾400 or incident cardiovascular event (odds ratio = 3.50; 95% confidence interval: 1.60–7.65). In conclusion, fasting plasma glucose in 1998 and incident diabetes were associated with higher cardiovascular burden.
Introduction
Diabetes mellitus is a highly prevalent condition, 1 with long, asymptomatic periods and, when left untreated, may result in significant atherosclerotic burden.2,3 These characteristics and the fact that fasting plasma glucose (FPG) test is widely available favour screening programmes.
Besides detecting individuals with previously undiagnosed diabetes, screening programmes may also identify individuals with impaired fasting glucose, defined as FPG levels between 100 and 125 mg/dL. 4 This condition received attention in the past years, and epidemiological studies have addressed the association between impaired fasting glucose and poorer outcomes in non-diabetic subjects, with mixed results.5,6 Levitzky et al. 7 analysed data from 4058 Framingham offspring cohort participants and found that an impaired fasting glucose between 110 and 125 mg/dL was associated with a higher 4-year risk of coronary heart disease or cardiovascular disease in women, but not in men. Yeboah et al., 8 analysing 6753 participants from the Multi-Ethnic Study of Atherosclerosis (MESA) study, found that impaired fasting glucose at baseline was not independently associated with incident cardiovascular events after 7.5 years of follow-up. Similarly, Schöttker et al. 9 analysed data from 3538 participants from a German study on prevention, early detection and treatment for chronic diseases among elder persons. They did not find an association between impaired fasting glucose and the development of chronic kidney disease after 8 years of follow-up.
ELSA-Brasil (The Brazilian Longitudinal Study of Adult Health) is a multicentre cohort study of 15,105 civil servants working in six academic institutions in Brazil. Specifically, 5061 of those participants are employees from the University of São Paulo who accepted the invitation to participate of the baseline examination, which occurred from 2008 to 2010. Previously, in 1998, the worksite health department of the same university applied a screening programme for its employees, which included FPG measurements. In this article, we analyse data from 1536 individuals without diabetes who underwent the screening in 1998 and joined the 2008–2010 ELSA-Brasil baseline assessment. Our aims were to determine (1) diabetes incidence rates in individuals with normal or impaired fasting glucose in 1998 after a mean follow-up of 11 years, (2) whether impaired fasting glucose in 1998 and/or incident diabetes were associated with subclinical atherosclerosis in ELSA-Brasil baseline assessment and (3) whether impaired fasting glucose in 1998 and/or incident diabetes were associated with non-fatal cardiovascular outcomes.
Methods
Study design
The 1998 screening assessment
All active civil employees from the University of São Paulo were invited by the Occupational Health Service to participate in a medical consultation including clinical and laboratorial data for cardiovascular risk factors in 1998. Of all employees, 6859 volunteers underwent a clinical consultation with collection of sociodemographic data, previous diagnosis of hypertension, diabetes, dyslipidaemia, smoking status and measurements of blood pressure, height and weight. In addition, FPG and total cholesterol [and, in a subsample, low-density lipoprotein (LDL)-cholesterol, high-density lipoprotein (HDL)-cholesterol and triglycerides] determinations were obtained.
ELSA-Brasil baseline assessment
Active and retired employees from the University of São Paulo participated in the ELSA-Brasil baseline assessment that occurred from 2008 to 2010. This assessment included questionnaires about personal and familiar antecedents, habits, medical diagnoses, as well as their date of acknowledgement and current treatments, and anthropometric measurements, clinical exams and laboratory evaluation. All ELSA-Brasil participants from São Paulo were also invited to perform a computed tomography to quantify coronary calcium. Additional data about the ELSA-Brasil design and cohort profile have been published earlier.10,11 This study is in accordance with the Helsinki Declaration and was approved by institutional review boards in all ELSA-Brasil centres (Approval number at São Paulo site, 659/09). All individuals signed informed consent.
Study sample
For this study, we evaluated 1545 civil servants from the University of São Paulo (aged 23–63 years in 1998), who participated in both 1998 screening and ELSA-Brasil baseline assessments, had a valid fasting glucose determination in both assessments, with no diabetes in 1998. We excluded 9 (0.6%) participants who self-reported incident outcomes in whom validation could not be performed, resulting in 1536 participants.
Study variables
Diabetes was defined as a medical history of diabetes mellitus or a FPG level ⩾126 mg/dL. In this study, we defined impaired fasting glucose as a FPG level between 100 and 109 mg/dL (5.56–6.06 mmol/L; level 1) or between 110 and 125 mg/dL (6.11–6.94 mmol/L; level 2), both in the absence of a diagnosis of diabetes. We opted to adopt these two different levels to be comparable to others.8,12 Blood samples were collected after a 12-h overnight fast. Plasma glucose determinations were performed at the same laboratory in 1998 and 2008–2010 using analytical methods, glucose-oxidase and hexokinase methods, respectively. Although methodologically different, there is excellent accuracy agreement between these techniques. 13 Dyslipidaemia was defined as a medical history of dyslipidaemia or a serum cholesterol determination ⩾240 mg/dL. We opted for these criteria as in the 1998 assessment we had no information about glycated haemoglobin or glucose tolerance test, and LDL and HDL cholesterol levels were available for a small subset of participants. Hypertension was defined by a medical history of hypertension, a systolic blood pressure ⩾140 mmHg or a diastolic blood pressure ⩾90 mmHg. These measurements were made after a 5-min rest in sitting position in a quiet and temperature-controlled room (20°C–24°C), in three measurements with 1-min interval. 14 Prevalent diabetes, hypertension or dyslipidaemia were defined by the presence of those criteria in 1998 evaluation. Incident diabetes, hypertension or dyslipidaemia were defined by the absence of those criteria in 1998 and a new diagnosis from 1999 to the ELSA-Brasil baseline assessment. We asked about smoking status (never, past or current), the age the participant started and quitted smoking, number of cigarettes per day and estimated total smoking pack-years.
Carotid intima-media thickness
Carotid intima-media thickness (CIMT) is a non-invasive measurement of subclinical atherosclerosis, which is altered from the initial phases of atherosclerotic disease. 15 The technique for CIMT measurement in the ELSA-Brasil was previously published.16–18 CIMT was measured by a technician blinded to diabetes status in the outer wall of a pre-defined carotid segment of 1 cm in length from 1 cm below carotid bifurcation, during three cardiac cycles. We used MIA™ software to standardize the reading and interpretation of carotid scans after image quality assessment. For the purposes of this article, we considered the average between left and right mean CIMT within an individual in analyses.
Coronary artery calcium
Coronary artery calcium (CAC) examinations were performed in a 64-detector computed tomography scanner (Brilliance 64, Philips Healthcare, Best, the Netherlands). After the scout images, each patient also underwent an ECG-gated prospective calcium score examination with a tube potential of 120 kV and a tube current adjusted to body habitus. Images were reconstructed in 2.5 mm slice thickness using standard filtered back projection. Coronary artery calcium scores (CACS) was evaluated in a blinded fashion by an experienced cardiologist using semiautomatic software (Calcium Scoring, Philips Workstation), following a method described by Agatston. 19 CACS was further categorized into four groups: 0, 0.1–99.9, 100–399.9 and ⩾400. CACS = 0 was used as reference in logistic regression models.
Cardiovascular outcomes
Individuals who had a myocardial infarction diagnosis or coronary revascularization until 1998 were considered to have prevalent clinical events. Incident clinical outcomes were considered for the participant who had no prevalent events and received a diagnosis of myocardial infarction or underwent coronary revascularization between 1999 and ELSA-Brasil baseline examination. Incident diabetes cases were validated using laboratory and use of medication in ELSA-Brasil baseline assessment. We reviewed medical charts to validate self-reported myocardial infarction and coronary revascularization between 1999 and ELSA-Brasil baseline assessment.
Statistical analysis
We used chi-square, Fisher’s exact and Kruskal–Wallis tests to compare categorical and continuous variables across groups, whenever applicable. We presented crude and adjusted diabetes incident rates (per 1000 person-years) for all individuals and then stratified by sex and body mass index (BMI) acquired in 1998. Incident rates were sex and age standardized, using the Brazilian population aged 20–69 years as reference, according to the 2000 Brazilian Census. We used Cox regression models to determine the risk of incident diabetes for individuals with impaired fasting glucose level 1 (FPG levels: 100–109 mg/dL) or impaired fasting glucose level 2 (FPG levels: 110–125 mg/dL) in 1998. We built crude and adjusted multiple linear regression models using CIMT (dependent variable) and multinomial regression models using CACS (dependent variable) to assess their association with (1) glucose levels measured in 1998 and (2) the occurrence of incident diabetes during the follow-up, as well. Explanatory variables included in adjusted models are (1) age, sex and race and (2) age, sex, race, BMI in 1998, BMI difference between assessments, smoking pack-years, and hypertension and dyslipidaemia status in both assessments. We repeated the analyses for the association of glucose levels with subclinical atherosclerosis excluding those with interim incident diabetes. We also built binary logistic regression models to determine the association between the occurrence of the composite variable of a CACS ⩾400 or the incidence of cardiovascular events (myocardial infarction or revascularization) with (1) glucose levels in 1998 and (2) the occurrence of incident diabetes. Analyses were performed using R software 20 version 3.1.2. Significance level was set at 0.05.
Results
Study sample included 1536 individuals, corresponding to 16,891 person-years with a mean follow-up of 11.0 years (Table 1). In 1998, 50.5% of the study sample was younger than 40 years and 50.2% had a BMI of 25 kg/m2 or above. Compared to participants with normal FPG, participants with higher glucose levels in 1998 were older (p < 0.001), more likely to be men (p < 0.001), of non-White races (p = 0.005), had a higher frequency of hypertension (p < 0.001) and higher BMI (p < 0.001). Individuals who had incident diabetes during follow-up were also older (p < 0.001), more likely to be men (p < 0.001), non-White (p = 0.010), had a higher frequency of hypertension (p < 0.001) and dyslipidaemia (p < 0.001) and higher BMI (p < 0.001) compared to those who did not develop diabetes during follow-up.
Characteristics of the study sample according to 1998 check-up evaluation glucose levels and incident diabetes mellitus.
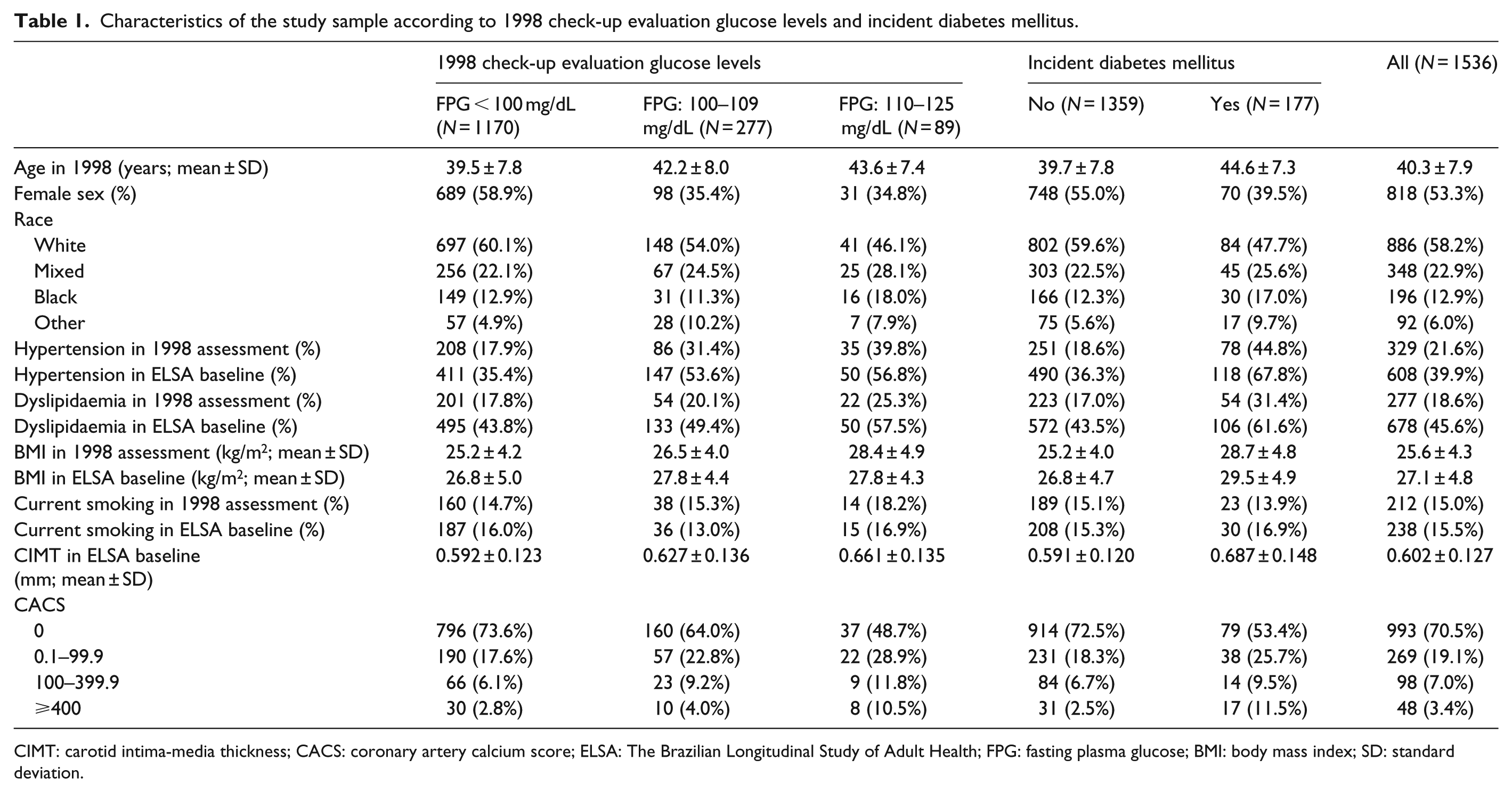
CIMT: carotid intima-media thickness; CACS: coronary artery calcium score; ELSA: The Brazilian Longitudinal Study of Adult Health; FPG: fasting plasma glucose; BMI: body mass index; SD: standard deviation.
Table 2 summarizes diabetes incidence rates. Incident diabetes occurred in 66 (5.6%), 63 (22.7%) and 48 (53.9%) individuals with normal FPG, impaired fasting glucose level 1 and level 2 in 1998, respectively. We found a higher risk of incident diabetes in individuals with impaired fasting glucose in all subgroups compared to individuals who were euglycemic in 1998, except for a non-significant positive association between impaired fasting glucose level 1 and incident diabetes in women (p = 0.094). Besides impaired fasting glucose, we also found age (p < 0.001), BMI in 1998 (p < 0.001), incident and prevalent hypertension (p = 0.027 and p = 0.021, respectively), incident and prevalent dyslipidaemia (p = 0.032 and p = 0.045, respectively) to be significant predictors for incident diabetes in the fully adjusted model with all individuals.
Incidence rates and hazard ratios (with respective 95% confidence intervals) for incident diabetes according to 1998 check-up evaluation glucose levels.
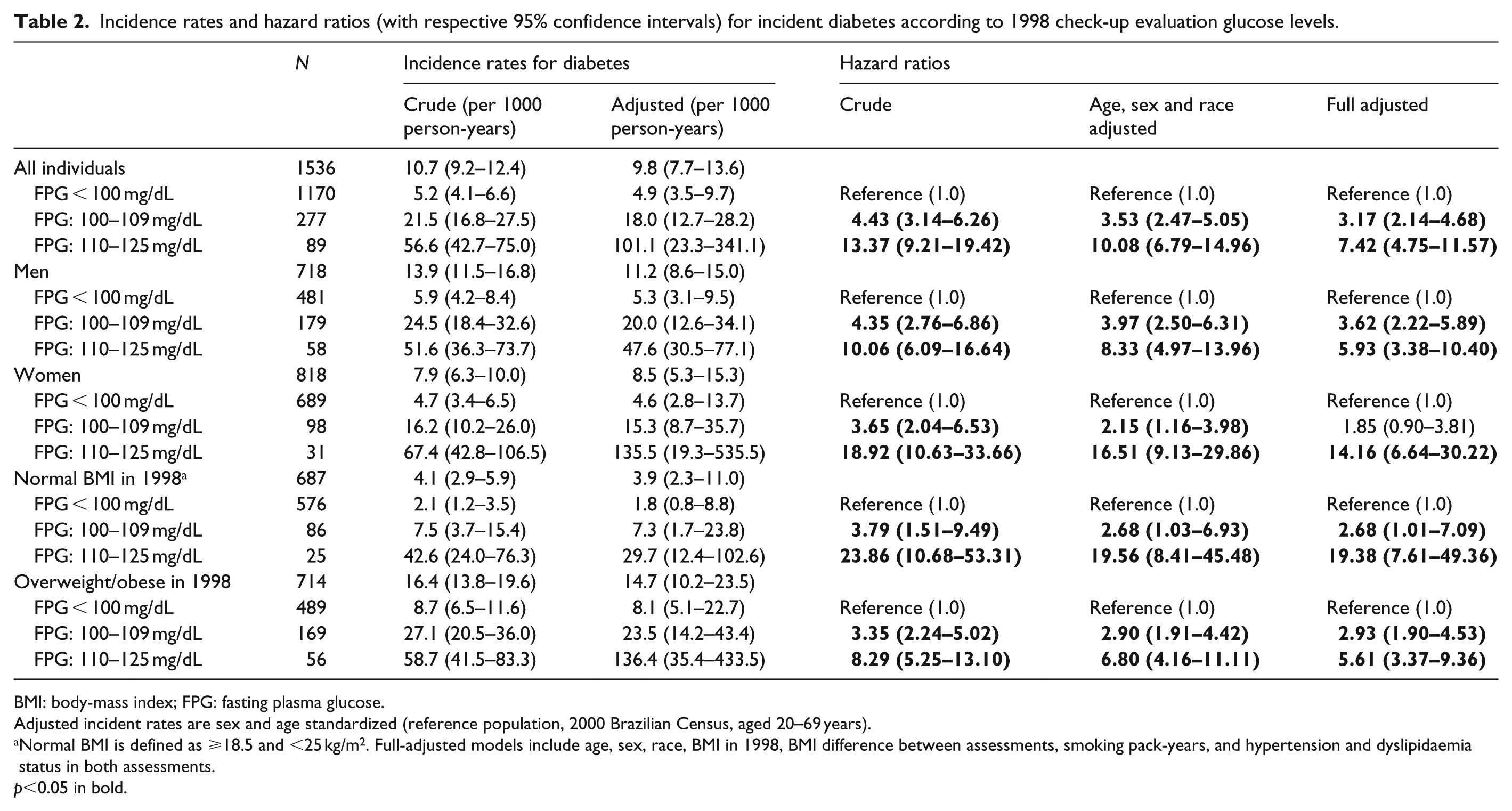
BMI: body-mass index; FPG: fasting plasma glucose.
Adjusted incident rates are sex and age standardized (reference population, 2000 Brazilian Census, aged 20–69 years).
Normal BMI is defined as ⩾18.5 and <25 kg/m2. Full-adjusted models include age, sex, race, BMI in 1998, BMI difference between assessments, smoking pack-years, and hypertension and dyslipidaemia status in both assessments.
p<0.05 in bold.
For the evaluation of subclinical atherosclerosis markers (CIMT and CACS), we excluded 9 (0.6%) individuals with prevalent clinical events or for whom we did not have complete information. For the remaining 1527 participants, we had valid CIMT imaging for 1481 (97.0%) and CACS for 1397 (91.5%) subjects. Nine individuals had a myocardial infarction or revascularization during the follow-up period. For the combined outcome of CACS ⩾400 and/or incident cardiovascular outcomes, we also included two participants with incident revascularization who did not perform CAC examination, resulting 1399 (91.6%) participants.
We found impaired fasting glucose level 2 in 1998 (Table 3) was a significant, independent predictor of higher CIMT levels in ELSA-Brasil baseline assessment (p = 0.030 in fully adjusted models), but not impaired fasting glucose level 1. The association between impaired fasting glucose level 1 and CIMT values vanished after adjustment for age, sex and race (p = 0.60). When we restricted these analyses to individuals who did not progress to diabetes, we found a significant association between impaired fasting glucose level 2 and higher CIMT after adjustment for age, sex and race [β = 0.037; 95% confidence interval (95% CI): 0.003–0.070; p = 0.033]. There was a non-significant association, in the same direction, in full-adjusted models (β = 0.030; 95% CI: −0.005 to 0.065; p = 0.093). Tables 4 and 5 show that glucose levels in 1998 were associated with both CACS ⩾400 points [odds ratio (OR): 3.47; 95% CI: 1.26–9.55] and the combined outcome of CACS ⩾400 points in ELSA-Brasil baseline and/or incident clinical events (OR: 3.17; 95% CI: 1.31–7.66) in age-, sex- and race-adjusted models. After full-adjustment, point estimate ORs still pointed towards positive associations. However, at least partially due to sample size limitations and consequent large CIs, in full-adjusted models statistical significance in both cases were borderline (p = 0.14 and p = 0.085, respectively).
Beta-coefficients (with 95% confidence intervals) from linear models for the association between CIMT values (in mm) and (1) fasting plasma glucose levels in 1998 and (2) incident diabetes during follow-up.
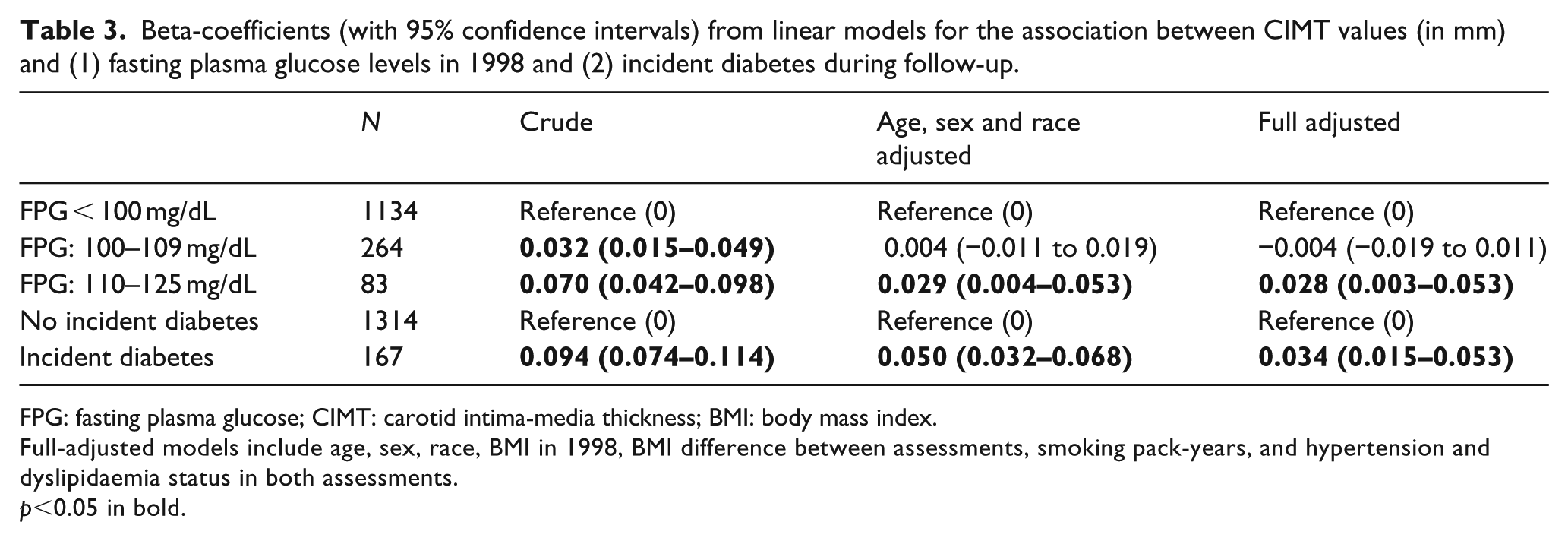
FPG: fasting plasma glucose; CIMT: carotid intima-media thickness; BMI: body mass index.
Full-adjusted models include age, sex, race, BMI in 1998, BMI difference between assessments, smoking pack-years, and hypertension and dyslipidaemia status in both assessments.
p<0.05 in bold.
Odds ratios (with 95% confidence intervals) from multinomial logistic models for the association between coronary artery calcium scores and (1) fasting plasma glucose levels in 1998 and (2) incident diabetes during follow-up.
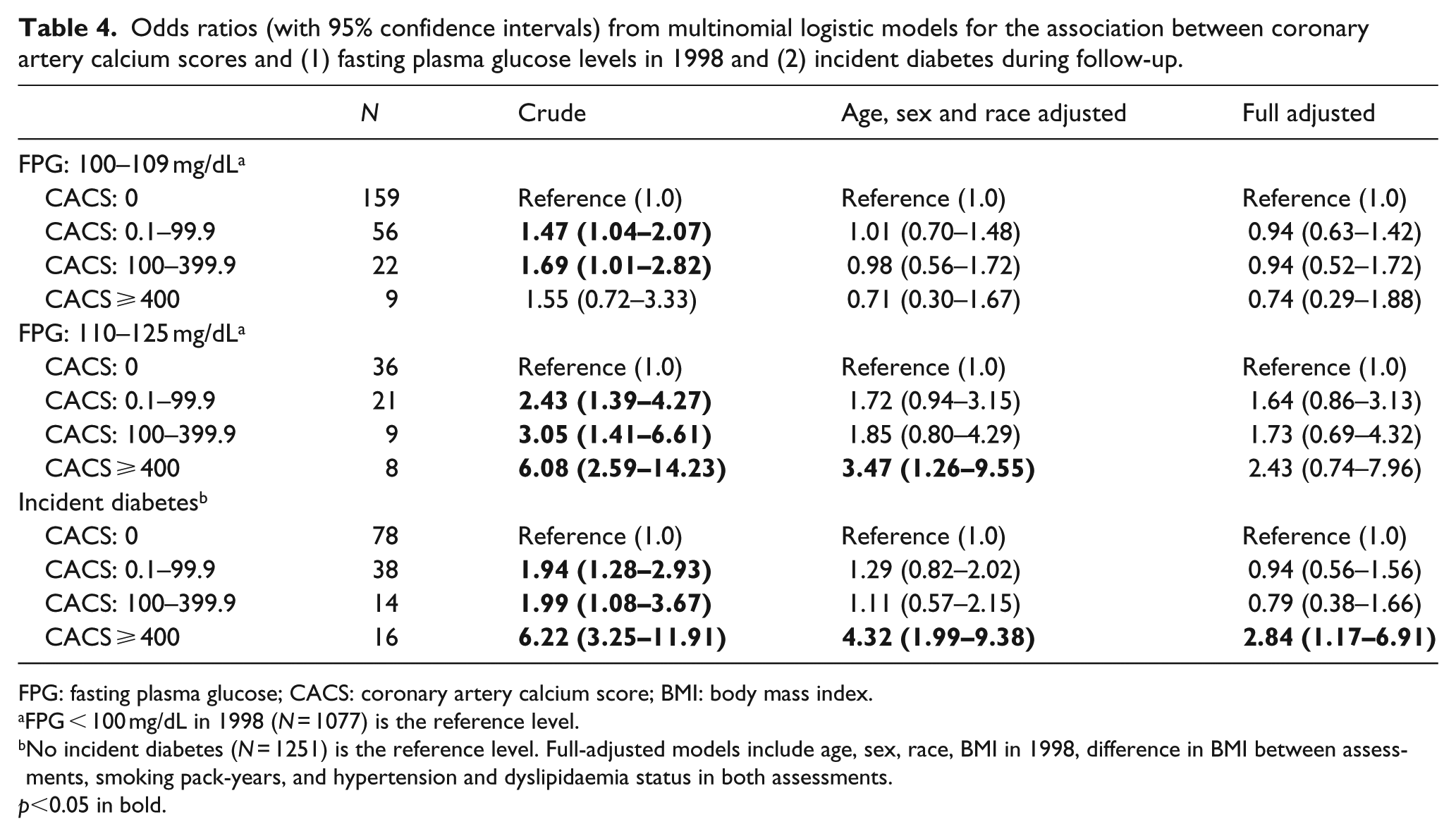
FPG: fasting plasma glucose; CACS: coronary artery calcium score; BMI: body mass index.
FPG < 100 mg/dL in 1998 (N = 1077) is the reference level.
No incident diabetes (N = 1251) is the reference level. Full-adjusted models include age, sex, race, BMI in 1998, difference in BMI between assessments, smoking pack-years, and hypertension and dyslipidaemia status in both assessments.
p<0.05 in bold.
Odds ratios (with 95% confidence intervals) from binary logistic models for the association between a CACS ⩾400 and/or incident cardiovascular events and (1) fasting plasma glucose levels in 1998 and (2) incident diabetes during follow-up.
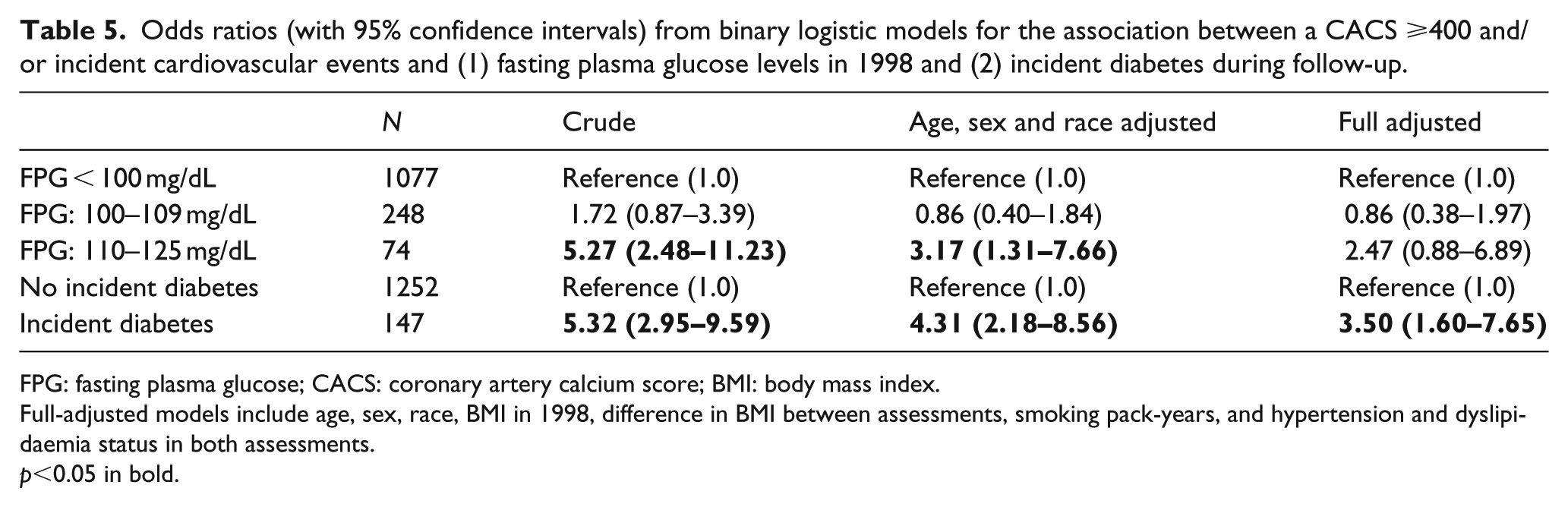
FPG: fasting plasma glucose; CACS: coronary artery calcium score; BMI: body mass index.
Full-adjusted models include age, sex, race, BMI in 1998, difference in BMI between assessments, smoking pack-years, and hypertension and dyslipidaemia status in both assessments.
p<0.05 in bold.
Regarding incident diabetes, we found that individuals who developed this condition during follow-up had higher CIMT levels than individuals without diabetes (Table 3) and had significantly higher odds of a CACS ⩾400 points in ELSA-Brasil baseline assessment (Table 4). Incident diabetes during follow-up was also associated with the combined outcome of CACS ⩾400 points and/or incident myocardial infarction or coronary revascularization (Table 5).
Discussion
We found evidence that impaired fasting glucose in 1998, especially in level 2, was a predictor of higher subclinical atherosclerosis measured by CIMT compared to euglycemic individuals. Incident diabetes was also associated with a higher subclinical atherosclerosis burden, quantified by both CIMT, CACS and the combined outcome of CACS ⩾400 points and/or incident myocardial infarction or coronary revascularization.
Although diabetes and impaired fasting glucose are frequent conditions in Brazil, 21 incidence data are scarce. Gimeno et al. 22 evaluated a sample of 253 Japanese-Brazilians aged 40–79 years, with normal glucose levels at baseline and found an incidence rate of diabetes of 30.9 per 1000 person-years. However, Japanese-Brazilians are a known high-risk population for diabetes, 23 but a small proportion of Brazilian population. Therefore, these very high rates may not reflect the whole country. Our diabetes age- and sex-adjusted incidence rates (9.8/1000 person-years) were similar to the rates found in another recent study in Tehran, which found an age-standardized rate of 9.9/1000 person-years. 24 It is well recognized that diabetes is more frequent than usual in Middle East countries, 25 and this may be true in our setting as well. 26
We found an independent association between impaired fasting glucose level 2 in 1998 and worse CIMT values in 2008–2010, suggesting a higher cardiovascular burden in these individuals. In models adjusted for age, sex and race, these individuals also had significantly higher odds to present with a CACS ⩾400 in ELSA-Brasil baseline although this association weakened in full-adjusted models. These findings are consistent to those reported by Moebus et al. 27 in the Heinz Nixdorf Recall Study. We also found a positive association between these FPG levels and the combined outcome of CACS ⩾400 in ELSA-Brasil baseline and/or incident clinical events in age-, sex- and race-adjusted models although this remained only with borderline significance in fully adjusted models, too. The EpiDREAM 12 is a cohort study of 18,990 individuals aged 30–85 years who had high risk of developing diabetes, defined by family history, ethnicity, gestational diabetes mellitus or abdominal obesity. In that study, the authors did not find a higher rate of cardiovascular events in non-diabetic individuals with glucose intolerance (hazard ratio (HR): 1.17; 95% CI: 0.89–1.53). Selection criteria for the EpiDREAM study, however, included additional risk factors for diabetes, and that cohort may, therefore, reflect a different population. In MESA study, Yeboah et al. 8 did not find a significant association between impaired fasting glucose and incident cardiovascular events in adjusted models either. However, in that study, impaired fasting glucose was defined as FPG levels between 100 and 125 mg/dL, and no analyses were presented using the subgroup with FPG levels above 110 mg/dL. It is reasonable to think that plasmatic glucose levels closer to diabetes diagnosis threshold may be more atherogenic. Park et al. 28 observed that the association between FPG and cardiovascular disease might have a nadir between 85 and 99 mg/dL. This is consistent to our findings of higher cardiovascular burden in individuals with impaired fasting glucose level 2. However, we did not find any positive associations between higher cardiovascular burden and impaired fasting glucose level 1 compared to euglycemic individuals. It is possible that we did not have power to detect weaker associations, as can be the case in this subgroup.
In our study, we also found a direct association between incident diabetes during follow-up and higher CIMT and CACS values with the combined endpoint of CACS ⩾400 points in ELSA-Brasil baseline and/or incident clinical events. Diabetic subjects have other cardiovascular risk factors, as hypertension, obesity and dyslipidaemia, in a higher proportion compared to the general population. Napoli et al., 29 in a study with 183 individuals, found higher CIMT values among participants with recently diagnosed diabetes compared to controls. Our findings allow an additional step forward, demonstrating that the association between incident diabetes and subclinical atherosclerosis remained significant after adjustment for other cardiovascular risk factors.
Our study has several strengths. This is a large sample of adults without diabetes in Brazil at baseline, with a long period between assessments. We used cardiovascular imaging techniques (CIMT and CACS) as an additional strategy to evaluate cardiovascular burden. This study also has some limitations. We did not use data about glycated haemoglobin or oral glucose tolerance test to define diabetes cases in 1998, as this was the real screening clinical scenario at that time. The exclusive use of FPG determinations in analyses was also adopted by others1,8,30 and, as one of our intentions was to estimate incidence rates in our sample, we considered important to use the same case definition strategy in both assessments. In addition, we cannot estimate incident CAC or CIMT progression in our sample, because these measurements were not performed in 1998. Clinicians received the results of blood tests for patient counselling, and this may have resulted in unequal chance of screening during the follow-up period. Although we do not have information about screening during follow-up, as all individuals in our sample underwent glucose measurement in ELSA-Brasil baseline, we were able to uncover underdiagnosed diabetes cases and minimize this bias. This is not a population-based study, so extrapolations to the general Brazilian or São Paulo population should be done carefully.
In conclusion, we found that, during the period between assessments, impaired fasting glucose in 1998 and incident diabetes were predictors of higher cardiovascular burden in the ELSA-Brasil baseline assessment, up to 12 years later. We also found high diabetes incidence rates in our sample in individuals with impaired fasting glucose in 1998. In addition, our results point towards higher diabetes incidence in São Paulo or Brazil compared to other populations.
Footnotes
Acknowledgements
The authors thank the ELSA-Brasil participants who agreed to collaborate in this study.
Declaration of conflicting interests
P.A.L. received honoraria (modest) for lectures: Abbott Brazil and Abbvie Brazil.
Funding
The ELSA-Brasil baseline study was supported by the Brazilian Ministry of Health and the Brazilian Ministry of Science and Technology (grants 01060010.00RS, 01060212.00BA, 01060300.00ES, 01060278.00MG, 01060115.00SP and 01060071.00RJ). The funding source had no involvement in study design, data collection, data analysis, article preparation and/or publication decisions.