
Abstract
The purpose of this study was to analyse the influence of simultaneous pancreas–kidney or kidney transplantation on endothelial function and systemic inflammation in type 1 diabetic patients with end-stage renal disease. In 39 simultaneous pancreas–kidney, 39 type 1 diabetic kidney and 52 non-diabetic kidney recipients, flow-mediated dilatation was measured. Additionally, blood glycated haemoglobin, serum creatinine and lipids, plasma nitrites
Keywords
Introduction
Patients with end-stage renal disease (ESRD) caused by type 1 diabetes (T1D) have poor prognosis on dialysis therapy. 1 Transplantation of kidneys procured from living or deceased donors reduces unacceptable mortality of these patients,2–4 and simultaneous pancreas–kidney transplantation (SPK) or transplantation of pancreas after living donor kidney transplantation (KTx) further improves long-term recipients and kidney grafts survivals.5–7 Pancreas and kidney recipients present reduced cardiovascular mortality and morbidity, which are a consequence of restored normal glucose metabolism, and better control of serum lipids and blood pressure (BP), compared to patients after KTx.7–9 However, the mechanism of beneficial influence of pancreas transplantation on vascular system exposed to long-term diabetic milieu remains unclear. The explanation of the observed improvement is additionally hindered by arterial injury caused by chronic renal insufficiency and dialysis therapy and by differences between patients treated with SPK or KTx in factors related to donor, recipient and transplantation procedures.2–4,10,11
According to numerous studies, it is endothelial dysfunction (ED) that plays the key role in the pathogenesis of atherosclerosis
12
and diabetic vascular injury.13–15 Since in T1D patients elevated plasma concentrations of inflammatory markers and soluble adhesion molecules are associated with cardiovascular disease and nephropathy,16,17 normalisation of these ED markers in SPK recipients is expected. However, the data concerning function of endothelium after pancreas transplantation are limited. In an experimental model, pancreatic transplantation restored the defective endothelium-dependent relaxation to acetylcholine without altering the relaxation to nitroglycerin.
18
T1D patients presented preserved
The aim of this cross-sectional study was to perform tests of endothelium function, as well as to measure several confirmed and novel biochemical markers of ED and systemic inflammation in T1D patients with ESRD treated with either SPK or KTx during medium-term follow-up period after transplantation.
Methods
The present cross-sectional study was performed in patients treated in two Polish transplant centres in Katowice and Wrocław (2014–2015). The study protocol was approved by Bioethics Committee of the Medical University of Silesia in Katowice (KNW/0022/KB1/151/12), and each participant gave the informed consent.
Study groups
Two equinumerous groups of T1D patients (N = 39) after SPK or KTx, with a minimum post-transplant follow-up period of 12 months, were enrolled into the study. In all patients, T1D requiring insulin therapy was diagnosed in childhood or adolescence, and ESRD developed as a consequence of long-lasting diabetes. The control group consisted of 52 kidney transplanted patients without diabetes diagnosed pre- or post-transplant.
The matching procedure was designed to include recipient’s gender, age at the time of transplantation, duration of pre-transplant diabetes and dialysis vintage. The limited number of eligible T1D kidney recipients in both centres (though comparable or larger than analysed in few previously performed studies devoted to this issue19–21) precluded full adjustment in all potentially significant selection criteria, particularly duration of follow-up period after transplantation.
The exclusion criteria included pre-emptive, living donor or second/third KTx; significantly impaired kidney graft function at the time of the study with estimated glomerular filtration rate (eGFR) ≤30 mL/min/1.73 m2 (calculated according to Modification of Diet in Renal Disease Study (MDRD) formula); bacterial or viral infection within 1 month preceding the study; diagnosis of cancer or liver cirrhosis; non-compliance; nitrates medication and additionally any antidiabetic medication in SPK recipients.
In all patients, kidney was transplanted on a standard basis, and in SPK recipients, pancreatic graft was placed intraperitoneally with systemic drainage of venous blood and enteric drainage of pancreatic juice.
Clinical data were obtained from a transplant centre–operated databases and from original medical records. and included recipient gender, age at the time of transplantation and at the time study, body mass index (BMI), duration of diabetes, dialysis vintage and follow-up period, smoking status, co-medication with immunosuppressive agents, glucocorticoids and statins.
BP was measured three times in the sitting position in the arm without arteriovenous fistula at the beginning of the study. Patients with BP values above 140/90 mmHg or those who received antihypertensive medication were diagnosed as hypertensive.
FMD measurements
FMD was measured after 12 h of fasting and after 10 min of lying in a quiet room with temperature of 20°C–25°C, using Aloka Prosound Alpha 6 ultrasound device (Hitachi Aloka Medical, Ltd., Mitaka, Japan) in both institutions. Patients were not allowed to smoke at least 6 h prior to the examination. Manual sphygmomanometer cuff was placed high on the arm without arteriovenous fistula, and 7–12 MHz linear transducer was positioned 4–5 cm above the cubital fossa in order to visualise a brachial artery and to measure its diameter (lumen). After initial BP measurement, the cuff was inflated approximately 50 mmHg above a current systolic pressure for 5 min (a minimum of 200 mmHg was applied). The widest dilatation of brachial artery was measured 60 s after cuff deflation (according to R wave). FMD was calculated as follows: FMD% = (A – B)/B × 100%, where A is diameter of artery after dilatation and B before examination.
Laboratory measurements
Concentrations of blood glycated haemoglobin (HbA1C) and serum creatinine and lipids were routinely measured during standard outpatient visit. Additionally, to obtain plasma from each patient, blood samples were withdrawn in a closed system into tubes containing citrate and ethylenediaminetetraacetic acid (EDTA). The tubes were allowed to stand for 2 h at room temperature, then centrifuged (15 min, 3000 r/min) and finally preserved at −70°C.
Plasma
The plasma concentrations of soluble vascular cell adhesion molecule-1 (sVCAM-1), soluble intercellular adhesion molecule-1 (sICAM-1) and soluble E-selectin (sE-selectin) were measured by enzyme-linked immunosorbent assay (ELISA; Diaclone SAS, Besancon, France), with sensitivity of 10, 30 and 5 ng/mL; intra-assay variation <2.8%, <4.5% and <4.1% and inter-assay variation <8.2%, <5.9% and <6.4%, respectively. Asymmetric dimethylarginine (ADMA) and high-sensitivity C-reactive protein (hsCRP) were assessed with ELISA (Immundiagnostik AG, Bensheim, Germany), with sensitivity of 0.05 µmol/L and 0.09 mg/L, intra-assay variation <7.8% and <6% and inter-assay variation <8.8% and <11.6%, respectively.The plasma concentrations of tumour necrosis factor-α (TNF-α), interleukin 6 and interleukin 1β were measured by ELISA (R&D Systems, Inc., Minneapolis, MN, USA), with sensitivity of 0.1, 0.04 and 1 pg/mL; intra-assay variation <8.7%, <7.4% and <8.5% and inter-assay variation <10.4%, <9.6% and <8.5%, respectively.
Statistical analysis
Statistical analysis was performed using STATISTICA 12.5 PL (StatSoft, Cracow, Poland), StataSE 12.0 (StataCorp LP, College Station, TX, USA) and R software. Statistical significance was set at a p value below 0.05. All tests were two-tailed. Imputations were not done for a few missing clinical data. Nominal and ordinal data were expressed as percentages, while interval data were expressed as mean value ± standard deviation (SD) in case of normal distribution or as median (lower quartile - upper quartile) in case of data with skewed or non-normal distribution. Distribution of variables was evaluated by the Shapiro–Wilk test and homogeneity of variances was assessed by the Levene test.
For comparison of data between all three analysed groups, the one-way analysis of variance (ANOVA) was used with Tukey’s honest significant difference (HSD) post hoc test. In case of skewed distribution, normalisation with the logarithmic function was done. Categorical variables were compared using either the χ2 tests or the χ2 tests with Yates correction.
In order to assess the relationship between variables, a linear regression was used with Pearson correlation coefficient. Multivariate models included variables selected on the basis of univariate regression analyses. The Cook–Weisberg test and Cameron and Trivedi’s decomposition test were used to test the residuals for heteroscedasticity as well as the violation of skewness and kurtosis assumptions in linear regression.
Results
Study group characteristics
Both recipient’s age and duration of diabetes at the time of transplantation were similar in SPK and KTx groups (Table 1). However, as a consequence of longer post-transplant follow-up period in KTx group, patients in this group were older at the time of the study than patients after SPK. Of note, there were no differences in BMI and dialysis vintage before transplantation between SPK and KTx groups. The frequency of hypertension was twice lower in patients after SPK than after KTx; however, current systolic and diastolic BPs were similar. There were also significant differences in immunosuppressive regimen and statin usage between SPK and KTx groups. HbA1C concentration was normal in SPK group and elevated in T1D patients after KTx. Finally, the kidney graft function was better and serum triglycerides level was lower in SPK group than in KTx group (Table 2). Results obtained in control group of non-diabetic kidney transplant recipients are presented in Tables 1 and 2.
Clinical parameters of patients in study groups (numbers and frequencies or mean ± standard deviation (SD)).
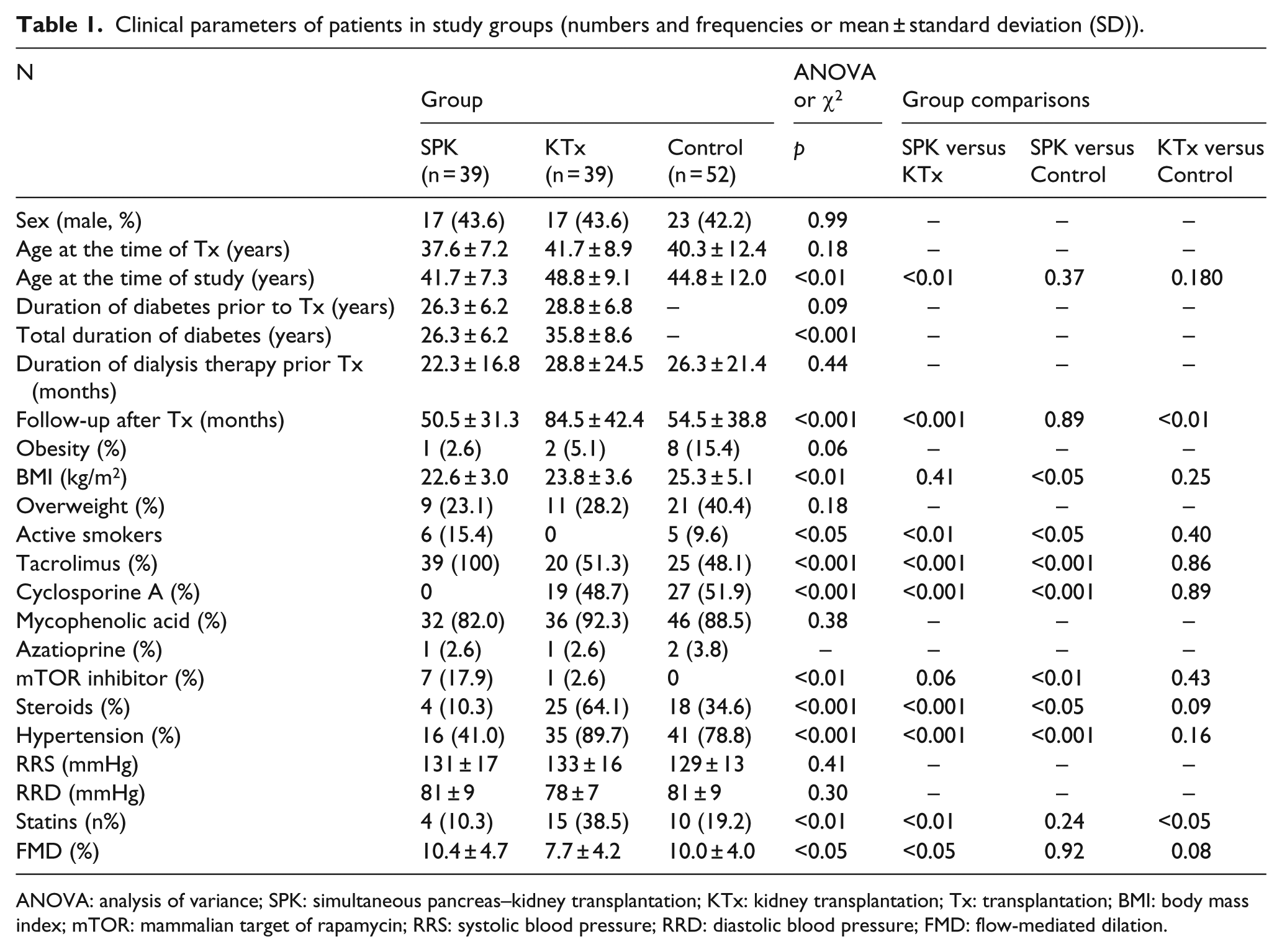
ANOVA: analysis of variance; SPK: simultaneous pancreas–kidney transplantation; KTx: kidney transplantation; Tx: transplantation; BMI: body mass index; mTOR: mammalian target of rapamycin; RRS: systolic blood pressure; RRD: diastolic blood pressure; FMD: flow-mediated dilation.
Biochemical parameters of patients in study groups (mean ± standard deviation (SD) or median (lower quartile - upper quartile)).
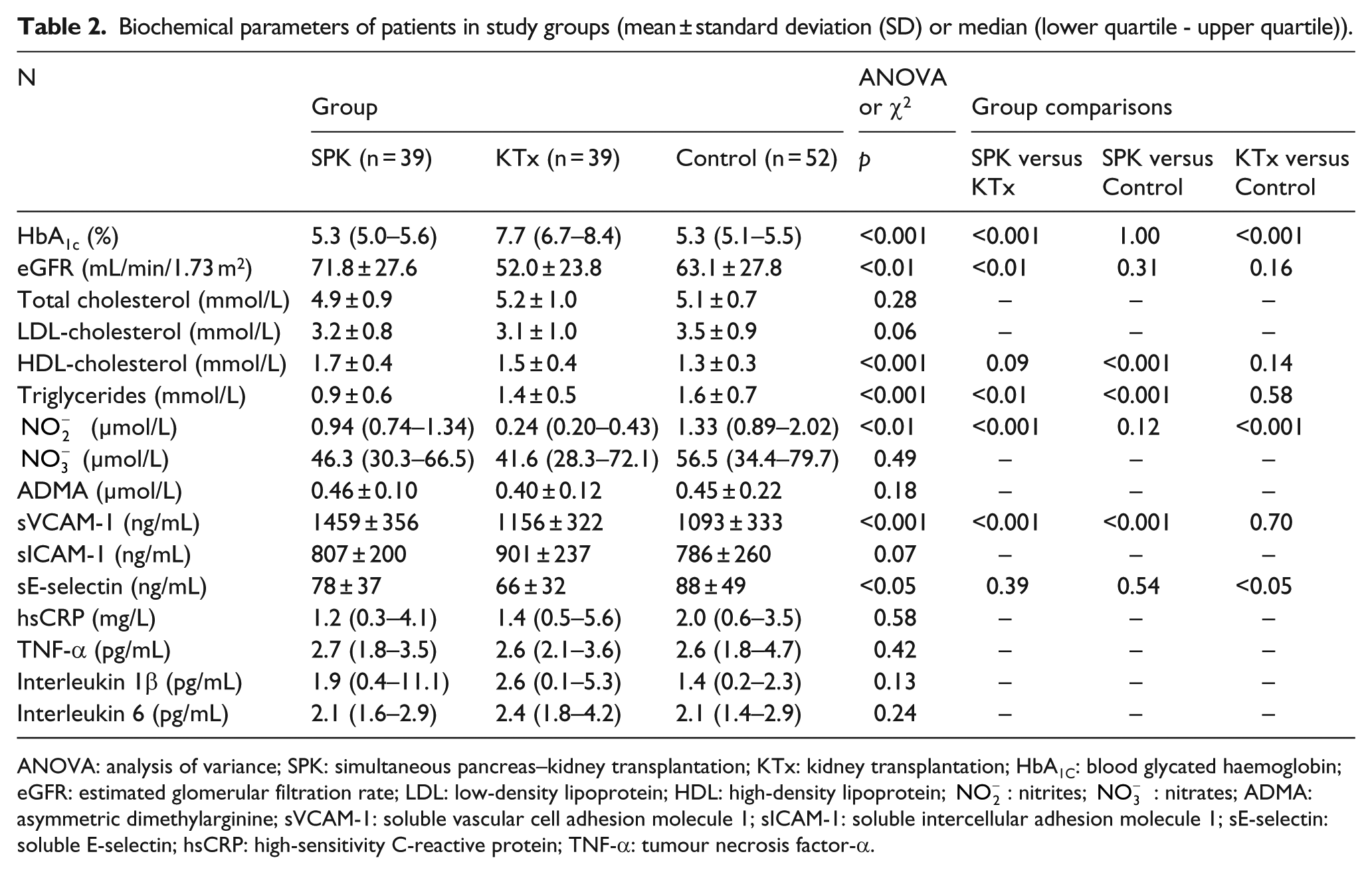
ANOVA: analysis of variance; SPK: simultaneous pancreas–kidney transplantation; KTx: kidney transplantation; HbA1C: blood glycated haemoglobin; eGFR: estimated glomerular filtration rate; LDL: low-density lipoprotein; HDL: high-density lipoprotein;
Endothelial function
FMD values and
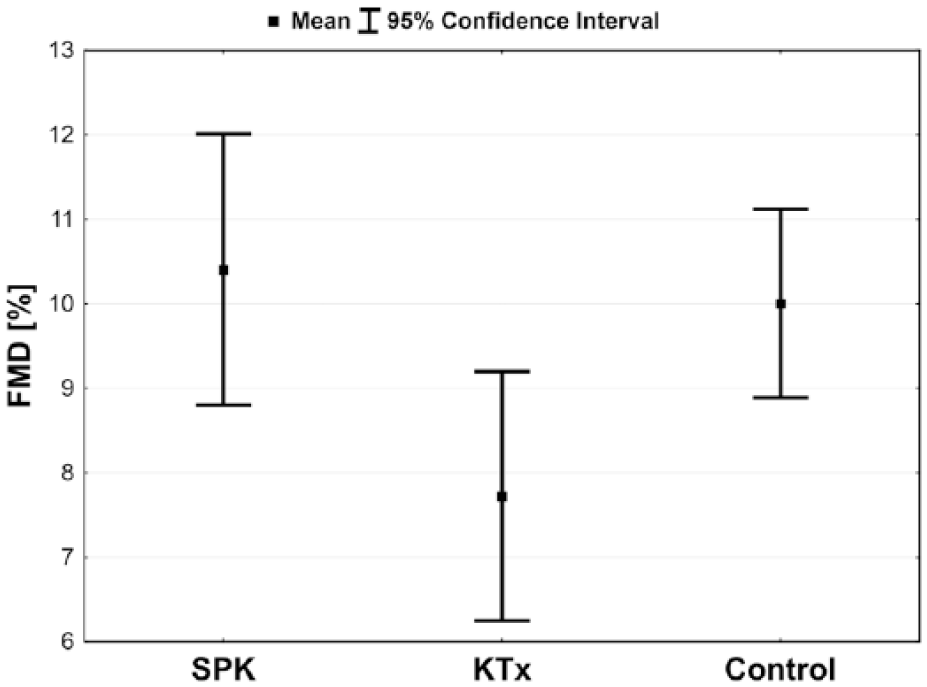
Mean values with confidence intervals of the flow-mediated dilatation (FMD) according to study groups: simultaneous pancreas–kidney transplantation (SPK), kidney transplantation (KTx) and control.
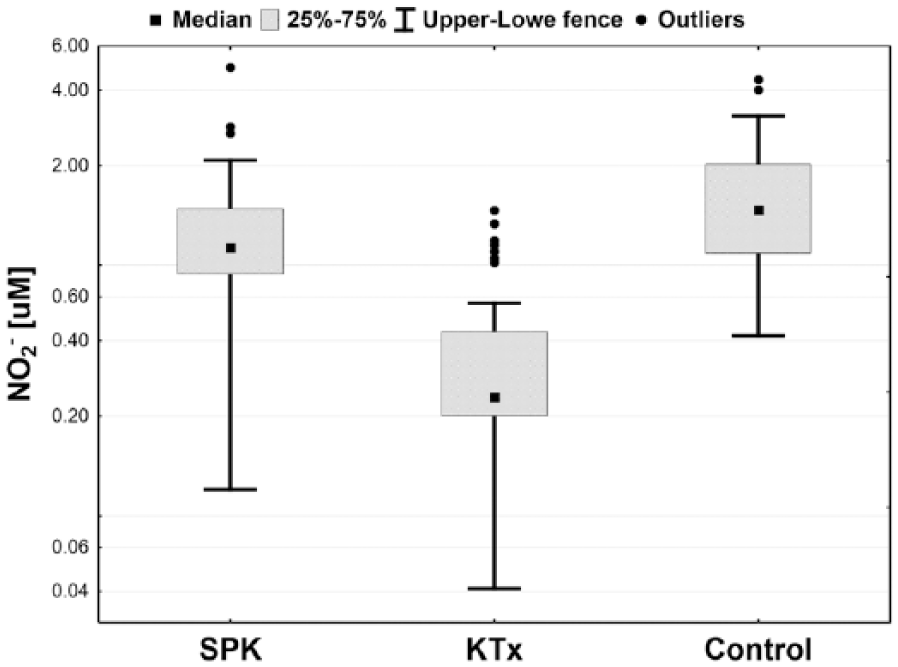
Box-plot of plasma nitrites concentration
Subanalysis of T1D patients
In the combined group of T1D patients after SPK or KTx, univariate analysis revealed that FMD variability was explained by age at the time of study and
Results of univariate linear regression analyses – factors influencing flow-mediated dilatation (FMD) and plasma nitrites concentration
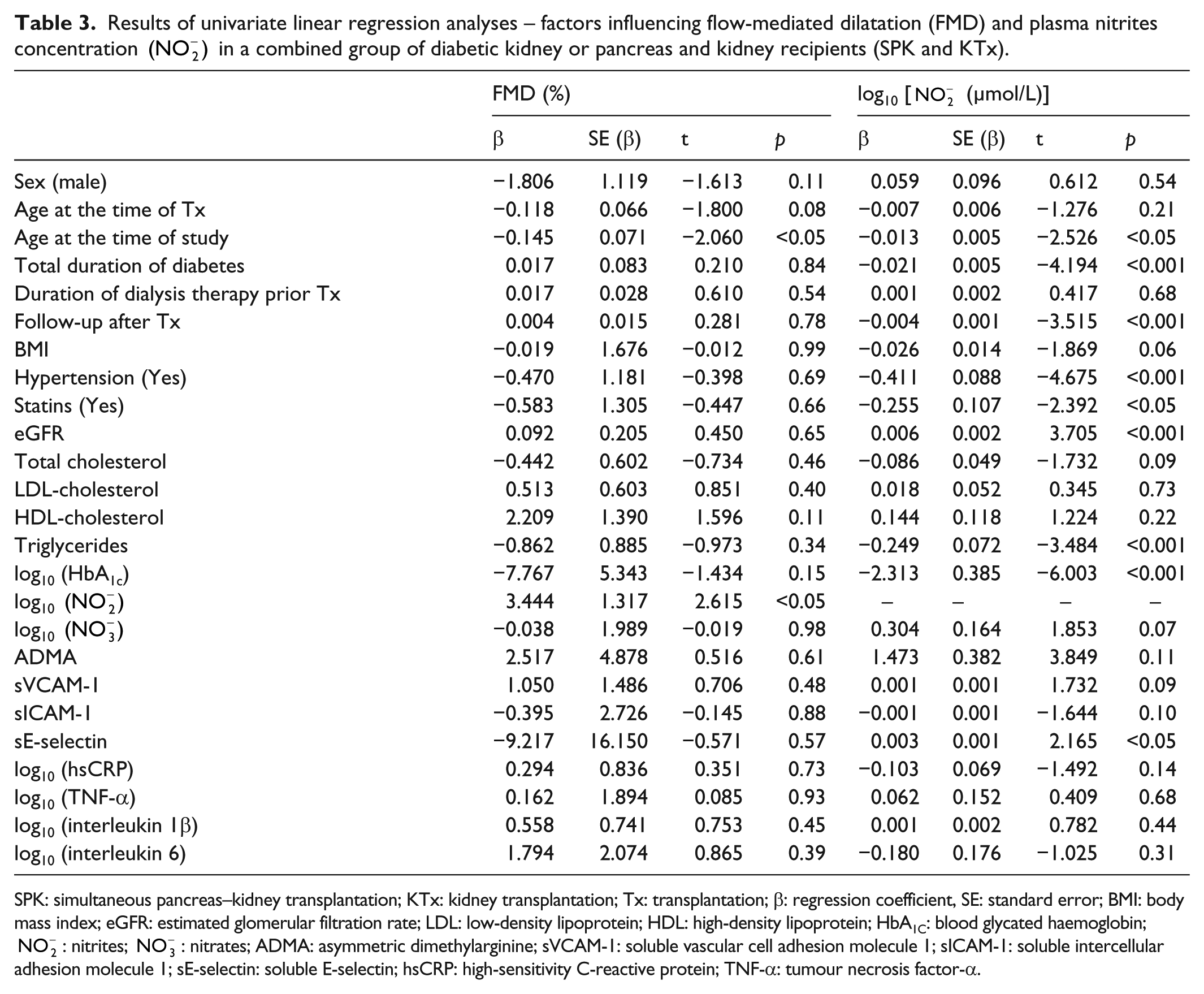
SPK: simultaneous pancreas–kidney transplantation; KTx: kidney transplantation; Tx: transplantation; β: regression coefficient, SE: standard error; BMI: body mass index; eGFR: estimated glomerular filtration rate; LDL: low-density lipoprotein; HDL: high-density lipoprotein; HbA1C: blood glycated haemoglobin;
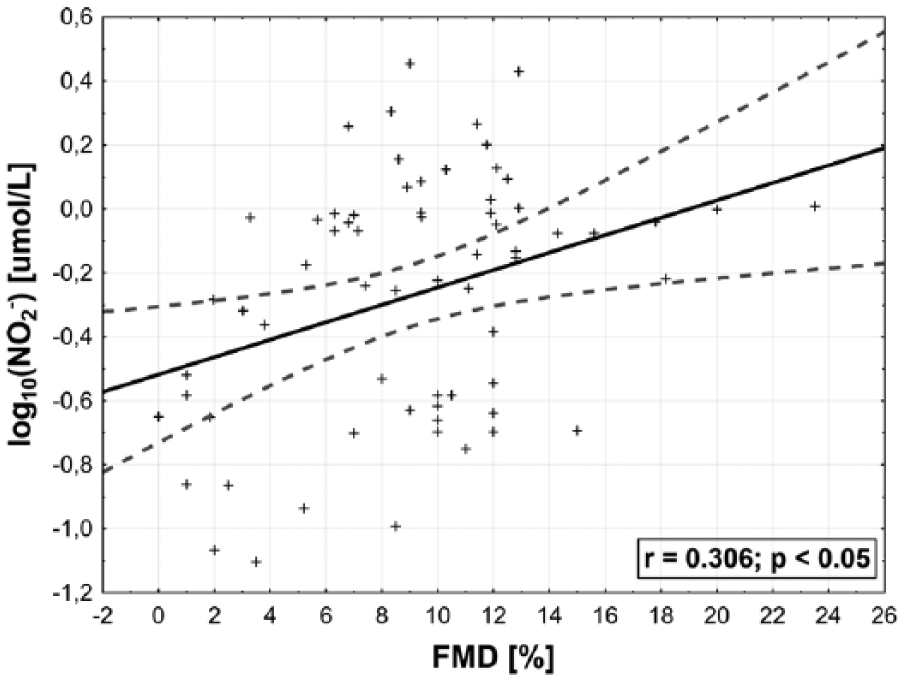
Linear regression between plasma nitrites concentration
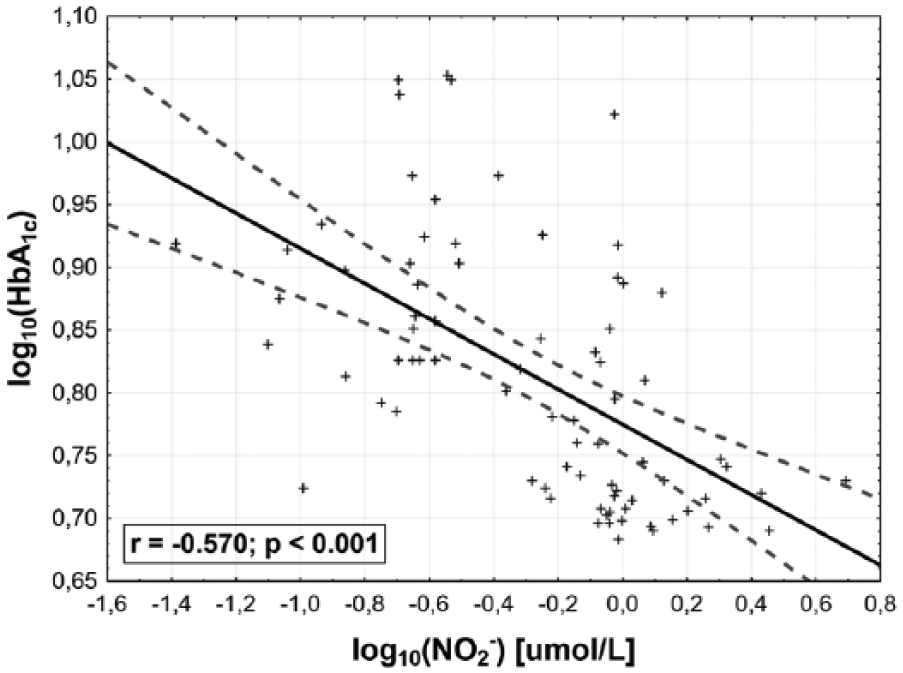
Linear regression between blood glycated haemoglobin (HbA1C) and plasma nitrites concentration
The variabilities of sVCAM-1 and sE-selectin were not explained by duration of diabetes, blood HbA1C or serum inflammatory markers levels or eGFR.
Discussion
In this study, we have shown for the first time that increased plasma
A number of studies confirmed a key role of ED in the pathogenesis of arterial wall injury in T1D patients.24–27 Decreased concentration of
Improved FMD in T1D patients after SPK compared to KTx was shown for the first time by Fiorina et al.
20
Both their and our findings are in line with the results of De Cobelli et al.
19
cross-sectional study, which revealed increased renal blood flow following the administration of
Since FMD inversely correlates with blood HbA1C in T1D patients,
26
and progression of arterial injury and cardiovascular risk in T1D patients is related to blood glucose control,30,31 we can assume that relationship between HbA1C and
However, in analysis of our study results, several potentially relevant factors that might influence observed differences in endothelial function between analysed groups must be considered.
These parameters undoubtedly belongs age.
32
Actually, this strong cardiovascular risk factor, higher in T1D kidney recipients compared to patients after SPK, correlated with both FMD and
Another confounder that should be addressed was significantly lower frequency of hypertension in SPK group. The improvement of BP control after SPK was shown by Luan et al.
9
We cannot exclude that improvement of endothelial function in addition to better kidney graft function and more frequent steroids withdrawal in SPK group resulted in better BP control, although this association can also be explained inversely. Impaired endothelium-dependent vasodilation was previously shown in patients with essential hypertension, and these observations were explained by the defect in NO synthesis.33,34 The lack of independent effect of hypertension on neither
The improvement of endothelial function in SPK recipients may be also related to lower serum triglycerides levels and less frequent necessity of statins administration observed by us and revealed in previous reports. 9 Since several studies confirmed positive influence of improved lipids profile achieved with statins administration on FMD, 35 we cannot exclude that better matching of study groups including statins use would reveal even greater differences in endothelial function. However, the lack of influence of triglycerides concentration and statin usage on endothelial function markers in multivariate analysis suggest that improvement of lipid disorders after SPK is less important than the restoration of normal glucose metabolism.
The only independent factor affecting plasma
Since decrease in FMD was reported to be accompanied by increased serum inflammatory markers and adhesion molecule concentrations,
39
and values of these biochemical parameters were elevated in T1D patients with both microalbuminuria and overt nephropathy,
17
we expected significant differences regarding mentioned factors between analysed groups. Despite analysis of wide panel of serum inflammatory markers and adhesion molecules, we failed to prove reduced inflammatory status and decreased values of adhesion molecules in patients after SPK compared to T1D kidney recipients. Although we noticed higher levels of sVCAM-1 in SPK patients, the potential influence of this factor on FMD or
The limitations of this study include its cross-sectional design, which precludes the possibility of prospective observation of endothelial function evolution in diabetic SPK and KTx recipients. Due to lack of data concerning patient’s vascular history, we were also not able to consider the interactions between ED and efficacy of diabetes, hypertension and lipid disorder therapy before transplantation. Of note, prospective studies devoted to this issue are not available so far, but their execution will be difficult due to differences in numerous clinical parameters between patients referred to SPK and KTx. 42
Limited size of the study caused that patients matching did not include all important parameters, for example, calcineurin inhibitors and steroids usage in both diabetic subgroups. However, the use of different calcineurin inhibitors in SPK recipients had no effect on glucose metabolism in the late post-transplant period, 43 and to the best of our knowledge, there is no data concerning the influence of calcineurin inhibitors or steroids administration on endothelial function.
Concluding, normal glucose metabolism achieved by simultaneously transplanted pancreas is associated with better endothelial function as evidenced by higher
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This research project was funded by National Science Centre, Poland (OPUS 5; Grant No. 2013/09/B/NZ5/00258).