
Abstract
Background:
Left atrial appendage closure is a preventive treatment of atrial fibrillation–related thrombo-embolism. Patients with diabetes mellitus have increased risk for a negative outcome in percutaneous cardiac interventions. We assessed whether percutaneous left atrial appendage closure is safe and effective in patients with diabetes mellitus.
Methods:
We included 78 patients (mean age of 74.4 ± 8.3 years) with indication for left atrial appendage closure in an open-label observational single-centre study.
Results:
Patients with diabetes mellitus (n = 31) were at higher thrombo-embolic and bleeding risk (CHA2DS2-VASc: 4.5 ± 0.9, HAS-BLED: 4.7 ± 0.7) compared to patients without diabetes mellitus (n = 47, CHA2DS2-VASc: 3.5 ± 1.0, HAS-BLED: 4.1 ± 0.8; p < 0.001 for both). Pre- and periprocedural risk was elevated in patients with diabetes mellitus (Euro II-Score: 6.6 ± 3.7 vs 3.9 ± 1.9, p < 0.01; Society of Thoracic Surgeons (STS)-Score: 4.0 ± 2.5 vs 2.6 ± 1.2, p < 0.01). Procedural success was similar. Periprocedural major adverse cardiac and cerebrovascular events occurred in one patient from the control group (2.1%), whereas patients with diabetes mellitus had no events (p = 0.672). Follow-up of 6 months revealed no bleeding complication in both groups. No stroke occurred in follow-up, and left atrial appendage flow velocity reduction (55.6 ± 38.6 vs 51.4 ± 19.1 cm/s, p = 0.474) and rate of postinterventional leakage in the left atrial appendage were comparable (0% vs 2.1%, p = 0.672).
Conclusion:
Despite patients with diabetes mellitus are high-risk patients, the outcome of percutaneous left atrial appendage closure is similar to patients without diabetes mellitus.
Keywords
Introduction
Patients with non-valvular atrial fibrillation (AF) have a four- to fivefold increase in stroke rate.1,2 In this setting, the left atrial appendage (LAA) has been found to be the source of embolic thrombus formation causing stroke in 90% of cases. 3 Stroke prevention in patients with non-valvular AF has largely been based on the use of oral anticoagulation (OAC) with warfarin, which reduces the risk of stroke by 60%, 4 and more recently, on the use of novel anticoagulants (NOACs).5,6 However, the risk of life-threatening bleeding complications ranging from 1.4% to 3% per year,7,8 drug interactions and narrow therapeutic windows constrain widespread usage of warfarin. Current guidelines recommend the primary use of novel anticoagulants; however, they only offer modest improvements in bleeding risk.9 –11 NOACs are dependent on the kidney function for elimination and cause an increased bleeding risk in renal impairment. Some are even contraindicated in patients with advanced chronic kidney disease and those on dialysis.12,13 Therefore, they may only be used in 40%–50% of patients at increased risk for stroke.1,14 To date, there are still many patients who are poor candidates for OAC.
For these reasons, device-based therapies for left atrial appendage closure (LAAC) are advocated as a potential therapeutic option in current guidelines. 9 Percutaneous LAAC has emerged to be an effective therapeutic alternative for patients suffering from bleeding complications under OAC.15,16 Previous studies were limited by small sample sizes, assessed patients treated with dedicated or non-dedicated devices and included centres with variable operator experience.15–19
So far, one unresolved issue for this percutaneous procedure is optimal patient selection. Little is known about patient-related predictors of periprocedural complications during LAAC. Many of the high-risk patients present with diabetes mellitus (DM), which is known to worsen the outcome in patients referred to percutaneous coronary intervention (PCI), cardiac surgery or transcatheter structural interventions.20–23 The underlying mechanisms involve increased platelet activity, endothelial dysfunction, impaired wound healing and a higher risk for infections as the main determinants.24–27 Furthermore, the periprocedural risk is increased by the typical diabetic comorbidities such as impaired renal function or coronary artery disease (CAD). The impact of DM on percutaneous LAAC outcome is not known. We therefore sought to assess whether percutaneous LAAC is safe and effective in patients with DM.
Methods
Patient population and study design
A total of 78 consecutive patients with AF and indication for LAAC in the Department of Cardiology and Vascular Medicine at the West-German Heart and Vascular Center Essen between 2010 and 2016 were included in this observational single-centre study. Procedures were performed using an AMPLATZER™ device (St. Jude Medical, Saint Paul, MN, USA).
Patients were grouped according to the presence of type II DM (oral medication or on insulin therapy). The objective of the study was to evaluate the safety and efficacy of the percutaneous LAAC procedure in patients with DM with a follow-up of 6 months. Study procedures were in accordance with the Declaration of Helsinki and the Institutional Ethics Committee of the University of Duisburg-Essen, who approved the study protocol.
LAAC procedure
The procedure and the LAAC system have previously been described in detail.28,29 The LAAC procedures were performed by experienced operators under transesophageal echocardiography (TOE) and fluoroscopy for guidance using dedicated AMPLATZER devices [first-generation AMPLATZER cardiac plug (ACP) and second-generation AMPLATZER Amulet, St. Jude Medical, Saint Paul, MN, USA]. Before device implantation, LAA flow velocity and presence of atrial septum defect were evaluated by TOE. After a femoral venous access, the left atrium was accessed by means of transseptal puncture in the majority of patients or through an atrial septal defect, if deemed feasible. 30 According to manufacturer instructions, device oversizing of 3–5 mm for the ACP and 2–4 mm for the AMPLATZER Amulet, relevant to the landing zone (defined fluoroscopically and on periprocedural TOE) was typically applied.
Antithrombotic medication
OAC was interrupted preprocedural if previously administered. Periprocedural heparin was applied after transseptal puncture under control of activated clotting time (ACT). Consistent with manufacturer recommendations as well as with previous evidence with AMPLATZER devices,9,17 OAC was discontinued immediately following successful LAAC, and dual antiplatelet therapy was initiated, consisting of aspirin 100 mg and clopidogrel 75 mg daily for 3 (n = 18) to 6 months (n = 60). In some cases, phenprocoumon was applied postprocedural for 45 days (n = 27) additionally to aspirin 100 mg and clopidogrel 75 mg.
Data collection and definitions
Patient and procedural characteristics, imaging findings, laboratory results, in-hospital and follow-up data up to 6 months after LAAC were collected in a dedicated database. Blood samples for biochemistry and haematology analysis were taken before the procedure. TOE was performed before the procedure, periprocedural and during follow-up. Procedural success was defined as successful implantation of the device in the LAA. Clinical outcome parameters for follow up after 6 months were bleeding complications and stroke without anticoagulation.
In-hospital complications were reported for both groups. Major adverse cardiac and cerebrovascular events (MACCE) were defined to include death, ST-elevation myocardial infarction, stroke and procedure-related reoperation.
Further complications included procedure-related major or life-threatening bleeding, device embolization, major access-vessel complication, need for cardiovascular surgery, need for cardiopulmonary resuscitation and serious pericardial effusion (i.e. haemodynamically significant effusion prompting intervention or resulting in prolonged hospitalization). Peripheral vascular complications were defined as minor vascular complications according to Valve Academic Research Consortium 2 (VARC 2) criteria. 31 A major vascular complication was defined according to VARC 2 as overt bleeding either associated with a drop in haemoglobin level of at least 3.0 g/dL or requiring transfusion of two or three units of whole blood, or causing hospitalization, or permanent injury, or requiring surgery and does not meet criteria of life-threatening or disabling bleeding. The study’s primary endpoint was the combined safety endpoint of device- and procedure-related complications during hospitalization or within 6 months post-procedure in patients with DM.
Statistical analysis
Continuous data were expressed as mean ± standard deviation (SD) and compared with unpaired Student’s t-test or Mann–Whitney U test if not normally distributed. Normality was checked with the Kolmogorov–Smirnov test. Categorical variables were evaluated as percentage and compared with the chi-square test or Fisher’s exact test. Statistical analysis was performed with SPSS Statistics 22 (IBM). A p-value <0.05 was considered to be significant.
Results
Study population
We enrolled 78 patients (mean age of 74.4 ± 8.3 years, 61.5% male) with non-valvular AF and contraindication for anticoagulation. Indications for percutaneous LAAC were bleeding complications under anticoagulation (n = 49), contraindication to anticoagulation (n = 13) or other reasons that made patients ineligible for anticoagulation, for example, intolerance of anticoagulation (e.g. hepatic injury, diarrhoea or severe nausea; n = 8), strong tendency to fall (n = 6) or insufficient adjustment of phenprocoumon (labile INR; n = 2). A total of 31 patients (39.7%) presented with type II DM with either oral medication or insulin therapy. Patients with DM revealed higher rates of CAD (80.6% vs 57.4%, p = 0.03). Regarding the other baseline parameters, the two groups did not differ. Baseline characteristics are summarized in Table 1.
Baseline characteristics of patients undergoing LAAC grouped according to the presence of type II diabetes mellitus.
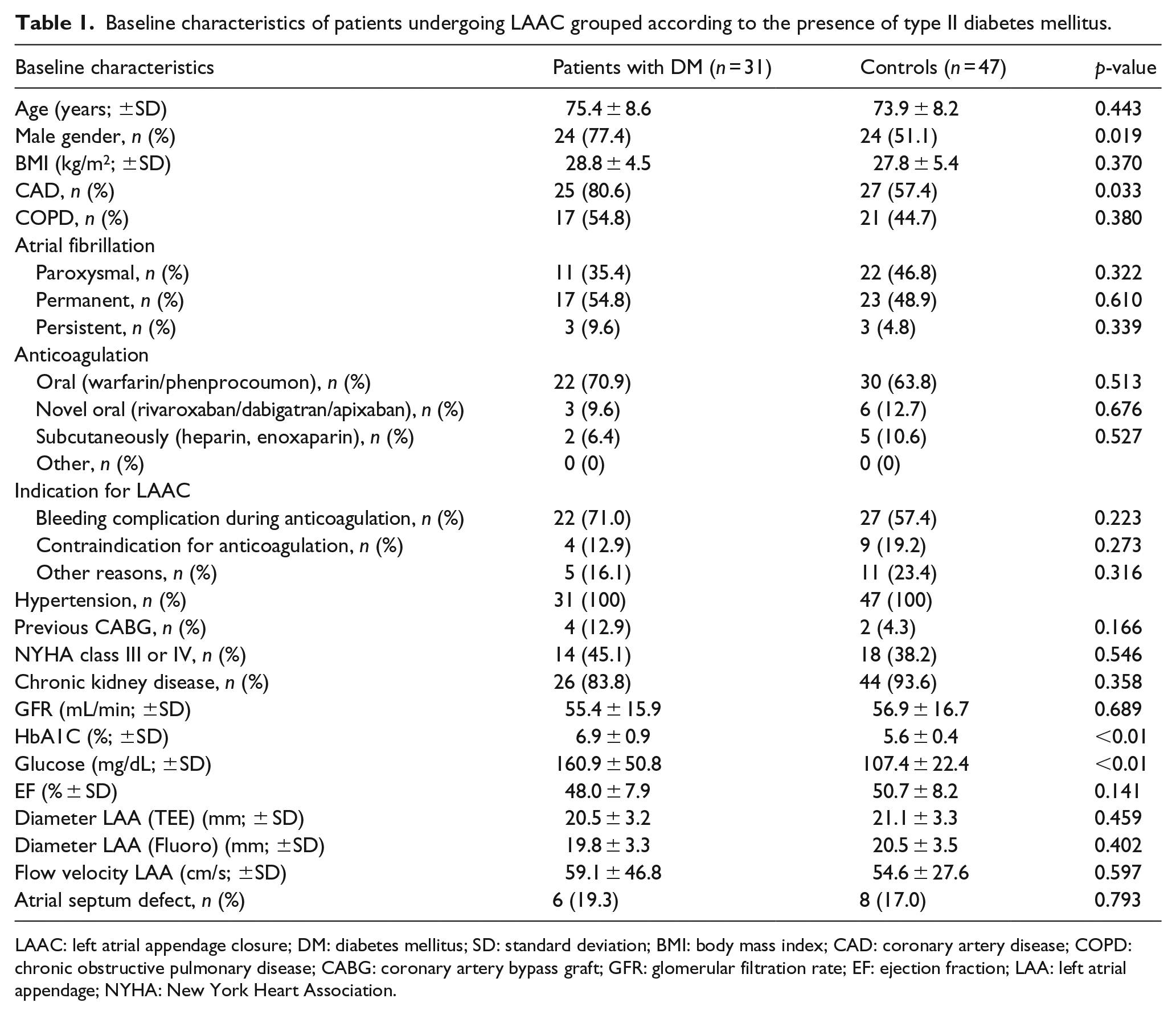
LAAC: left atrial appendage closure; DM: diabetes mellitus; SD: standard deviation; BMI: body mass index; CAD: coronary artery disease; COPD: chronic obstructive pulmonary disease; CABG: coronary artery bypass graft; GFR: glomerular filtration rate; EF: ejection fraction; LAA: left atrial appendage; NYHA: New York Heart Association.
Risk stratification
Patients with DM were at higher risk for stroke (CHA2DS2-VASc: 4.5 ± 0.9 vs 3.5 ± 1.0, p < 0.01) and bleeding complications (HAS-BLED: 4.7 ± 0.7 vs 4.1 ± 0.8; p < 0.01) than patients without DM. Furthermore, pre- and periprocedural risk was significantly elevated in patients with DM (Euro II-Score: 6.6 ± 3.7 vs 3.9 ± 1.9, p < 0.01; STS-Score: 4.0 ± 2.5 vs 2.6 ± 1.2, p < 0.01; Figure 1).
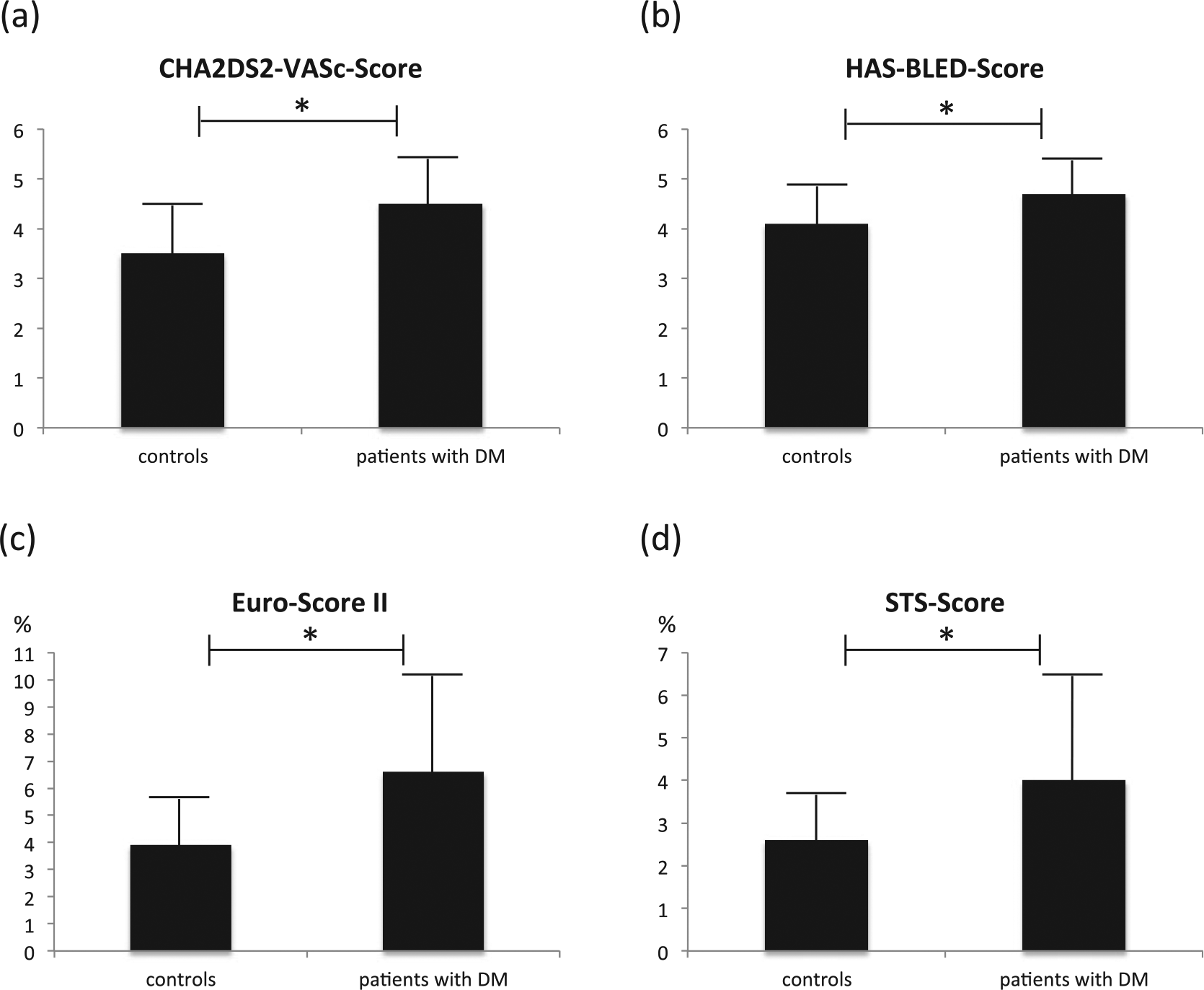
Pre- and periprocedural risk stratification of closure of left atrial appendage in controls versus patients with DM: (a) CHA2DS2-VASc-Score, (b) HAS-BLED-Score, (c) Euro-Score II and (d) STS-Score.
Primary endpoint – safety
The primary endpoint of this study was related to safety with regard to successful device implantation, in-hospital complication rate and mortality during follow-up. Overall procedural success was achieved in 93.6% (n = 73). Rate of successful device implantation was similar in patients with DM compared to controls (Figure 1). One patient in the control group had to undergo surgery for significant pericardial effusion.
At the time of follow-up, overall survival was 98.7% (n = 77) with no death after discharge from hospital in both groups (Table 2). Periprocedural stroke occurred in none of the interventions. Complications were defined as MACCE (patients with DM vs controls: 0% vs 2.1%, p = 0.672), device embolization rate (0% vs 2.1%, p = 0.672), major access-vessel complication (0% vs 0%), need for cardiovascular surgery (0% vs 2.1%, p = 0.672), need for cardiopulmonary resuscitation (0% vs 0%), serious pericardial effusion (0% vs 2.1%, p = 0.672), peripheral major and minor vascular complications (0% vs 0%) and acute kidney injury stage III (0% vs 0%). Within 72-h postprocedural, no death occurred. Three-month mortality rate was 2.1% in patients without DM due to one fatal device embolization with need for cardiovascular surgery and fatal outcome after 7 days. No patient died in the diabetes group (p = 0.672). After follow-up of 6 months, no bleeding complications or stroke occurred in neither groups (Table 3).
Periprocedural results of patients undergoing closure of the left atrial appendage grouped according to the presence of type II diabetes mellitus.
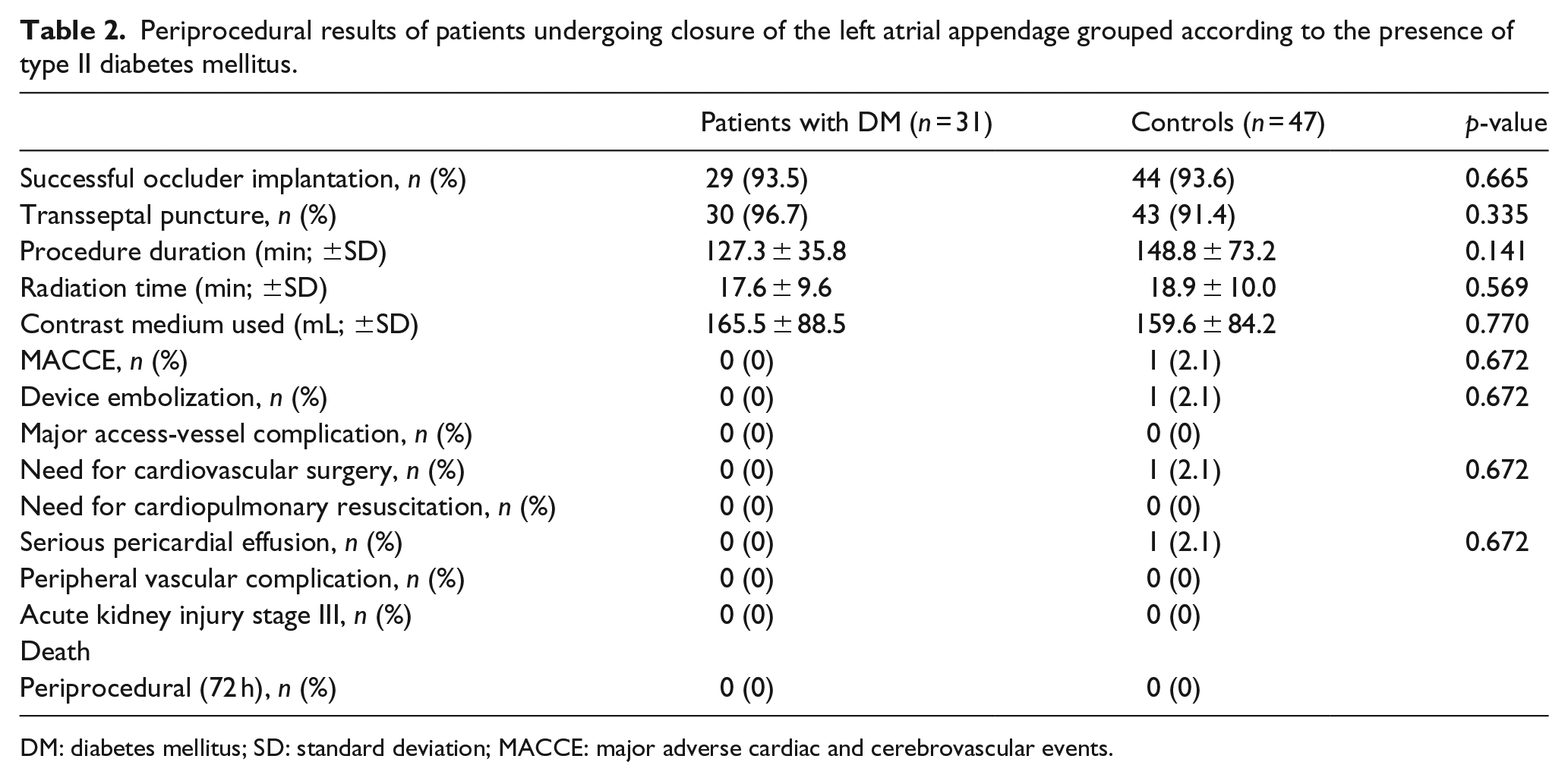
DM: diabetes mellitus; SD: standard deviation; MACCE: major adverse cardiac and cerebrovascular events.
Post-procedural results of patients after closure of the left atrial appendage grouped according to the presence of type II diabetes mellitus after 6 months.
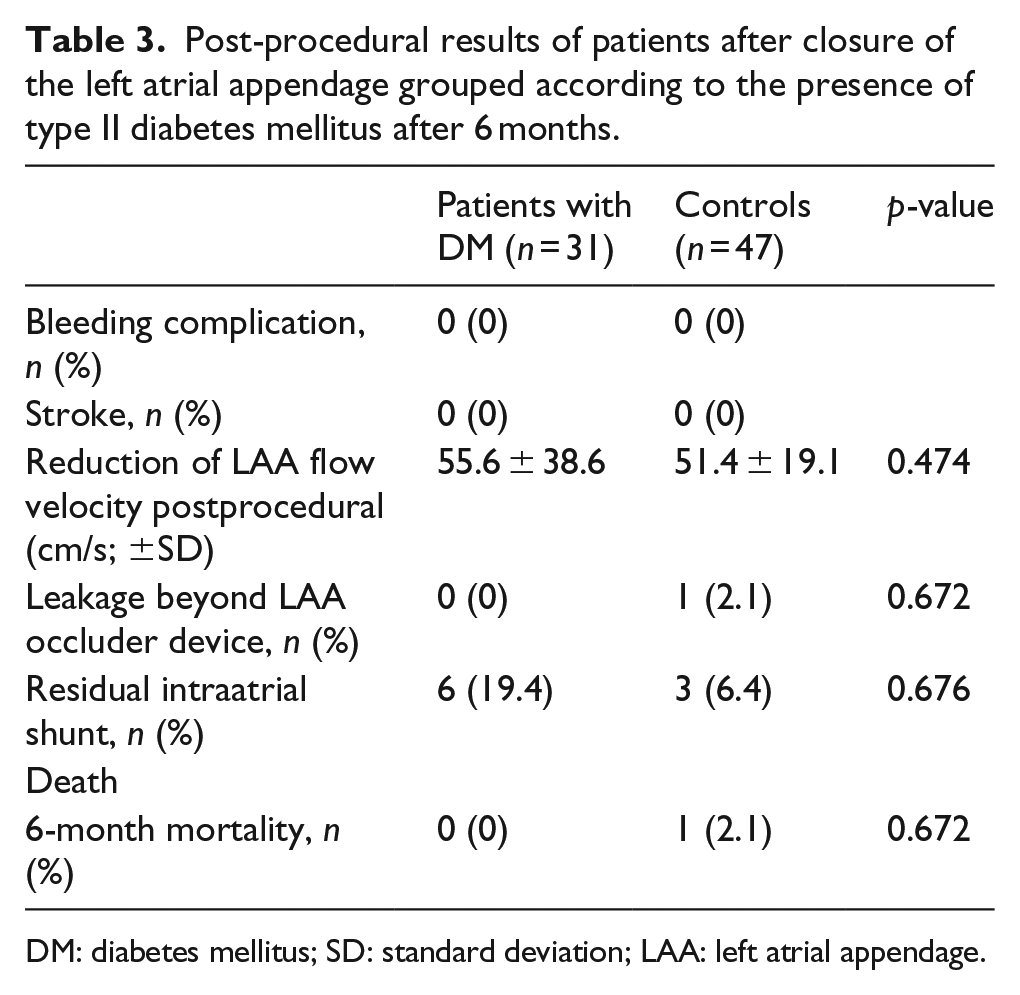
DM: diabetes mellitus; SD: standard deviation; LAA: left atrial appendage.
Secondary endpoint – efficacy
The secondary endpoints were related to efficacy with regard to procedure duration (patients with DM vs controls: 127.3 ± 35.8 vs 148.8 ± 73.2 min, p = 0.141), transseptal puncture (30/31 (96.8%) vs 43/47 (91.5%), p = 0.335), atrial septal defect feasible for LAAC (1/31 (3.2%) vs 4/47 (8.5%), p = 0.589), radiation time (17.6 ± 9.6 vs 18.9 ± 10.0 min, p = 0.569) and applied amount of contrast medium (165.5 ± 88.5 vs 159.6 ± 84.2 mL, p = 0.77; Table 2).
After follow-up of 6 months, changes in cardiac parameters were observed in both groups with comparable outcomes (Figure 2). Significant reduction of LAA flow velocity was seen in patients with DM as well in controls. Leakage beyond the LAA occluder device was observed in none of the patients with DM versus 2.1% in the controls (p = 0.672). Residual intraatrial shunt after transseptal puncture was documented in six (19.4%) patients with DM versus three (6.4%) controls (p = 0.676).
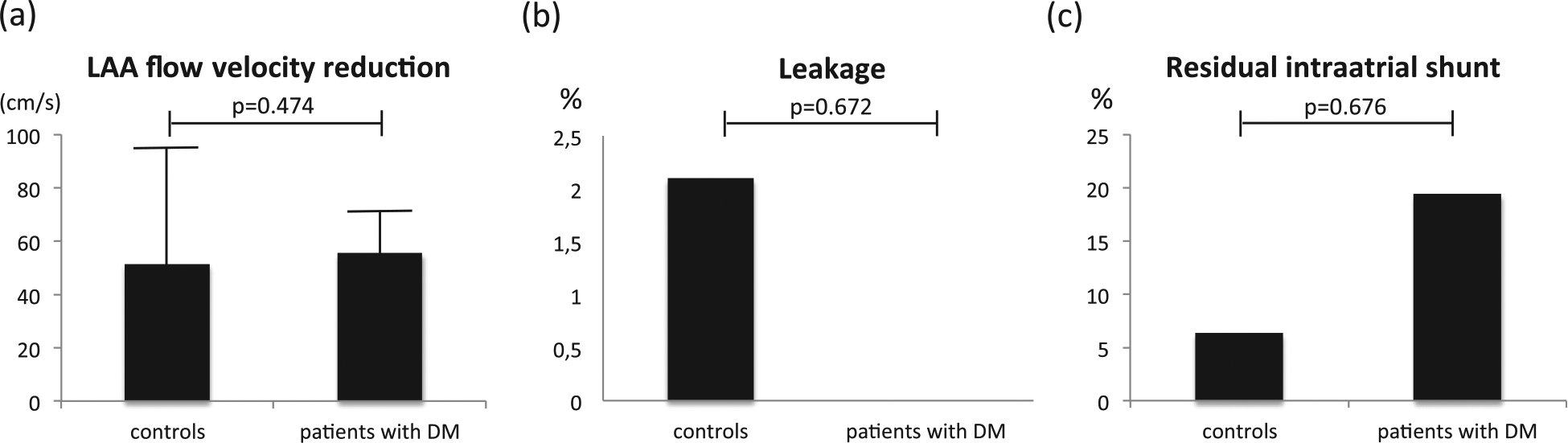
Changes in cardiac parameters after short-term follow-up of 6 months in patients undergoing percutaneous closure of the left atrial appendage (LAA): (a) LAA flow velocity reduction, (b) leakage in LAA during follow-up and (c) residual intraatrial shunt during follow-up.
Discussion
Percutaneous device-based LAAC is a rising treatment option for stroke prevention in patients with non-valvular AF who are not eligible for long-term OAC.23,32,33 Despite a clinical benefit by LAAC that appears to be non-inferior to OAC, careful patient selection for LAAC is paramount. Especially in high-risk patients, such as patients with DM, there remain concerns regarding the procedural safety of this preventive intervention. Patients with DM reveal increased platelet activity, endothelial dysfunction, impaired wound healing and a higher risk for infections.24 –27 Furthermore, the periprocedural risk is increased by the typical diabetic comorbidities such as impaired renal function or CAD. In this study, we analysed a cohort of consecutive patients undergoing LAAC, focusing on peri- and postprocedural adverse events and early outcome in patients with DM.
The key finding of our study is that despite significant elevated pre- and periprocedural risk, LAAC is safe and feasible in patients with DM. In our study, periprocedural risk was estimated using the STS-Score and Euro-Score. 20 Successful device implantation rate as well as peri- and postprocedural complication rate was similar to controls.
Patients with diabetes are at higher risk when undergoing PCI or cardiac surgery.21 –23 We are aware that both STS-Score and Euro-Score are scoring systems feasible to calculate the procedural risk of interventional and surgical cardiac interventions and so far not used for risk assessment before percutaneous LAAC. However, interventional closure of the LAA is a rising technique, which has been performed more frequently in the last years. The fact that the ageing process of our population and the rate of patients with AF ineligible for anticoagulation will increase in the future and makes it necessary to identify a useful scoring system for procedural risk assessment of patients undergoing LAAC.
Interventional LAAC with the AMPLATZER devices has been shown to be safe and feasible; previous studies report diminishing rates of major events, starting from 7% in the initial European experience report, 17 5.8% for in-hospital events 19 and finally 5% in the multicentre AMPLATZER registry. 16 In randomized trials with the WATCHMAN™ device, early adverse events were more frequent at initial stages. 11 These complication rates may reflect the morbidity of the patients who are referred to LAAC procedure and the importance of careful patient selection and risk stratification. The role of diabetes in interventional LAAC has not been investigated so far.
Intriguingly, patients with diabetes revealed a significantly higher thrombo-embolic as well as bleeding risk compared to controls. This might suggest that these patients have a greater benefit through LAAC-guided stroke prevention. Clearly, this should be investigated in further studies.
In our study, population none of the patients with DM died within 6 months of postinterventional follow-up. Successful device implantation was identical in the patients with DM compared to patients without DM (93.5% vs 93.6%). Overall complication rate was low in our study population, which has also been proved in other studies and confirms the safety of the procedure. However, complication rate of patients with DM was comparable to the control group. Previous studies have identified DM to be a risk factor for mortality after surgical approach.34,35 Rates for unsuccessful surgical LAAC have been described to be up to 60%, 36 while rates of reoperation for bleeding risks range between 0% and 10.9%. 10
Echocardiographic evaluation after 6 months of follow-up showed a good result with a significant reduction of LAA flow velocity and correct location of the device in all patients including patients with DM.
Since DM is a known risk factor for several patient outcome parameters, it seems not to be a risk factor for the procedure of interventional LAAC or one of its follow-up parameters.
Limitations
LAAC is safe and event rates are low. However, our sample size is small (n = 78) and follow-up time is limited to 6 months. A prospective randomized study with more patients and longer follow-up time is needed. Patients should be classified concerning the duration of diabetes and diabetes-induced comorbidities such as advanced chronic kidney disease. Patients on dialysis represent a collective of high-risk patients for cardiovascular interventions with contraindication for NOACs and warfarin, who should be investigated more detailed in a separate analysis.
In our study, we used exclusively dedicated AMPLATZER devices (ACP and Amulet, St. Jude Medical, Saint Paul, MN, USA) for LAAC. So far, randomized comparison of LAAC with warfarin has only been performed with the WATCHMAN device (Boston Scientific, Marlborough, MA, USA). A study using both these most widely used devices for LAAC is needed to investigate our analysis in a comparative setting.
Conclusion
Patients with type II DM have a significantly elevated periprocedural risk. The percutaneous device-based LAAC can be performed safely and effectively in patients with DM.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.