
Abstract
Purpose:
To summarize the association of diabetes with abdominal aortic aneurysm rupture, we reviewed currently available studies with a systematic literature search and meta-analytic evaluation.
Methods:
To identify all studies reporting the association of diabetes with abdominal aortic aneurysm rupture, MEDLINE and EMBASE were searched through July 2015. For each study, data regarding diabetes prevalence in both the ruptured and non-ruptured groups were used to generate an unadjusted odds ratio for abdominal aortic aneurysm rupture and 95% confidence intervals. Alternatively, an unadjusted or adjusted odds ratio, or hazard ratio for abdominal aortic aneurysm rupture with 95% confidence interval was directly abstracted (as available) from each individual study.
Results:
Our search identified 11 eligible studies. A primary meta-analysis of nine studies reporting data on ruptured (not including non-ruptured symptomatic) abdominal aortic aneurysm demonstrated that diabetes was associated with significantly lower prevalence/incidence of abdominal aortic aneurysm rupture (odds ratio/hazard ratio, 0.71; 95% confidence interval, 0.56 to 0.89; p = 0.003). A secondary meta-analysis of all 11 studies (adding two studies in which non-ruptured symptomatic abdominal aortic aneurysm was included in the rupture group) also demonstrated that diabetes was associated with significantly lower prevalence/incidence of abdominal aortic aneurysm rupture (odds ratio/hazard ratio, 0.77; 95% confidence interval, 0.63 to 0.95; p = 0.01).
Conclusion:
Diabetes is negatively associated with abdominal aortic aneurysm rupture.
Introduction
Coronary artery disease (CAD) and peripheral artery disease (PAD), both representative atherosclerotic diseases, are positively associated with the presence of abdominal aortic aneurysm (AAA).1,2 Despite the positive associations of CAD and PAD with AAA presence, diabetes (major risk factor of CAD and PAD) is negatively associated with not only presence 3 but also growth 4 of AAA. The negative associations of diabetes with AAA presence and growth support the hypothesis that diabetes may be also negatively associated with AAA rupture. The RESCAN individual patient data meta-analysis 5 of only two studies6,7 including a total of 3153 patients with small AAA, however, revealed no association between diabetes and rupture. Whereas, a recent large (including 188 patients with ruptured and 1482 patients with non-ruptured AAA) retrospective study by Theivacumar et al. 8 suggests that diabetes patients with AAA are significantly less likely to present with rupture or to die from aneurysm rupture when compared to non-diabetes patients with AAA. It is still debated whether diabetes is negatively associated with AAA rupture. To summarize the association of diabetes with AAA rupture, we reviewed currently available studies with a systematic literature search and meta-analytic evaluation in this article.
Methods
All studies reporting the association of diabetes with AAA rupture were identified using a two-level search strategy. First, databases including MEDLINE and EMBASE were searched through July 2015 using Web-based search engines (PubMed and OVID). Second, relevant studies were identified through a manual search of secondary sources including references of initially identified articles and a search of reviews and commentaries. All references were downloaded for consolidation, elimination of duplicates and further analysis. Search terms included ‘rupture’ or ‘ruptured’, ‘abdominal aortic aneurysm/aneurysms’ and ‘diabetes’ or ‘diabetic/diabetics’.
Studies considered for inclusion met the following criteria: the design was a case–control or prospective/retrospective cohort study; the study population was (1) patients with ruptured AAA and those with non-ruptured AAA or (2) patients with diabetes and those without diabetes; and main outcomes included (1) diabetes prevalence or (2) AAA-rupture incidence. Two authors (H.T. and T.U.) reviewed the eligible studies and determined whether the studies met the selection criteria. For each study, data regarding diabetes prevalence in both the ruptured and non-ruptured groups were used to generate an unadjusted odds ratio (OR) for AAA rupture and 95% confidence intervals (CIs). Alternatively, an unadjusted or adjusted OR or hazard ratio (HR) for AAA rupture with 95% CI was directly abstracted (as available) from each individual study. Data were extracted in duplicate by two investigators (H.T. and T.U.), and disagreements were resolved by consensus.
Study-specific estimates (preferentially adjusted estimates) were combined using inverse variance-weighted averages of logarithmic ORs/HRs in both fixed-effect and random-effects models. Between-study heterogeneity was analysed by means of standard χ2 tests. Where no statistically significant heterogeneity was identified, the fixed-effect estimate was used preferentially as the summary measure. Sensitivity analyses were performed to assess the contribution of each study to the pooled estimate by excluding individual studies one at a time and recalculating the pooled OR/HR estimates for the remaining studies. Publication bias was assessed graphically using a funnel plot and mathematically using an adjusted rank-correlation test 9 and a linear regression test. 10 All analyses were conducted using Review Manager version 5.3 (available from http://tech.cochrane.org/revman) and Comprehensive Meta-Analysis version 3 (Biostat, Englewood, NJ).
Results
Of 100 potentially relevant articles screened initially, nine eligible studies8,11–18 were identified. Furthermore, two relevant studies6,7 were added through a manual search. In total, our meta-analysis included 11 studies.6–8,11–18 Study design (Table 1), patient characteristics (Table 1; online Appendices 1 and 2), diabetes prevalence, rupture incidence and relative risk of rupture are summarized in Table 2. In a case–control study by Buijs et al., 11 non-ruptured symptomatic AAA and ruptured AAA were combined and labelled as non-elective AAA. In the rupture group of another case–control study by Fillinger et al., 13 emergency AAA repair was performed because of rupture or acute severe pain. As a primary meta-analysis, thus, we combined the remaining nine studies6–8,12,14–18 reporting data on ruptured (not including non-ruptured symptomatic) AAA. Additionally, all of the 11 studies were combined as a secondary meta-analysis.
Study design and patient characteristics.
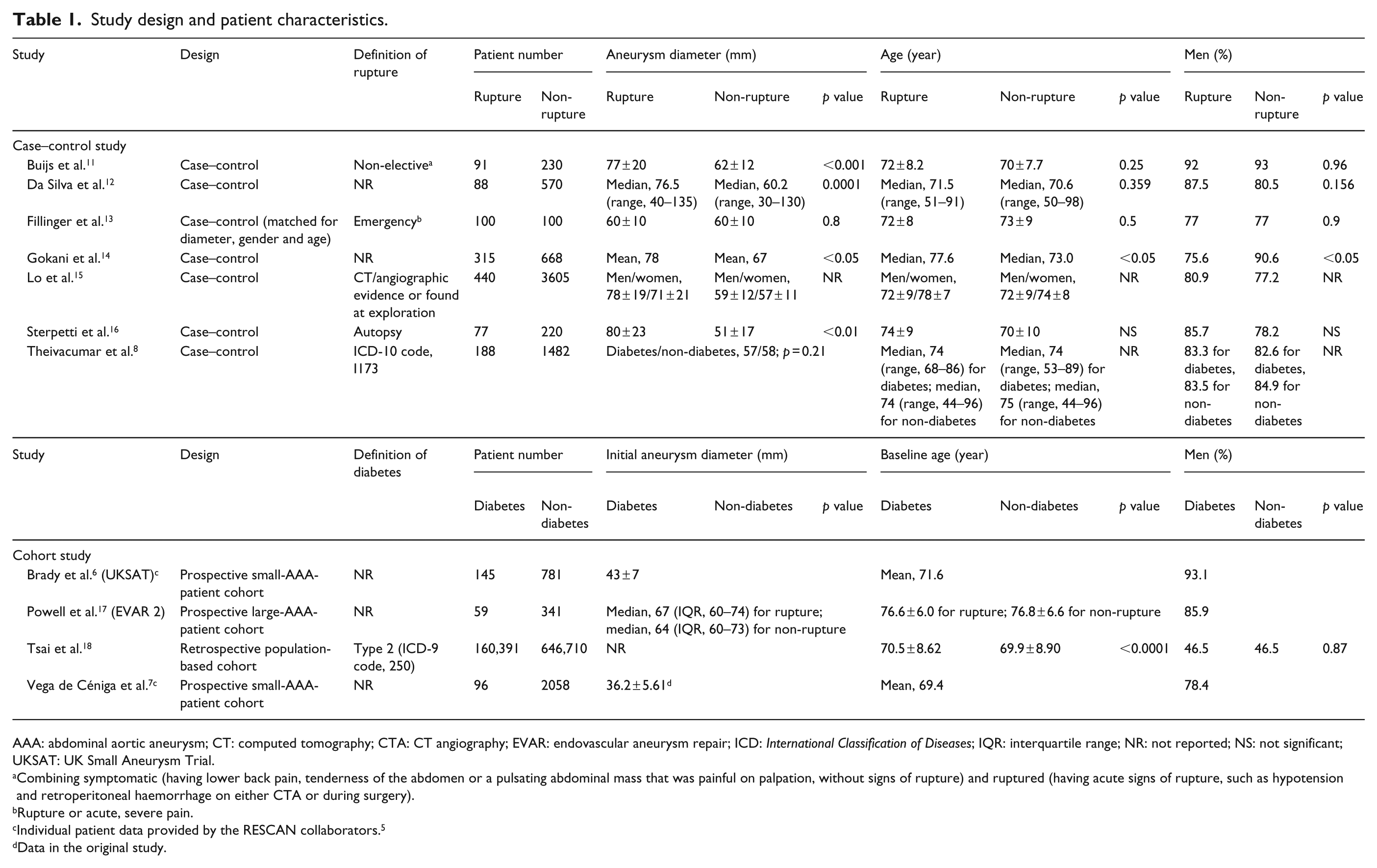
AAA: abdominal aortic aneurysm; CT: computed tomography; CTA: CT angiography; EVAR: endovascular aneurysm repair; ICD: International Classification of Diseases; IQR: interquartile range; NR: not reported; NS: not significant; UKSAT: UK Small Aneurysm Trial.
Combining symptomatic (having lower back pain, tenderness of the abdomen or a pulsating abdominal mass that was painful on palpation, without signs of rupture) and ruptured (having acute signs of rupture, such as hypotension and retroperitoneal haemorrhage on either CTA or during surgery).
Rupture or acute, severe pain.
Individual patient data provided by the RESCAN collaborators. 5
Data in the original study.
Diabetes prevalence, rupture incidence and relative risk of rupture.
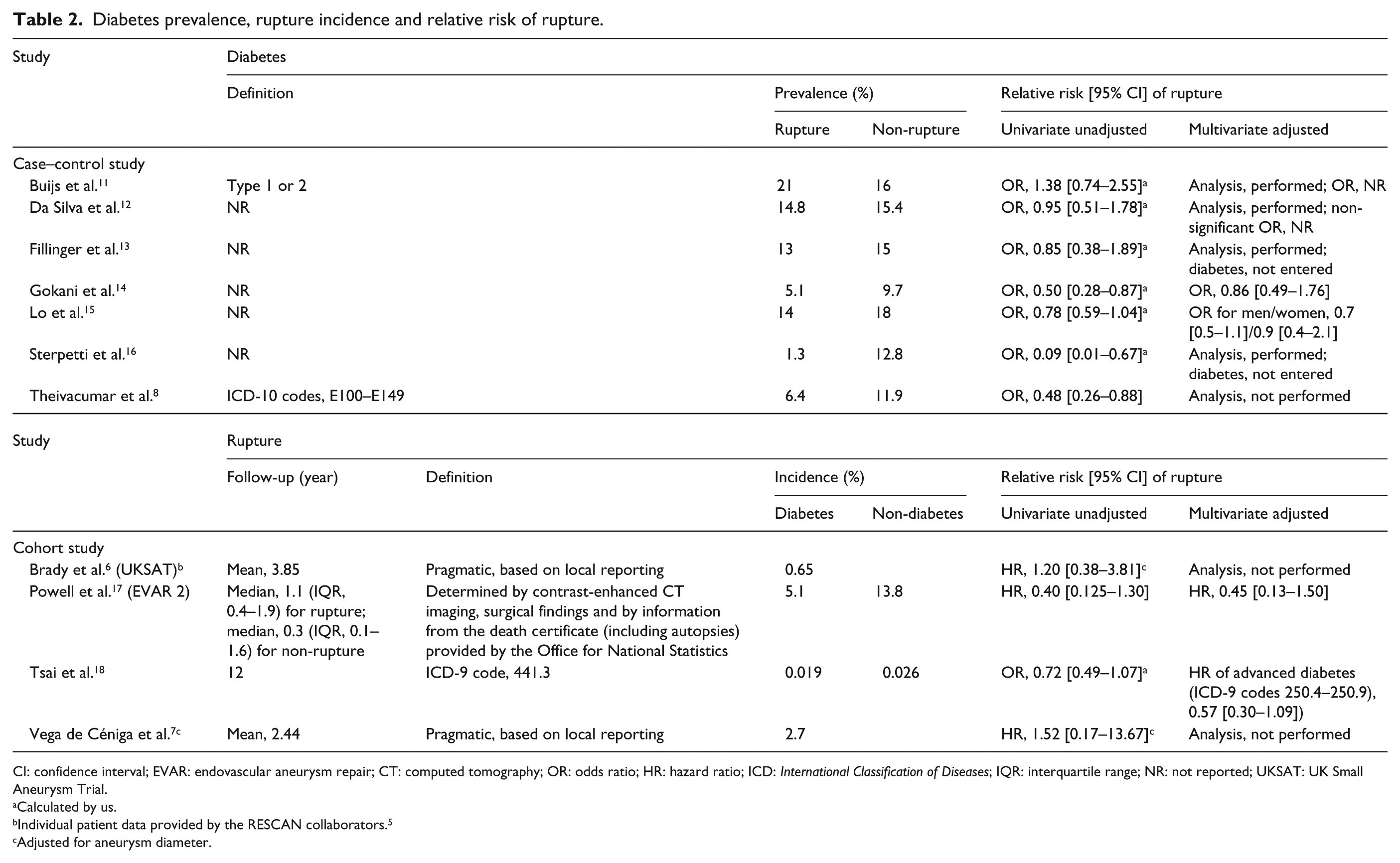
CI: confidence interval; EVAR: endovascular aneurysm repair; CT: computed tomography; OR: odds ratio; HR: hazard ratio; ICD: International Classification of Diseases; IQR: interquartile range; NR: not reported; UKSAT: UK Small Aneurysm Trial.
Calculated by us.
Individual patient data provided by the RESCAN collaborators. 5
Adjusted for aneurysm diameter.
Multivariate-adjusted ORs/HRs were available in four studies,14,15,17,18 whereas univariate-unadjusted ORs/HRs only in seven studies.6–8,11–13,16 Two8,16 of these seven studies provided significantly lower diabetes prevalence in AAA rupture (i.e. significantly lower AAA-rupture prevalence in diabetes), which was sequentially eliminated in sensitivity analyses to assess their impact on the pooled effect estimate. The primary meta-analysis of the nine studies6–8,12,14–18 demonstrated that diabetes was associated with significantly lower prevalence/incidence of AAA rupture (i.e. significantly and negatively associated with AAA rupture) (fixed-effects OR/HR, 0.71; 95% CI, 0.56 to 0.89; p = 0.003; Figure 1). There was no between-study heterogeneity of results (p = 0.40) and accordingly little difference in the pooled result from random-effects modelling (random-effects OR/HR, 0.71; 95% CI, 0.56 to 0.90; p = 0.004.)
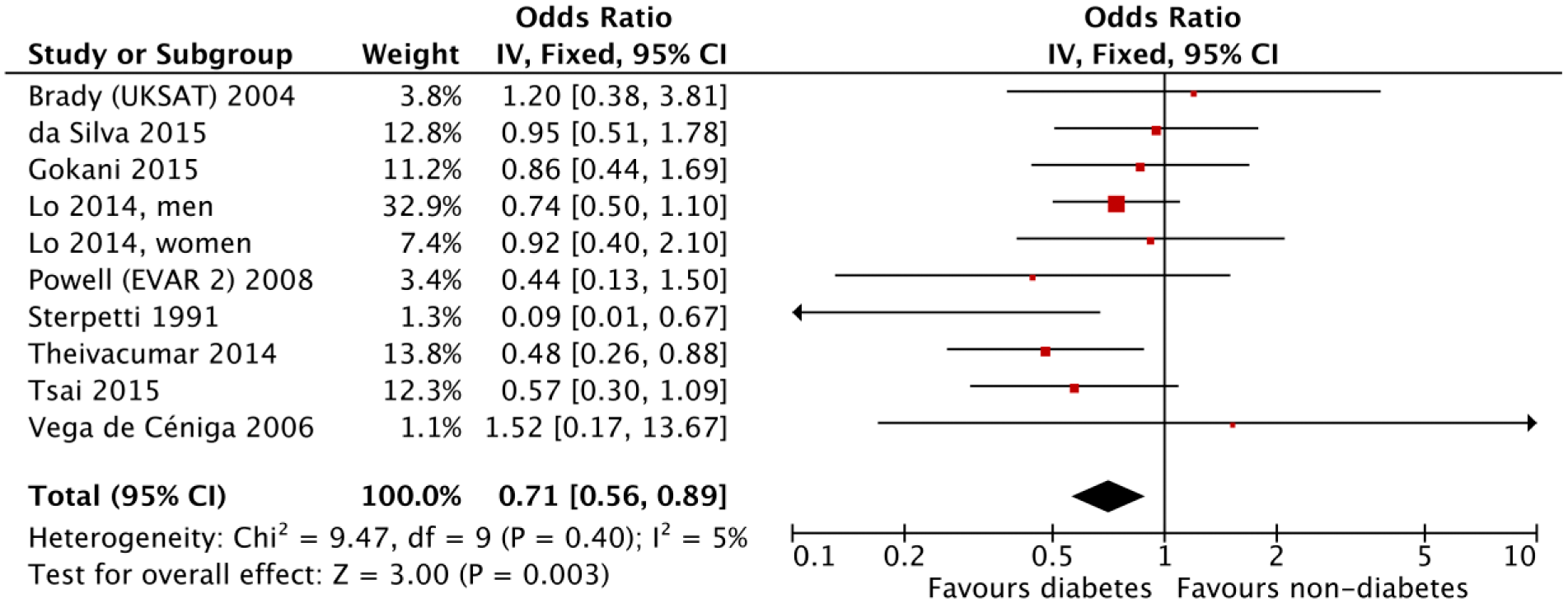
Primary meta-analysis of odds/hazard ratios for abdominal aortic aneurysm (AAA) rupture from nine studies reporting a relative risk of exclusive ruptured (not including non-ruptured symptomatic) AAA. CI: confidence interval; EVAR: endovascular aneurysm repair; IV: inverse variance; UKSAT: UK Small Aneurysm Trial.
To assess the impact of qualitative heterogeneity in study design and patient selection on the pooled effect estimate, we performed several sensitivity analyses. First, we excluded a study by Lo et al. 15 with the greatest weight (30.4% and 7.8% for men and women, respectively). Without it, there was still a statistically significant benefit for diabetes (p for heterogeneity = 0.26; fixed-effect OR/HR, 0.67; 95% CI, 0.50 to 0.90; p for effect = 0.007; random-effects OR/HR, 0.67; 95% CI, 0.47 to 0.94; p for effect = 0.02). Second, we excluded both study by Theivacumar et al. 8 and that by Sterpetti et al., 16 which reported the significantly lower unadjusted prevalence of AAA rupture in diabetes. Combining the remaining seven studies generated an attenuated but still statistically significant result favouring diabetes (fixed-effect and random-effects OR/HR, 0.78; 95% CI, 0.61 to 0.99; p for effect = 0.04; p for heterogeneity = 0.86). In general, exclusion of any single study from the analysis did not substantively alter the overall result of our analysis (online Appendix 3). Furthermore, the secondary meta-analysis of all the 11 studies (adding two studies11,13 in which non-ruptured symptomatic AAA was included in the rupture group) also demonstrated that diabetes was associated with significantly lower prevalence/incidence of AAA rupture (p for heterogeneity = 0.26; fixed-effect OR/HR, 0.77; 95% CI, 0.63 to 0.95; p for effect = 0.01; random-effects OR/HR, 0.77; 95% CI, 0.61 to 0.98; p for effect = 0.03). To assess publication bias in the primary meta-analysis, we generated a funnel plot of the logarithm of effect size (OR/HR) versus the precision (reciprocal of standard error (SE)) for each study (online Appendix 4). There was no evidence of significant publication bias (two-tailed p with continuity correction = 1.00 by the adjusted rank-correlation test; 9 two-tailed p = 0.60 by the linear regression test 10 ).
Discussion
The results of our analysis suggest the negative association of diabetes with AAA rupture as well as presence 3 and growth, 4 which was robust in sensitivity analyses. Only two studies were able to demonstrate a statistically significant benefit to diabetes, likely due to systematic under-powering (as reflected in the wide CIs and lack of statistical significance) of studies in the design phase and primarily due to the small number of events (ruptures).
Diabetes is negatively associated with AAA presence.3,19 In a recent meta-analysis by De Rango et al. 19 of 17 large population prevalence studies, preferring to use data adjusted for local confounders at each study level and combining the adjusted data, there was a significant inverse association between diabetes and AAA (OR, 0.80; 95% CI, 0.70 to 0.90; p = 0.0009). Another recent meta-analysis 3 of adjusted estimates from 13 studies also demonstrated that diabetes was significantly associated with lower prevalence of AAA (OR, 0.59; 95% CI, 0.52 to 0.67; p < 0.00001). Furthermore, diabetes is also negatively associated with AAA growth.4,5 The RESCAN meta-analysis 5 of 6268 individual patient data from 10 studies demonstrated that diabetics had growth rates that were on average 0.51 ± 0.10 (SE) mm/year slower than those of non-diabetics after adjustment for all demographics, medical history and drug history. A recent meta-analysis 4 of 19 studies also demonstrated a statistically significant slower growth rates in diabetic patients than in non-diabetic patients (unadjusted standardized mean difference (SMD), −0.32; 95% CI, −0.40 to −0.24; p < 0.00001; adjusted SMD, −0.29; 95% CI, −0.41 to −0.18; p < 0.00001).
Although diabetes is negatively associated with all of AAA presence, 3 growth 4 and rupture (as demonstrated in the present analysis), discrepancy between the association of comorbidity with AAA presence and that of the same comorbidity with AAA growth could be identified. Although CAD is positively associated with AAA presence,1,2 it is negatively associated with AAA growth. 20 A previous meta-analysis by Cornuz et al. 1 of six population-based risk factor studies of AAA showed that a history of myocardial infarction was a major risk factor or risk indicator for screening-detected AAA (OR, 2.30; 95% CI, 1.92 to 2.75). A recent meta-analysis by Li et al. 2 of 10 epidemiological studies also showed that CAD was a risk factor for AAA (OR, 1.82; 95% CI, 1.65 to 2.00). Another recent meta-analysis 20 of 20 studies, however, demonstrated a statistically significant association of CAD with slower AAA growth rates (SMD, −0.06; 95% CI, −0.12 to −0.0027; p = 0.04).
Although PAD is also positively associated with AAA presence,1,2 it is negatively associated with AAA growth. 21 The meta-analysis by Cornuz et al. 1 of eight population-based risk factor studies of AAA showed that a history of PAD was a major risk factor or risk indicator for screening-detected AAA (OR, 2.48; 95% CI, 2.10 to 2.92). The meta-analysis by Li et al. 2 of three epidemiological studies also showed that claudication was a risk factor for AAA (OR, 3.00; 95% CI, 1.74 to 5.19). A recent meta-analysis of 11 studeis, 21 however, demonstrated a statistically significant association of PAD with lower AAA growth rates (SMD, −0.17; 95% CI, −0.25 to −0.09; p < 0.0001).
Although chronic obstructive pulmonary disease (COPD) is also positively associated with AAA presence, 22 it is not associated with AAA growth. 23 A recent meta-analysis 22 of seven case–control and four population-based AAA-screening studies demonstrated a statistically significant 1.78-fold (OR, 1.78; 95% CI, 1.38 to 2.30; p < 0.00001) increased prevalence/incidence of COPD in patients with AAA relative to subjects without AAA (i.e. a statistically significant 1.78-fold increased prevalence/incidence of AAA in patients with COPD relative to subjects without COPD). Another recent meta-analysis 23 of 10 studies, however, demonstrated that COPD was not associated with AAA growth rates (SMD, 0.04; 95% CI, −0.07 to 0.15; p = 0.50).
The above-mentioned findings (the same comorbidity is positively associated with AAA presence but not or even negatively associated with AAA growth) suggest that accelerated mechanisms regarding expansion of an existing AAA may be different from those regarding initial formation of an AAA. Regrettably, there has been little knowledge regarding an association of CAD, PAD or COPD with AAA rupture. Whereas, the negative associations of diabetes with all of AAA presence, 1 growth 2 and rupture (as demonstrated in the present analysis) suggest that decelerated mechanisms regarding expansion and exploding of an existing AAA may be the same as those regarding initial formation of an AAA. Although primary abdominal wall hernia 24 and simple renal cyst 25 are also positively associated with AAA presence, there has been no knowledge regarding an association of these comorbidities with AAA growth or rupture.
Conclusion
Diabetes is negatively associated with rupture as well as presence and growth of AAA. Although diabetes is a major risk factor of CAD and PAD, both CAD and PAD are positively associated with AAA presence. Further investigations would be required to understand precise mechanisms regarding the negative association of diabetes with AAA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.