
Abstract
Objective
Pregnancy is characterized by progressive insulin resistance. The present study evaluated whether the adiponectin/leptin ratio is associated with insulin resistance in pregnancy, since this ratio has been shown to be associated with insulin resistance in obesity, type 2 diabetes mellitus, metabolic syndrome and polycystic ovary syndrome.
Methods
In this cross-sectional study, adiponectin and leptin concentrations were measured in pregnant women using enzyme-linked immunosorbent assays. Insulin resistance was assessed using the homeostasis model assessment of insulin resistance (HOMA–IR).
Results
Mean ± SD age of the participants (n = 74) was 30.76 ± 4.27 years, mean ± SD gestational age was 26.81 ± 3.52 weeks and median body mass index (BMI) before pregnancy was 22.68 kg/m2 (interquartile range 20.75–26.79 kg/m2). There was a significant correlation between the HOMA–IR and leptin concentration, but not between the HOMA–IR and adiponectin concentration. There was a significant inverse correlation between the HOMA–IR and adiponectin/leptin ratio. The adiponectin/leptin ratio was inversely correlated with BMI before pregnancy.
Conclusion
The adiponection/leptin ratio inversely correlates with HOMA–IR in pregnancy.
Introduction
Pregnancy is characterized by varying degrees of progressive insulin resistance. 1 The homeostasis model assessment of insulin resistance (HOMA–IR) represents a simple and noninvasive method for estimating insulin resistance during pregnancy, using fasting glucose and insulin concentrations. 2
Adiponectin and leptin are two adipocyokines that have been shown to be associated with insulin resistance.3,4 Adiponectin has insulin-sensitizing, anti-inflammatory and antiatherogenic properties; 5 leptin plays an important role in glucose metabolism and acts as a metabolic and neuroendocrine hormone. 6 Decreased adiponectin and increased leptin concentrations are associated with insulin-resistant states.3,7 Several studies have reported associations between adiponectin/leptin ratios and states with increased insulin resistance.7–12 A decreased adiponectin/leptin ratio has been shown to be associated with insulin resistance in obesity,7,8 type 2 diabetes mellitus,9,10 polycystic ovary syndrome 11 and metabolic syndrome. 12
The significance of the adiponectin/leptin ratio as a potential noninvasive biomarker of insulin resistance in pregnancy remains unknown, however. Thus, the present study evaluated whether the adiponectin/leptin ratio was associated with insulin resistance in pregnancy.
Subjects and methods
Study Population
This was a cross-sectional study conducted between May 2007 and January 2009. Women who attended the outpatient clinic at the University Medical Centre Ljubljana, Ljubljana, Slovenia, as part of a standard screening procedure during pregnancy, were enrolled sequentially. Exclusion criteria were: concomitant disease or treatment; use of medications that interfere with insulin resistance; history of previous diabetes mellitus; aged <18 or >45 years.
For each participant, data regarding age, week of gestation and prepregnancy weight were collected. Prepregnancy data were collected during routine health checks and were available for all participants. Body height and weight were measured, and body mass index (BMI) before and during pregnancy were calculated.
The study protocol was approved by The National Medical Ethics Committee of the Republic of Slovenia, Ljubljana, Slovenia, and the study was conducted in accordance with the Declaration of Helsinki and its amendments. Each study participant provided written informed consent.
Glucose, Insulin, Adiponectin and Leptin Measurements
For each participant, fasting blood samples were collected into one ethylenediaminetetra-acetic acid (EDTA)-coated tube (1.8 mg of EDTA/ml of blood) and one tube with no additives. Commercially available blood-collection tubes were used (Becton, Dickinson and Company, Plymouth, UK). The blood samples were centrifuged at 2800
Plasma glucose concentrations were determined using the standard glucose oxidase method (Beckman Coulter Glucose Analyzer; Beckman Coulter, Brea, CA, USA), according to the manufacturer’s instructions. Serum insulin concentrations were measured using a commercially available Immulite® 2000 analyser and a chemiluminescent immunoassay kit (Immulite® 2000 Insulin; Siemens Healthcare Diagnostics, Camberley, Surrey, UK), according to the manufacturer’s instructions. Plasma adiponectin and serum leptin concentrations were measured using commercially available enzyme-linked immunosorbent assay kits (Adiponectin full-length + globular EIA [44-ADPHU-E01-GLOB] and Leptin EIA [11-LEPHU-E01]; both from ALPCO Diagnostics, Salem, NH, USA), according to the manufacturer’s instructions. Insulin resistance was assessed using HOMA–IR, where HOMA–IR = (fasting insulin [mIU/l] x fasting plasma glucose [mmol/l])/22.5. A HOMA–IR score of 2.0 was considered as the cut-off point for insulin resistance. 2
Stastistical Analyses
The Shapiro–Wilk test was used to assess normality or log normality of the data. Data for normally and log-normally distributed parameters were presented as mean ± SD. Results for not-normally distributed parameters were presented as median and interquartile range. The correlation between numerical variables was estimated using Pearson’s correlation coefficient. Statistical analyses were performed using R language for statistical computing (version 2.8.1). 13 A P-value of <0.05 was considered statistically significant.
Results
Demographic and clinical characteristics of pregnant women assessed for a correlation between the adiponectin/leptin ratio and insulin resistance (n = 74).
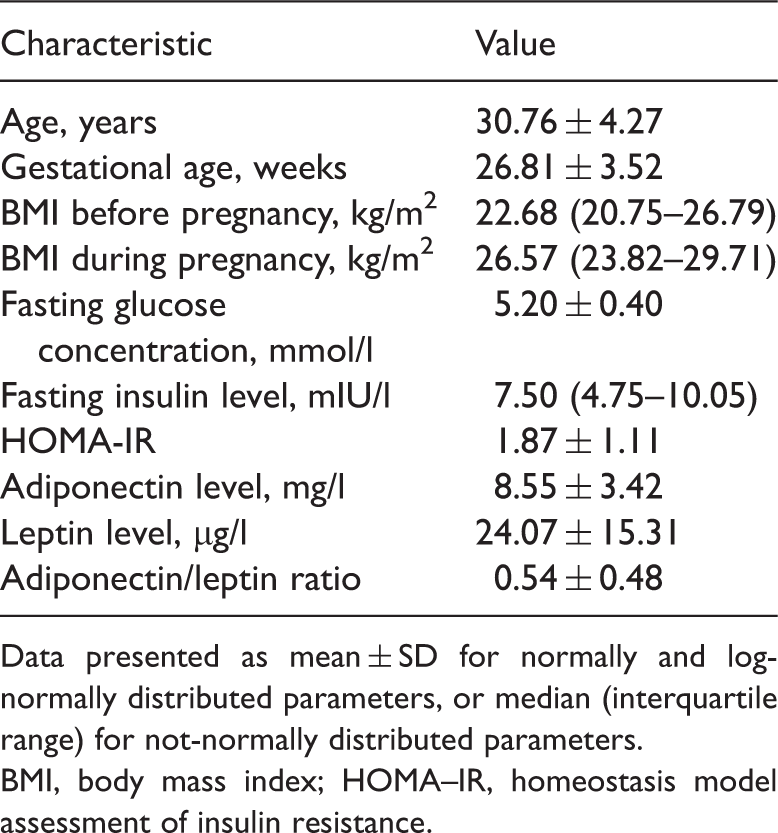
Data presented as mean ± SD for normally and log-normally distributed parameters, or median (interquartile range) for not-normally distributed parameters.
BMI, body mass index; HOMA–IR, homeostasis model assessment of insulin resistance.
There was a significant correlation between the HOMA–IR and serum leptin concentrations (r = 0.42, 95% confidence interval (CI) 0.21, 0.59; P < 0.01), but no correlation was detected between the HOMA–IR and plasma adiponectin concentration (r = −0.19, 95% CI –0.40, 0.04). There was a statistically significant inverse correlation between the HOMA–IR and adiponectin/leptin ratio (r = −0.42, 95% CI –0.60, −0.22; P < 0.01 [Figure 1]) and between the adiponectin/leptin ratio and BMI before pregnancy (r = −0.41, 95% CI –0.58, −0.20; P < 0.01) Correlation between the homeostasis model assessment of insulin resistance (HOMA–IR) and adiponectin/leptin ratio in pregnant women (n = 74); r = −0.42, 95% confidence interval −0.6, −0.22; P < 0.01; Pearson’s correlation coefficient.
Discussion
Several studies have investigated the role of the adiponectin/leptin ratio in states with increased insulin resistance.7–12 The present study investigated the significance of the adiponectin/leptin ratio in pregnancy. A significant inverse correlation was found between the adiponectin/leptin ratio and insulin resistance, using HOMA–IR as a reference. Additionally, the serum leptin concentration correlated with HOMA–IR, whereas no correlation was found between the adiponectin concentration and HOMA–IR.
It has been shown that, compared with healthy subjects, adiponectin concentrations are lower in insulin-resistant states such as obesity and type 2 diabetes mellitus. 3 Adiponectin concentrations are also lower in women with gestational diabetes mellitus, compared with those having a normal pregnancy.14,15 In contrast, higher leptin concentrations have been observed in women with gestational diabetes mellitus compared with those who have normal glucose tolerance.15,16 Other studies, however, have found no difference in leptin concentrations between women with gestational diabetes mellitus and those who are having a normal pregnancy, 14 and no correlation between concentrations of adipocytokines (including adiponectin and leptin) and gestational diabetes mellitus. 17
A study performed in obese subjects showed that an increased leptin/adiponectin ratio and increased leptin concentrations, as well as decreased adiponectin concentrations, were associated with insulin resistance in this population. 7 The pregnant women in the present study were not classified as obese (median BMI before pregnancy being 22.68 kg/m2 and median BMI during pregnancy being 26.57 kg/m2) which could explain why no correlations between HOMA–IR and adiponectin concentrations were observed.
The present study also showed an inverse correlation between the adiponectin/leptin ratio and BMI before pregnancy. This is in accordance with a report indicating that the leptin/adiponectin ratio correlated with BMI and HOMA–IR in obese patients. 8 In a study involving a paediatric population, the leptin/adiponectin ratio was eight-fold greater in obese compared with nonobese children, and showed a stronger correlation with BMI than adiponectin alone. 18 Moreover, the adiponectin/leptin ratio has been shown to correlate with percentage body fat, lipid profile and HOMA–IR in a study on metabolic syndrome, 12 and has been described as a sensitive and specific biomarker for metabolic syndrome, 19 as well as an indicator of atherosclerosis. 20
The adiponectin/leptin ratio has been described as a more sensitive and reliable marker of insulin resistance than the HOMA–IR, in patients with type 2 diabetes, as fasting plasma glucose concentrations rise. 10 It has also been suggested that, for type 2 diabetic patients, the adiponectin/leptin ratio may add information beyond that obtained by analysing separate adipocytokines. 21 The present study revealed that the correlation between the leptin concentration and HOMA–IR was similar to that between the adiponectin/leptin ratio and HOMA–IR. Nevertheless, since pregnant women represent a diverse population, the adiponectin/leptin ratio might be a more reliable marker of insulin resistance than the leptin concentration alone. Studies involving larger populations are required to answer this question.
The present study was limited by the fact that the adiponectin/leptin ratio was only compared with insulin resistance as measured by HOMA-IR, not with insulin resistance measured using the euglycaemic–hyperinsulinaemic clamp technique (an invasive procedure not generally used in pregnant women). In patients with type 2 diabetes, the adiponectin/leptin ratio correlated better with the clamp technique measurement of insulin resistance than did HOMA–IR and other surrogate measures of insulin resistance. 9 A larger study in nondiabetic individuals, performed to investigate correlations between the leptin/adiponectin ratio and measures of insulin resistance (including the euglycaemic–hyperinsulinaemic clamp method), revealed the leptin/adiponectin ratio to be a useful measure of insulin resistance. 22
One report suggested that adiponectin and leptin concentrations in pregnancy are influenced by various factors, including placental hormone levels, 23 which were not investigated in the present study. Overall, the results of the present study can be applied to a broader understanding of the significance of adiponectin/leptin ratio in insulin-resistant states.
In conclusion, both the adiponectin/leptin ratio and the leptin concentration correlate with the HOMA–IR, in pregnant women. Further studies in larger populations are required, to determine whether the adiponectin/leptin ratio could represent a potential biomarker of insulin resistance in pregnancy, and provide information beyond the HOMA–IR.
Footnotes
Declaration of Conflicting Interest
The authors declare that there are no conflicts of interest.
Funding
This study was supported by the Slovenian Ministry of Higher Education, Science and Technology, Ljubljana, Slovenia.