
Abstract
This publication is a commentary on the Letter to the Editor by Juliette Raffort and Fabien Lareyre. This article clarifies a number of concerns about the method of calculating the index of prevalence of ruptured abdominal aortic aneurysms (AAA). The method of qualifying patients for the study and the method of calculating the index of prevalence of ruptured AAA in cohorts of diabetic and non-diabetic patients was presented. Most researchers calculate the Index of Prevalence per 100,000 of the general population. This gives the misleading result that diabetes reduces the risk of AAA rupture.We used a method which calculated prevalence per 100,000 with diabetes mellitus and per 100,000 without diabetes mellitus. This method confirms that diabetes mellitus increases the risk of ruptured AAA.
Keywords
Dear Sir, We are pleased to be given the opportunity to answer questions raised by Raffort and Lareyre 1 relating to our paper published in this journal ‘Diabetes mellitus increases the risk of ruptured abdominal aortic aneurysms’. 2
The diagnosis of diabetes mellitus was made using the criteria of the Polish Society of Diabetes which are identical to those employed by other organisations, for example, the European Society of Endocrinology, and verified by payers at a regional and national level. Data are collected in the registry of the National Health Fund (NHF) according to the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10).
The NHF database in Poland for the period 1 January and 31 December 2012 includes reports regarding services for the main diagnosis of abdominal aortic aneurysms (AAA) according to the following ICD-10 codes: 171.3 – aneurysm of the abdominal aorta, raptured and 171.4 – aneurysm of the abdominal aorta without rapture. Reports for services associated with diabetes with the main diagnosis of ‘diabetes mellitus’ were found in the NHF database for the year 2012 with ICD-10 codes: E10.X – insulin-dependent diabetes mellitus; E11.X – insulin non-dependent diabetes mellitus; E12.X – malnutrition-related diabetes mellitus; E13.X – other unspecified forms of diabetes mellitus; E14.X – unspecified diabetes mellitus or patient taking medications from group A10.X (insulins); and A10B.X – oral antidiabetic agents and specialised and appropriate diagnostic tests.
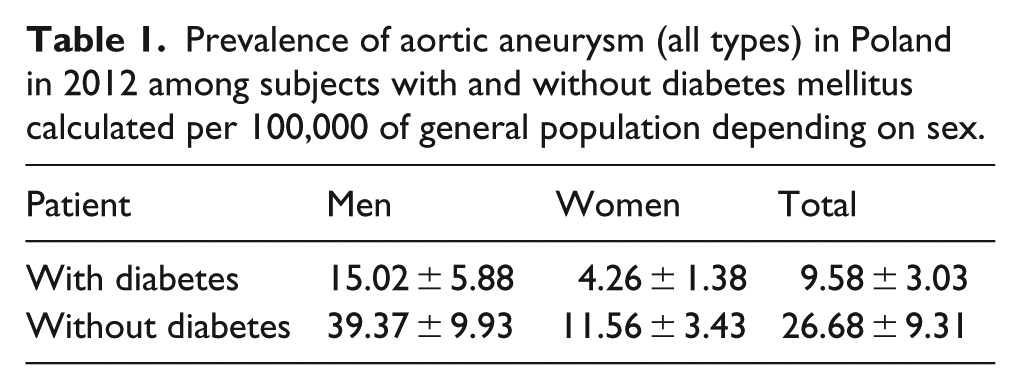
The cohorts involved in the study were similar to those described in other publications. The novel approach in our article was the method used to calculate the Index of Prevalence per 100,000 of the general population. This was previously described by Lilienfeld et al., 3 Lopez-de-Andres et al. 4 and De Rango et al.; 5 however, in papers by Wierzba et al. 2 and Czeleko et al., 6 we used a different method which calculated prevalence per 100,000 with diabetes mellitus and per 100,000 without diabetes mellitus, which seems to better represent the clinical and epidemiological picture. This method of calculation for all types of aortic aneurysms in the population with and without diabetes mellitus obtained values close to those presented in papers by Takagi and Umemoto 7 and De Rango et al. 5 and others (Table 1).
Prevalence of aortic aneurysm (all types) in Poland in 2012 among subjects with and without diabetes mellitus calculated per 100,000 of general population depending on sex.
Using this method, our results indicated a higher prevalence of ruptured aortic aneurysm in diabetes mellitus subjects. Data limitations did not allow an evaluation of the type or duration of diabetes or the relationship of aneurysm rupture to the presence of hypertension or obesity and lipid values or control of diabetes.
We concur with Raffort et al. regarding the underdiagnosis of diabetes. Simulated calculations assuming a 30% higher number of diabetes subjects do not change the final conclusion that there is a higher prevalence of AAA rapture in patients with diabetes.
We also agree with the need for further prospective studies of this issue.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.