
Abstract
Aim:
To examine the association of cardiovascular disease risk factors with and their cumulative effect on coronary artery calcium in hard-to-reach asymptomatic patients with diabetes.
Methods:
A total of 2563 community-dwelling asymptomatic subjects from Central Appalachia participated in coronary artery calcium screening at a heart centre. Binary variable was used to indicate that coronary artery calcium was either present or absent. Independent variables consisted of demographic and modifiable risk factors and medical conditions. Descriptive statistics and multinomial logistic regression analyses were conducted.
Results:
In total, 55.8% and 13.7% of study participants had subclinical atherosclerosis (coronary artery calcium ⩾1) and diabetes, respectively. The presence of coronary artery calcium was higher in subjects with diabetes (68.5%) than those without (53.8%). Compared to subjects without diabetes with coronary artery calcium = 0, obesity, hypertension, hypercholesterolaemia and smoking increased the odds of the presence of coronary artery calcium (coronary artery calcium score ⩾1) regardless of diabetes status; however, with larger odds ratios in subjects with diabetes. Compared to subjects without diabetes with coronary artery calcium score = 0, having 3, 4 and ⩾5 risk factors increased the odds of presence of coronary artery calcium in subjects with diabetes by 14.06 (confidence interval = 3.26–62.69), 32.30 (confidence interval = 7.41–140.82) and 47.12 (confidence interval = 10.35–214.66) times, respectively.
Conclusion:
There is a need for awareness about subclinical atherosclerosis in patients with diabetes and more research about coronary artery calcium in subpopulations of patients.
Keywords
Introduction
Diabetes1–3 is a strong risk factor for cardiovascular diseases (CVDs), which is the leading cause of death in the United States. 4 In patients with diabetes, CVD accounts for 65%–70% of deaths 5 and 85% of cumulative treatment costs for the initial 5 years following diagnosis. 6 In 2013, diabetes accounted for over 75,000 deaths in the United States 3 with the financial impact for 2012 estimated at US$245 billion in direct and indirect economic costs.3,7,8 There are nearly 30 million (9.3%) people in the United States diagnosed with diabetes. The prevalence continues to increase9,10 and is expected to reach one in three adults by 2050. 7 This increasing prevalence makes diabetes a major public health issue that requires both medical and policy attentions.
Diabetes is widely recognized as an independent risk factor for the development of clinical atherosclerotic CVD and was historically recognized as a cardiovascular risk equivalent,5,11 although not all patients with diabetes appear to be at equal risk. 12 The prevalence of diabetes in the United States is, likewise, not uniform as major disparities exist across population subgroups and geographic areas.13,14 Particularly, the Appalachian region is considered as the ‘Diabetes Belt’ due to a disproportionately high burden of the disease. 13
Of the 644 counties in the ‘Diabetes Belt’, 232 are in Appalachia, including a majority of the Central Appalachian counties.13,14 Studies have found that residents in distressed Appalachian counties had a 33% higher risk [95% confidence interval (CI), 1.10–1.60] of reporting diabetes than residents of non-Appalachian counties. 15 In addition, people in distressed or at-risk counties (the least economically developed) were diagnosed for diabetes at an earlier age, by 2–3 years, than in non-Appalachian counties. 16 Rural areas, such as Central Appalachia, have a higher diabetes prevalence relative to urban areas and the remainder of the United States as a whole,13,16 suggesting that research in subclinical atherosclerosis in patients with diabetes in this region is critical to achieve the Healthy People 2020 goals for reducing health disparities.
Coronary artery calcium (CAC) is a measure of subclinical atherosclerosis and has been validated as a predictor of cardiovascular events in asymptomatic patients, including those with diabetes.17–19 Studies have shown that asymptomatic patients with diabetes have increased prevalence and progression of CAC and a higher incidence of CVD as absolute values increase. 19 Both cross-sectional 17 and longitudinal20,21 studies have found that CAC scores were higher in men and women with diabetes across all age groups than those without diabetes and that CAC correlates with an increase in mortality for patients with diabetes. As such, it is reasonable to infer that using screening tools, such as CAC to identify subclinical atherosclerosis in regions with a high burden of diabetes, such as Central Appalachia, 13 may have positive health benefits. However, few studies evaluating the utility of CAC to detect and prevent CVD events in patients with diabetes in the Appalachian region exist,15,16 providing the basis for this study that assesses subclinical atherosclerosis in Central Appalachian subjects with diabetes.
This study aimed to (1) examine the association of traditional CVD risk factors with CAC status in a hard-to-reach diabetic population and (2) assess the association between the number of traditional CVD risk factors and CAC status in this population. While studies have examined the association between the traditional risk factors and cardiovascular outcomes, such as subclinical atherosclerosis (assessed as CAC), 22 little evidence exists on how multiple risk factors assessed collectively predicts CAC in patients with diabetes. Moreover, per our knowledge, no study has evaluated these outcomes in Central Appalachia, although the region constitutes the core of the ‘Diabetes Belt’ in the United States.13,14 Given the propensity for overt CVD in patients with diabetes,2,3 identifying the presence of subclinical atherosclerosis could lead to reclassification of patients with diabetes at risk for developing CVD for primary and prevention efforts. Thus, this study has the potential to inform policies and programmes targeting both diabetes and CVD in the Central Appalachian region, which would translate into clinical practice and improve CVD outcomes for residents of this region and other underserved populations.
Methods
Study population
The study population consisted of 3000 asymptomatic individuals from the Central Appalachian region of Southeast Kentucky, Western North Carolina, Northeast Tennessee and Southwest Virginia who had participated in a CAC screening programme in the largest cardiovascular centre in the region between August 2012 and December 2016. The recruitment, enrolment and data collection processes have been published in previous studies.23–25 In brief, adult patients visiting the cardiovascular centre who were free of any cardiovascular events were assessed for eligibility for the CAC screening. Eligible participants were adults aged 18 years or older who were referred by a physician. Self-referred individuals were also included if they met age eligibility of 45 years for males and 55 years for females. Potential subjects were informed about the study procedure and were assured about the confidentiality of the information collected. The participants completed an informed consent process before participating in the CAC screening. A self-administered questionnaire was used to collect additional information on lifestyle, risk behaviours, history of cardiovascular health and anthropometric measures. Ethical approval for this study was obtained from the institutional review board (IRB) of investigators’ institutions and the cardiovascular centre.
The data for the total population were examined for completeness. Subjects with missing information for either dependent or independent variables (n = 400) were excluded from the final analyses. In addition, non-Whites (n = 34), subjects with extreme recorded values for height (n = 1) and weight (n = 2) were excluded from the final study sample to reduce the effect of outliers. As a result, out of the 3000 initial subjects, the final analyses included 2563 (85.43%) subjects. Presence of diabetes was indicated by a self-reported question, with yes or no response, as to whether or not the subject had been informed by a physician or other healthcare professional that he or she has diabetes. Subjects were also asked whether or not they were currently taking any medication to control their diabetes in a yes/no fashion. Participants who answered yes to either question were assessed as having diabetes.
Assessment of CAC
The dependent variable was CAC score, which was ascertained using a 64-slice multi-detector computed tomography (CT) scanner based on a standard procedure and protocol for identifying and assessing CAC. 26 After the procedure, the patient was assigned a CAC score based on the Agatston scale, 27 which quantifies the volume of calcification (calculated as the product of the area of calcification per coronary tomographic segment and a factor rated 1 through 4 depending on the maximal X-ray density in that segment) and categorizes CAC based on the severity of risk for coronary artery disease (CAD) as 0 (zero; no plaque), 1–99 (mild plaque), 100–399 (moderate plaque) and ⩾400 (severe plaque). This standard Agatston scale was utilized to describe the extent of CAC in patients with or without diabetes. Due to small sample size for certain cells, presence of CAC was assessed as CAC ⩾1 (vs CAC = 0, indicating its absence) in bivariate and multivariable analyses.
Independent variables
Data on demographics, CVD risk factors and family history of CAD were obtained by self-administered questionnaire. The demographic data included age and sex. While age was assessed as a continuous variable, sex was categorized into male or female. Two modifiable risk factors (smoking, sedentary lifestyle) and three medical conditions (hypertension, hypercholesterolaemia and obesity) were obtained via questionnaire. The participants were asked whether or not they had been diagnosed and/or informed by their physicians if they had hypertension or hypercholesterolaemia and/or were currently using any medications to control these conditions. The participants responded as yes or no and this provided the information on clinical status of hypertension and hypercholesterolaemia, respectively. The participants were further asked about their behaviour related to smoking cigarettes (never smoker, current smoker or former smoker). During analysis, former smokers and current smokers were combined as smokers and the rest were evaluated as nonsmokers. Sedentary lifestyle was assessed by asking the participants whether or not they considered their lifestyle as sedentary; the responses were ‘yes/no’. The participants were also asked if they had a family history of CAD (yes/no). Self-reported height and weight was used to calculate the body mass index (BMI; kg/m2) and those with a BMI ≥30 kg/m2 were classified as ‘obese’. Finally, a cumulative risk factor index (RFI) was assessed based on the number of risk factors for CVD (i.e. obesity, hypertension, hypercholesterolaemia, smoking, sedentary lifestyle and family history of CAD); the presence of each calculated as 1 to assign an RFI ranging from 0 to 6. Only five subjects had all six risk factors; hence, participants with five or six risk factors were combined under the same group and were referred to as having ≥5 risk factors in the analysis.
Analysis
Descriptive statistics, including frequency and percentages, were used to describe the study population by the number of risk factors for CVD (0, 1, 2, 3, 4, ⩾5). Differences in sample characteristics, by number of risk factors, were tested using chi-square tests. Bivariate analyses were conducted to compare the prevalence of individual and multiple CVD risk factors by CAC status in subjects with diabetes and those without diabetes. For the regression analyses, a three-category nominal-dependent variable was created as follows: subjects without diabetes and CAC score = 0 (reference), subjects without diabetes and CAC score ⩾1, and subjects with diabetes and CAC score ⩾1. Adjusted multinomial logistic regression models were then constructed to determine the association between individual CVD risk factors and CAC status in patients with and without diabetes. Multinomial logistic regression analyses, adjusting for age and sex, were also carried out to determine the association between number of risk factors and CAC status in subjects with and without diabetes. The level of significance was set at p < 0.05. The data were analysed using SAS software, Version 9.2 (SAS Institute Inc., Cary, NC).
Results
Sample characteristics
A total of 2563 asymptomatic subjects were included in the final analyses. The majority (54.2%) were females and aged 46–74 years (85.7%; Table 1). In total, 35.9% were obese and 49.6% and 56.6% had hypertension and hypercholesterolaemia, respectively. Smokers accounted for 10.1% of the participants and 38.3% reported having a sedentary lifestyle. In total, 65.7% reported a family history of CAD. Of subjects identified as obese, 32.1% had four risk factors (Table 1). For those subjects classified as having hypocholesterolaemia, hypertension, sedentary lifestyle or a family history of CAD, 32.5%, 35.1%, 32.6% and 31.1%, respectively, had three risk factors (Table 1). Of subjects who smoked, 29.5% had three and 29.5% had four risk factors, accounting for 59% of these subjects in these two categories (Table 1). Overall, 13.7% of the subjects had diabetes (Table 2).
Prevalence and distribution of CAC and coronary artery disease risk factors (n = 2563).
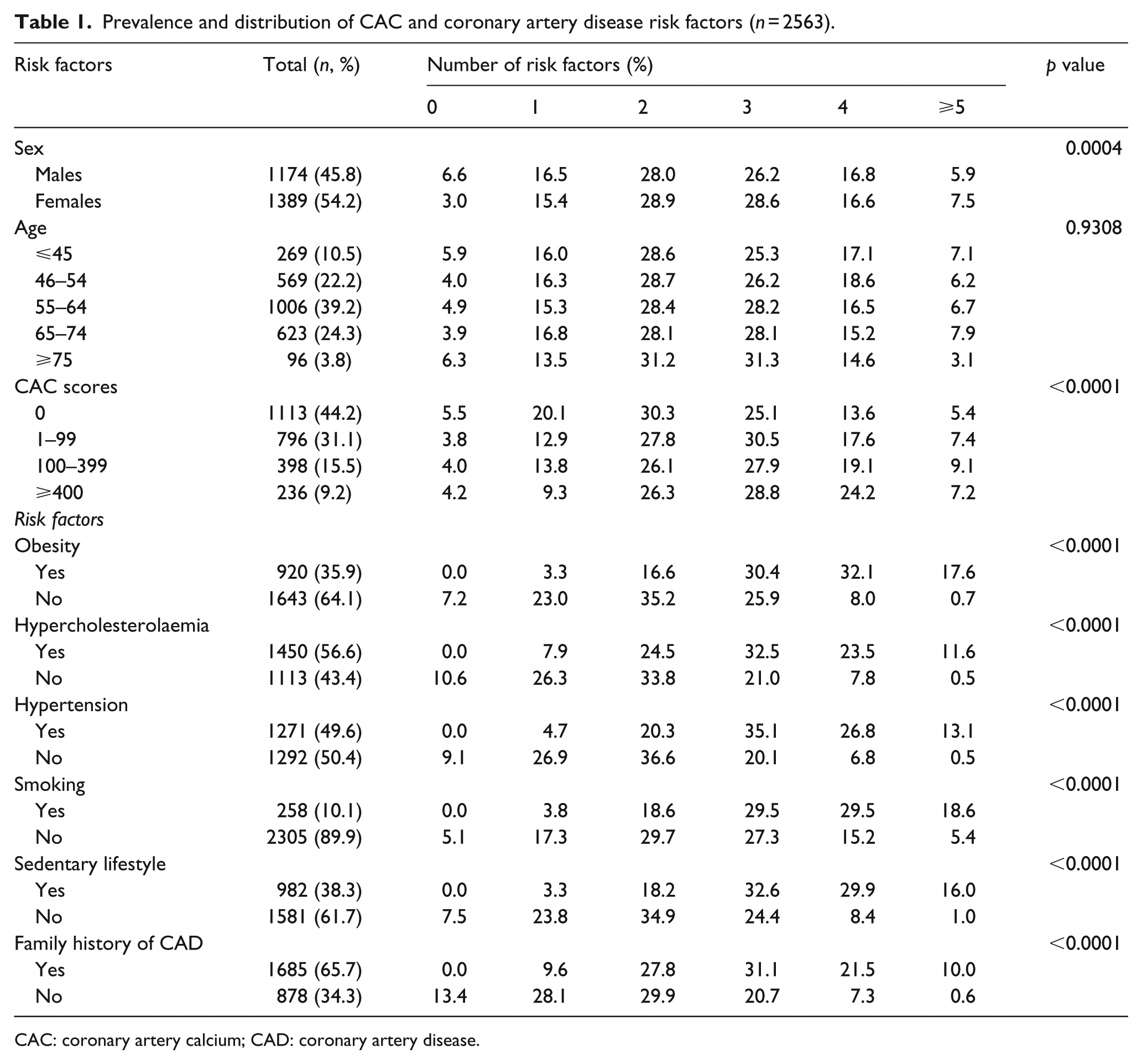
CAC: coronary artery calcium; CAD: coronary artery disease.
Prevalence of coronary artery disease risk factors by CAC status in subjects with and without diabetes (n = 2563).
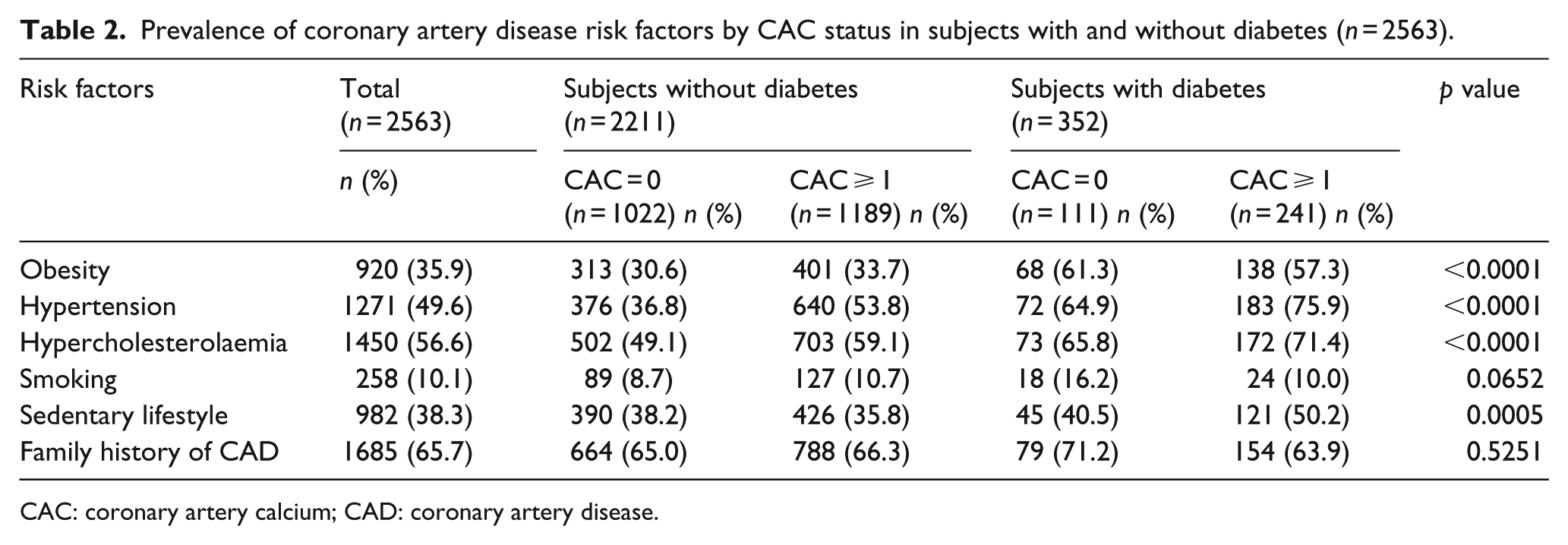
CAC: coronary artery calcium; CAD: coronary artery disease.
The presence and extent of CAC in study population
Approximately 55.8% of the participants had CAC score ⩾1 (Tables 1 and 2); the largest proportion constituted of those with mild plaque burden or CAC score = 1–99 on the Agatston Scale. 27 Among subjects without diabetes (n = 2211; 86.3%), 53.8% (n = 1189) had a CAC score ⩾1, and in the subjects with diabetes (n = 352; 13.7%), 68.5% (n = 241) had CAC score ⩾1. Except for smoking and family history of CAD, there was difference in the prevalence of CAC for subjects with or without diabetes across the other risk factors (obesity, hypertension, hypercholesterolaemia and sedentary lifestyle). Overall, 95.4% of all the participants had ⩾1 risk factors (Table 3). When comparing subjects with and without diabetes, 95.5% of those with no diabetes and CAC score ⩾1 had one or more risk factors, while 99.2% of subjects with diabetes and CAC score ⩾1 had one or more risk factors.
Prevalence of multiple coronary artery disease risk factors by CAC status in subjects with or without diabetes (n = 2563).
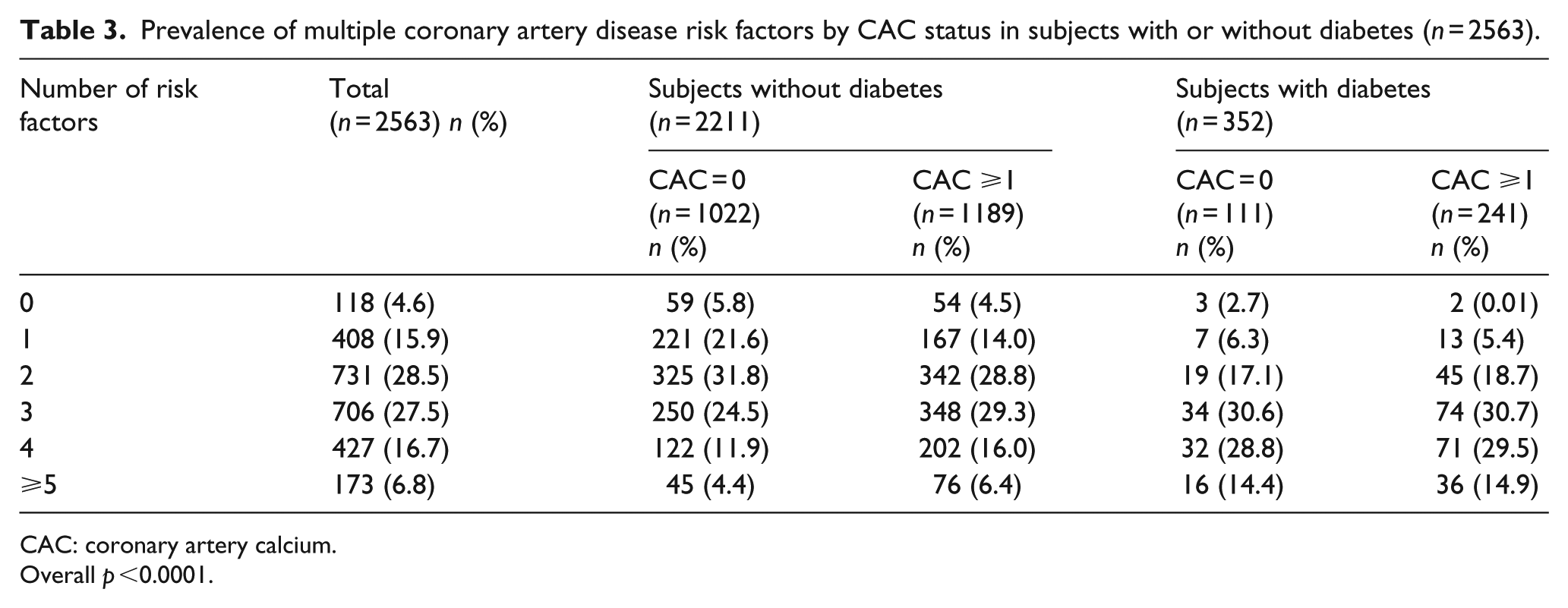
CAC: coronary artery calcium.
Overall p <0.0001.
Risk factors and cumulative number of risk factors in study population
In the multinomial logistic regression analyses, which controlled for age and sex, we examined the risk factors relative to their association with the presence of CAC in patients with or without diabetes (Table 4) and the number of risk factors present relative to the presence of CAC in patients with or without diabetes (Table 5). Except sedentary lifestyle and family history of CAD, the other risk factors (obesity, hypertension, hypercholesterolaemia and smoking) were associated with increased odds of the presence of CAC in both patients with or without diabetes, but those with diabetes generally had larger odds ratios (ORs). Sedentary lifestyle was only associated with an increased CAC score in the participants with diabetes. Hypertension was associated with the largest odds, almost 4.4-fold, of having subclinical atherosclerotic disease in patients with diabetes. Overall, compared to the healthy subjects, that is, those without diabetes and with CAC = 0, the odds for having CAC score ⩾1 in patients with diabetes were higher for all the examined risk factors, except smoking.
Multinomial logistic regression analyses for the association between coronary artery disease risk factors and CAC status in asymptomatic subjects with or without diabetes (n = 2563). a
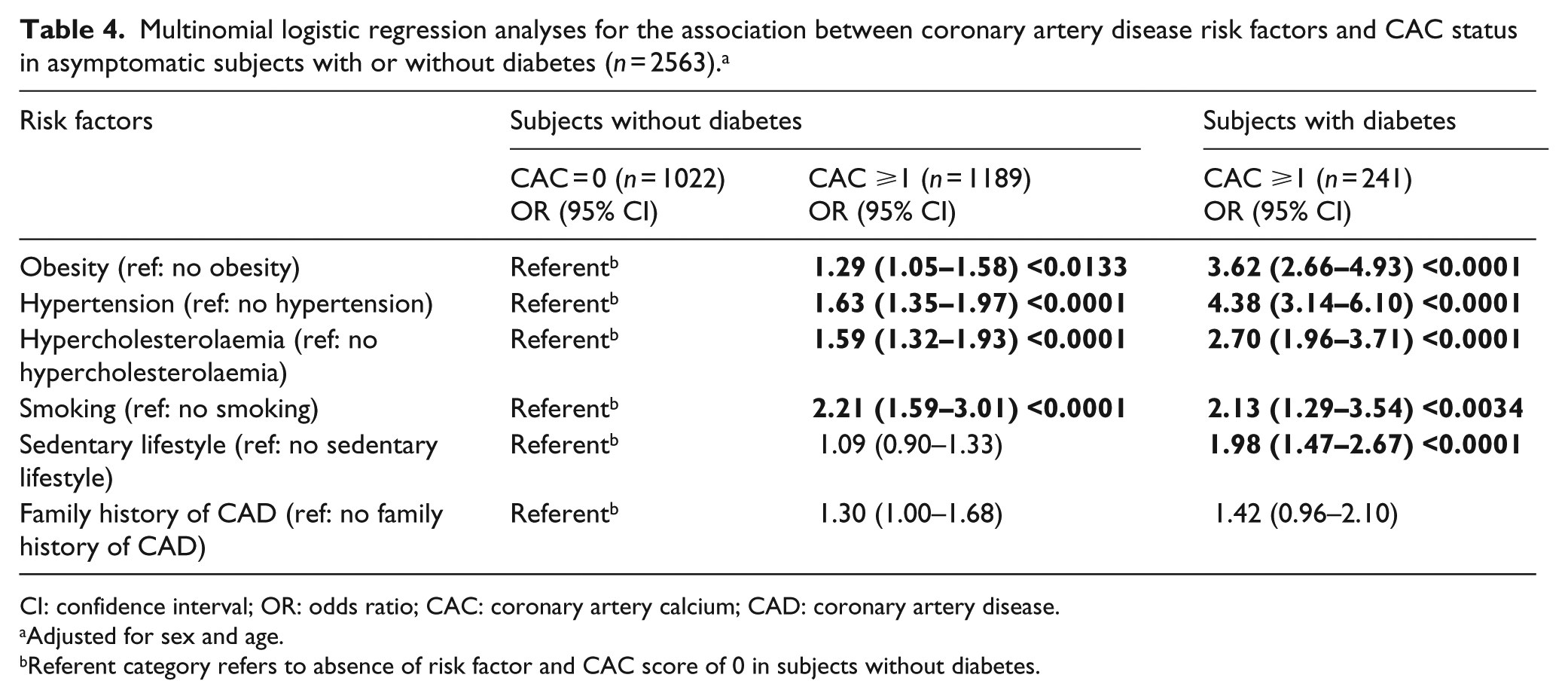
CI: confidence interval; OR: odds ratio; CAC: coronary artery calcium; CAD: coronary artery disease.
Adjusted for sex and age.
Referent category refers to absence of risk factor and CAC score of 0 in subjects without diabetes.
Multinomial logistic regression analyses for the association between number of coronary artery disease risk factors and CAC status in asymptomatic subjects with or without diabetes (n = 2563). a
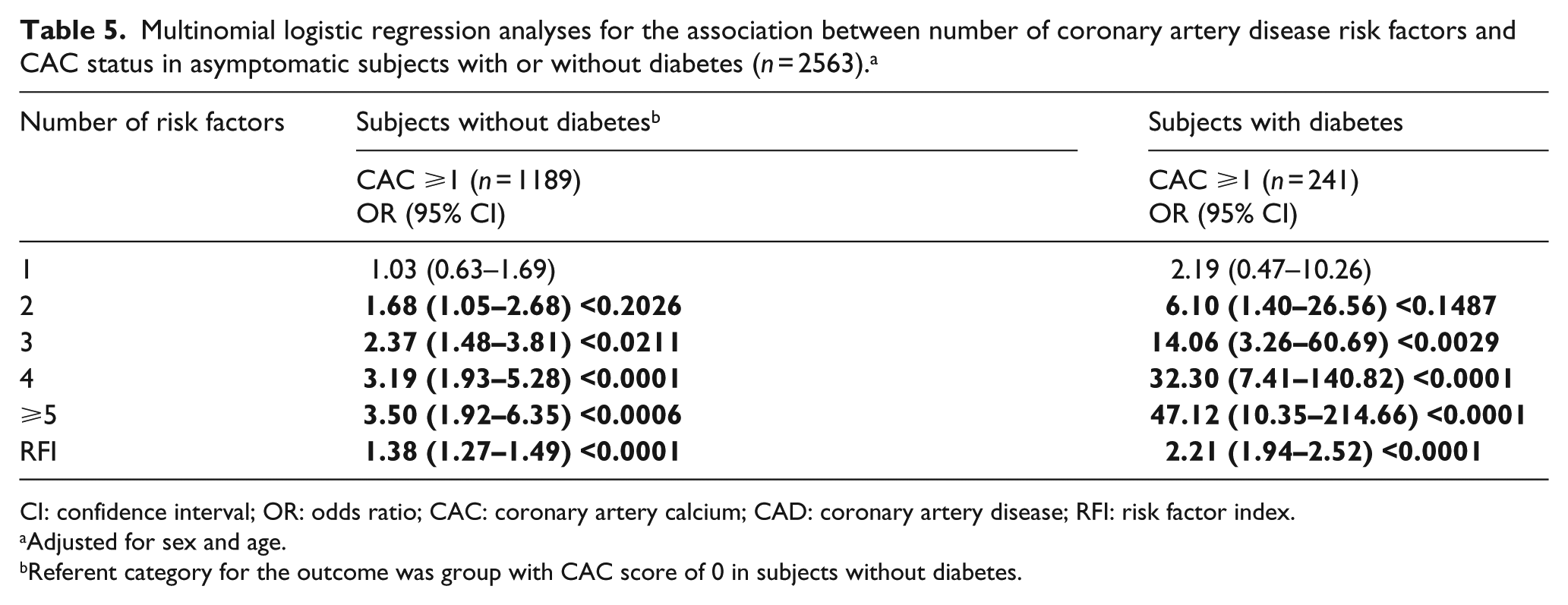
CI: confidence interval; OR: odds ratio; CAC: coronary artery calcium; CAD: coronary artery disease; RFI: risk factor index.
Adjusted for sex and age.
Referent category for the outcome was group with CAC score of 0 in subjects without diabetes.
Finally, Table 5 shows that as the number of risk factors increases, so does the odds for subclinical atherosclerotic disease, as defined by a CAC score ⩾1, in patients with diabetes. Compared to the reference group, the risk for subclinical atherosclerosis increased incrementally as the presence of two risk factors was associated with a greater than sixfold increased odds for high CAC score, while having five or more risk factors increased the odds by more than 47-fold. Generally, each increase in the number of likelihood factors was associated with an increased odds of having a CAC score ⩾1 in patients with and without diabetes.
Discussion
Although diabetes mellitus is an independent risk factor for developing atherosclerotic CVD,28,29 studies involving CAC in patients with diabetes in the ‘Diabetes Belt’ of the Central Appalachian region of the United States13,14 are sparse. In order to close this gap in CVD research, we conducted this study to examine the presence and the extent of CAC in asymptomatic patients with and without diabetes in this population. Overall, it was found that 55.8% of the total study population had a CAC score ⩾1, and in subjects with diabetes (13.7%), 68.5% had a CAC score ⩾1. While these findings are consistent with similar studies in this population,23,25,30 the proportion of patients with diabetes is higher than both the national average and the averages of the states comprising the Central Appalachia region (Kentucky, North Carolina, Ohio, Tennessee, Virginia and West Virginia). Thus, this study affirms the assertion that disparities in diabetes and CVD exist in this region and that using traditional risk factors and CAC scoring, health outcomes may be targeted for improvement in the Central Appalachian region and similar populations in the United States. 31
Six standard risk factors were examined in this analysis: three medical conditions (obesity, hypertension and hypocholesterolaemia); two behavioural risk factors (smoking and sedentary lifestyle); and one genetic factor (family history of CAD). While one in three of the study participants were obese, one in two had hypertension and hypocholesterolaemia. In terms of the behavioural factors, 1 in 10 were current smokers, while 1 in 3 reported a sedentary lifestyle. Approximately two in three of the study participants reported having a family history of CAD, mirroring the pervasiveness of CVD in the region. With the exception of smoking, the prevalence of all other CVD risk factors examined in this study population, when compared to the states comprising the Central Appalachian region and those of the entire United States, was higher. 32 The proportion of these risk factors was greater among patients with diabetes than those without. Specifically, as an example, the prevalence of obesity was 59% and 39%, respectively, among subjects with and without diabetes. Consistent with a previous study, 23 95.4% of the study population reported having ⩾1 risk factors, which is substantially higher than the national rate. 3
In the examination of the associations between the CVD risk factors and CAC, we identified significant independent associations between obesity, hypertension, hypercholesterolaemia, smoking, and sedentary lifestyle and subclinical atherosclerosis in patients with diabetes. These results are consistent with those in previous studies involving populations elsewhere in the United States.20,33,34 In a further analysis to delineate the associations between the number of risk factors and the presence of CAC, it was found that compared to health subjects with a CAC score = 0, having ⩾1 risk factors increased the likelihood of a CAC score ⩾1 in both subjects with and without diabetes. This was exhibited as a dose response with substantially higher ORs among subjects with diabetes. The subjects with diabetes had a much greater likelihood for subclinical atherosclerosis as having two risk factors was significantly associated with more than sixfold increased odds of having CAC score ⩾1, while having ⩾5 risk factors increased the odds for CAC score ⩾1 by more than 47-fold.
The dose–response relationship in subjects with diabetes, coupled with data from previous studies, lends credence to future exploration in this clinical area. Prior studies have demonstrated an association with the number of CVD risk factors along with CAC on all-cause mortality. 35 In addition, the number of risk factors is associated with the risk for CAC in asymptomatic patients. 23 Thus, this study provides evidence to support research involving CAC in populations with specific health conditions, namely, diabetes. Perhaps such an approach will provide information for early detection and treatment of CVD in high-risk population subgroups, ultimately helping to address the persistent CVD disparities in the United States.
These findings support the claim that the Central Appalachian region is not only disproportionately burdened with CVD outcomes such as subclinical atherosclerosis, that is, CAC, but also the risk factors for CVD, supporting and reinforcing previous findings from earlier studies.23,25,30 Furthermore, these findings highlight the necessity for research to understand why individuals are predisposed to a disproportionately high prevalence of these CVD risk factors while engaging in individual- and population-based interventional programmes to address these risk factors, and in turn the overall health, of this and similar regions.
The higher proportions of these risk factors in subjects with diabetes suggest that more aggressive efforts to address CVD risk is warranted in this high-risk subset of patients. Given the increased prevalence of diabetes in this and similar regions, not only are additional programmes needed but these programmes should focus not just on diabetes but in the overall reduction of risk factors for CVD, the primary threat to this vulnerable population. 2 Furthermore, consistent with American College of Cardiology and American Heart Association guidelines, CAC screening could potentially be incorporated into the standard care of patients with diabetes in the region, with a Class IIA recommendation.19,22,33 In fact, some leading experts feel this is an underutilized resource that could greatly enhance the ability to identify high-risk patients, such as those requiring statin therapy for primary prevention, which is directly translatable to our high-risk population.36,37
Moreover, previous studies identified that the rate of adherence to medications is low in patients with diabetes. 38 Not only does CAC provide objective motivation for patients to adhere to prescribed medical treatments, but it also provides a visual representation of the level of disease in their coronary arteries. Future research in this vein would follow best practice recommendations for strategies to improve medication adherence among patients with diabetes and could be significantly useful for a region with higher levels of poor health literacy, such as Central Appalachia. This is supported by previous studies that indicate the protective effect of CAC visualization in lifestyle modification.3,39 Medication adherence among patients with diabetes is critically important because it not only improves blood glucose, a measure many patients focus on today, but also improves the long-term CVD health outcomes and saves healthcare costs. 40 In the United States alone, poor medication adherence contributes to 33%–69% of medication-related hospital admissions and nearly US$100 billion in annual costs. 40
The results of this study should be interpreted with recognition of certain limitations. First, cross-sectional data were utilised for this study, which precludes claims of causation. Second, several measures were self-reported, including weight and height; hence, they were subject to recall and social desirability biases. For example, asking study subjects to report whether they consider their lifestyle as sedentary could lead to a major bias due to under-reporting. Third, the study examined only individual risk factors; however, previous studies suggest that factors such as social determinants and neighbourhood or environmental characteristics affect CVD outcomes, including subclinical atherosclerosis.30,41 Fourth, CAC score was collapsed into two categories which may lead to loss of information. However, categorizing CAC status as a binary variable has been successfully done in multiple studies23,25,30,42,43 and facilitates interpretation of results. Nevertheless, the study adopts a unique approach that examined the effects of traditional risk factors and the cumulative number of these risk factors present on the outcome of subclinical atherosclerosis in subjects with and without diabetes, as assessed by CAC scoring. With further research, this could provide guidance for not only early detection and treatment of CVD but also addressing the CVD disparities in population subgroups.
Conclusion
Diabetes is a major risk factor for CVD and this study examined the presence and extent of subclinical atherosclerosis (assessed as CAC) in asymptomatic subjects with diabetes in the Central Appalachian region, part of the ‘Diabetes Belt’ of the United States. In total, 13.7% of the total population comprises patients with diabetes. While the prevalence of subclinical atherosclerosis was 55.8% in the total population; it was substantially higher at 68.5% among subjects with diabetes. All risk factors examined were associated with an increased likelihood of subclinical atherosclerotic disease in this asymptomatic population with diabetes, except family history of CAD. In addition, the presence of subclinical atherosclerotic disease in these subjects with diabetes positively correlated with the number of CVD risk factors. While this study affirms disparities in CVD for residents of Central Appalachia, it also suggests the need for awareness about subclinical atherosclerosis (i.e. CAC) in patients with diabetes and more research about CAC in subpopulations of patients.
Footnotes
Acknowledgements
We would like to thank the Colleges of Public Health, Medicine, and Pharmacy at East Tennessee State University (ETSU) for supporting the ETSU Cardiovascular Research Group on this project. We would also like to thank Wellmont CVA Heart Institute (now Ballad Health) for providing the researchers with the electronic medical record data. We thank the Office of Research and Sponsored Program and the ETSU Office of Equity and Diversity for providing the funds to support data cleaning and management and research assistants. Finally, we would like to say special thanks to all colleagues and graduate assistants who reviewed different versions of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.