
Abstract
Objective:
Obesity-related atherosclerosis is a systemic disease with a background connected to multiple metabolic-neurohumoral pathways. The leptin/adiponectin ratio has been suggested as an atherosclerotic marker in obese patients. The aim of this study was to assess (1) the significance of the L/A ratio in overweight subjects, (2) the relation with anthropometric/metabolic parameters and (3) gender difference.
Method:
The study included 80 adult males and females, overweight, non-diabetic patients. Biochemical blood analysis and anthropometric and cardiovascular measurements were performed. Serum leptin levels were measured with a radioimmunoassay test and total adiponectin levels with enzyme-linked immunosorbent assay. Leptin/adiponectin ratios were calculated as ratios between total serum concentrations of leptin and adiponectin.
Results:
Differences between leptin, adiponectin serum levels and leptin/adiponectin ratios are presented in overweight persons, where females have a significantly higher leptin/adiponectin ratio than men (p < 0.001). In men, the leptin/adiponectin ratio showed a positive correlation with total cholesterol levels (p = 0.011), low-density lipoprotein (p = 0.013) and triglycerides (p = 0.032). In females, the leptin/adiponectin ratio correlated with anthropometric parameters of visceral obesity: waist circumference (p = 0.001) and waist-to-hip ratio (p = 0.025).
Conclusion:
The leptin/adiponectin ratio could represent an atherosclerotic risk marker of the early stage of obesity. Gender plays a significant role in pathophysiological changes, with different clinical manifestations, where sex hormones have a crucial effect on neurohumoral adipose tissue activity.
Introduction
Obesity-related atherosclerosis is caused by multiple metabolic changes that result in acute and chronic cardio-cerebro-vascular diseases, whereby inflammation and endothelial dysfunction play a key role.1–3 The metabolic profile is associated with the presence of dyslipidemia, diabetes mellitus and hypertension, along with neurohumoral mechanisms caused by adipokines disbalance and cytokines activation. These factors, both individually and combined, have a great proatherogenic potential and each patient’s atherosclerotic risk profile is unique. 1
Adult obesity is characterized by adipocyte hypertrophy. More leptin and less adiponectin are secreted, whereby leptin could accelerate and adiponectin restrain the development of atherosclerosis 4 acting directly on vascular cells, 5 which makes them important mediators linking adiposity and atherosclerosis in the adipo-vascular axis. 5 Both leptin and adiponectin could be individually associated with the development of atherosclerosis via plaque formation and progression and plaque rupture and thrombosis,2,3 and their combination might result in more atherosclerotic manifestations than their individual activity. 6 The leptin/adiponectin (L/A) ratio is a new surrogate marker for atherosclerosis in subjects with obesity and type 2 diabetes mellitus.4,6 It is a better parameter in monitoring for metabolic disorders 7 such as (1) atherosclerotic index in patients with diabetes type 2 regardless of body weight and obesity level,4,7 (2) parameter for insulin resistance and 7 (3) screening for vascular risk and endothelial dysfunction.8,9
From the clinical point of view, obesity-related atherosclerosis is characterized by insulin resistance, higher visceral fat, and dyslipidemia, where a high L/A ratio and higher triglyceride serum levels may be additional obesity risk factors regardless of waist circumference and body mass index (BMI). 10 Considering the relation between L/A ratio and an index of atherosclerosis in obese subjects with diabetes, the aim of this study was to examine the value of L/A ratio in overweight patients without diabetes, along with the other components of the metabolic syndrome, and to determine whether there are gender-based differences.
Materials and methods
The study included 80 adult, hypertensive, overweight subjects (body mass index (BMI): 25–29.99 kg/m2), who were hospitalized at the Department for Cardiovascular Disease, Osijek University Hospital because of myocardial infarction. All involved subjects voluntarily agreed to participate in the study and gave their written consent. The study was authorized by the hospital ethics committee.
Inclusion criteria for this study were adult overweight subjects of both sexes, no diabetes mellitus and normal renal function. Included females were postmenopausal and were not taking hormonal replacement therapy. Other presented conventional risk factors were hypertension, dyslipidemia and smoking. Exclusion criteria for the study were glucose intolerance and diabetes, renal failure, BMI above 30 kg/m2 or less than 25 kg/m2, systolic dysfunction [left ventricular ejection fraction (LVEF) < 55%], history of previous myocardial infarctions and/or acute stroke.
Medical history, physical examination, biochemical and anthropometric measurements, monitored values of blood pressure, transthoracic echocardiography and coronary angiography by a standard procedure were performed in all patients.
Leptin and adiponectin blood samples were taken from all subjects in the morning at the same time. Serum leptin levels were measured using the radioimmunoassay (RIA) method and total circulating adiponectin serum levels were measured using enzyme-linked immunosorbent assay (ELISA) for quantitative determination of human adiponectin (Biosource Europe S.A, Belgium). L/A ratio was calculated as the ratio between total serum concentrations of leptin and adiponectin.
Statistical analysis
All statistical tests were two-sided and carried out to a significance level (p) of 0.05. Distribution normality for L/A level was tested using Shapiro–Wilk test. According to the results of Shapiro–Wilk test, the nonparametric Mann–Whitney test was used. To verify relationship between univariate relations, we used the Spearman method. Data were prepared for analysis in Microsoft Excel 2003. Statistical analysis was done by SPSS 15.0 for Windows Evaluation Version and Statistica 7.1.
Results
Subjects in both groups were Caucasian, overweight and present with conventional risk factors, normal renal function and no other significant co-morbidities. The average age in the group of male subjects was 59.47 ± 7.60 years, while it was 64.10 ± 7.59 years in female subjects.
According to the results, leptin and adiponectin levels varied in males and females.11,12 Leptin levels were statistically significantly higher in females compared to the male group (p < 0.001); also, total adiponectin levels were higher in the female group than in the male group (p = 0.006). According to these results, the L/A ratio showed a gender-related difference, where the L/A ratio is lower in men than in women (p < 0.001; Figure 1). Statistically significant correlation was found between the L/A ratio and metabolic parameters in male subjects [total cholesterol (p = 0.011), triglycerides (p = 0.032) and low-density lipoprotein (LDL; p = 0.013)], but there was no significant correlation with glucose level in this sample size. The results suggest that correlation might be positive in a study with a larger sample. In females, the L/A ratio significantly correlated with anthropometric parameters [waist circumference (p = 0.001) and waist-to-hip ratio (p = 0.025)]. In both groups of patients, the L/A ratio did not correlate with weight in both genders [male (p = 0.380) and female (p = 0.350)] or with BMI [male (p = 0.091) and female (p = 0.080)].
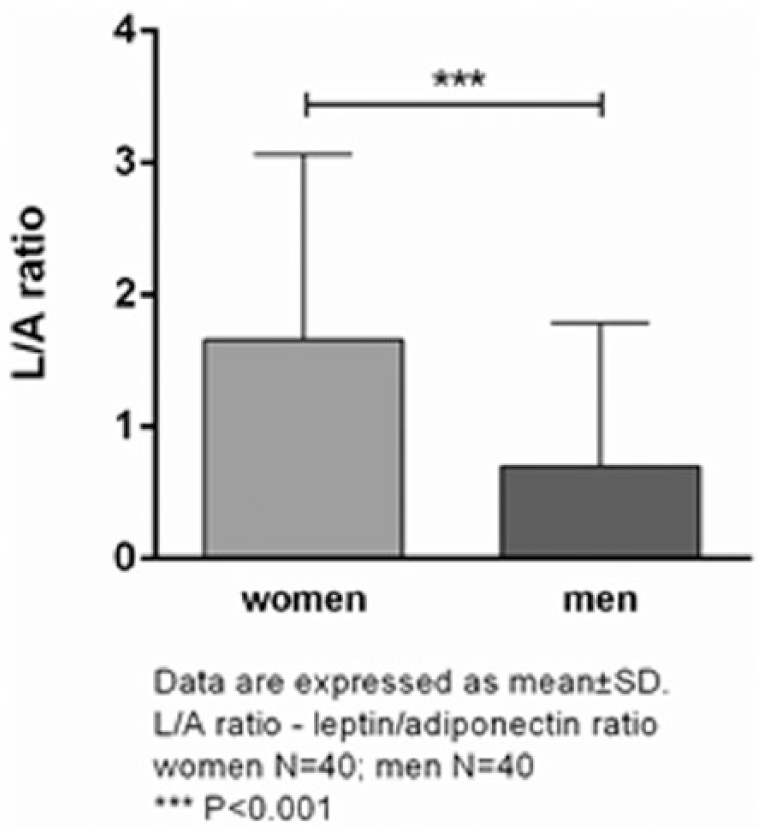
L/A ratio and gender difference in overweight.
Discussion
Visceral type of obesity is an independent risk factor for atherosclerosis, but the personal profile is unique as a result of the complexity of included metabolic, genetic and environmental risk factors and influences. Neurohumoral mechanisms that link atherosclerosis with obesity are adipocytokines production, endothelial dysfunction and chronic inflammation. Regarding opposite effect of leptin and adiponectin on vascular endothelium, angiogenesis, inflammatory and thrombogenic state in obesity, it is logical to consider the L/A ratio as a possible marker for atherosclerosis.
There are still unanswered questions: can the L/A ratio serve as an early atherosclerotic marker in the pre-stage of obesity or in patients without diabetes mellitus? What is the clinical relevance of the L/A ratio and is there a gender-related difference? Data in this area are very scarce, especially if one takes into account differences based on race and ethnicity.
Results from our study confirm the significance of gender differences of the L/A ratio and its correlation with anthropometric and metabolic profiles. The L/A ratio is not related with BMI or weight measurements, but in females it is related with visceral type of obesity, while this is not evident in males in this early stage of obesity. This is probably caused by hormone-related differences in body structure and distribution of adipose tissue in men and women, especially in overweight persons since it is not clear if significant changes in synthetic activity of adipose tissue start at this obesity level. 4 It is possible that visceral obesity is manifested earlier in women than in men at lower levels of obesity. Also, in early stages of obesity, adipose tissue is less active as a possible consequence of low-grade adipokines inflammation.7,8
However, the L/A ratio correlates with lipidogram components in men, while there is no correlation in women at this level of obesity. The reason for this might be a still unexplained activity of fat cells, as well as volume of visceral tissue. There is positive correlation between L/A ratio and glycaemia at low levels of obesity, when glucose levels in blood are still normal, both in men and in women, which might indicate that there is significant correlation between the L/A ratio and hyperglycaemia and other disorders of glucose metabolism.
Conclusion
Gender-related differences of the L/A ratio suggest that sex hormones might influence body adipose tissue composition and affect certain metabolic parameters. This could be a result of sex hormone–induced changes of the mechanisms of adipokine synthesis and consequent changes of adipokine activity as signalling factors. Overweight is a warning sign in cardiovascular risk assessment as well as a risk factor for the development of atherosclerosis. Since obesity has ceased to be only a lifestyle consequence and has become a serious disease, early detection of risk factors for its development, recognizing the disease in its early stages and developing strategies for its prevention and treatment have become a necessity. Further research in this area is needed, especially of the influence of sex hormones on obesity development and influence on metabolic changes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.