
Abstract
Diabetes is one of the most common metabolic disorders and emerges secondary to an interaction between genetic, environmental and lifestyle factors. This work provides an overview of the impact of smoking on the development of vascular complications in this condition and also provides an overview of the potential role of smoking in predisposition to diabetes. There are many studies documenting the impact of smoking on health (not focused on patients with diabetes), suggesting that the health exposure in these individuals is at least comparable to that observed in the general population. Distinct studies of smoking in patients with diabetes have unambiguously confirmed an increased prevalence and a higher risk of early death associated with the development of macrovascular complications. Smoking is also associated with premature development of microvascular complications and may contribute to the pathogenesis of type 2 diabetes. It has been shown that smoking is a predictor of the progression of glucose intolerance at both the transition from normoglycaemia to impaired glucose tolerance status and the increased risk of developing diabetes. The mechanisms explaining the relationship between smoking and the development of diabetes are not fully understood, although a number of hypotheses have been put forward. Current evidence indicates that smoking cessation is not only important to prevent macrovascular complications in diabetes, but also has a role in limiting microvascular disease and may also facilitate glycaemic management in this condition.
Introduction
Smoking is one of the modifiable risk factors for many chronic conditions, such as cardiovascular disease (CVD), cancer, chronic obstructive lung disease, asthma and diabetes. Smoking cessation is one of the few interventions that can safely and cost-effectively be recommended for individuals with diabetes. In the guidelines from the American Diabetes Association, smoking cessation is recommended as one of the most important steps in preventing the complications of diabetes. 1 Many studies have shown that the adverse effects of smoking on diabetes mellitus are not only related to macrovascular complications but also microvascular disease.2–12
Although smoking is known to decrease body weight, it is associated with central obesity. 13 Substances present in tobacco smoke undoubtedly trigger free radical processes, interfere with vascular homeostasis and proper functioning of the vascular endothelium,14,15 and also increase inflammation/oxidative stress, 16 in addition to directly damaging β-cell function. 17
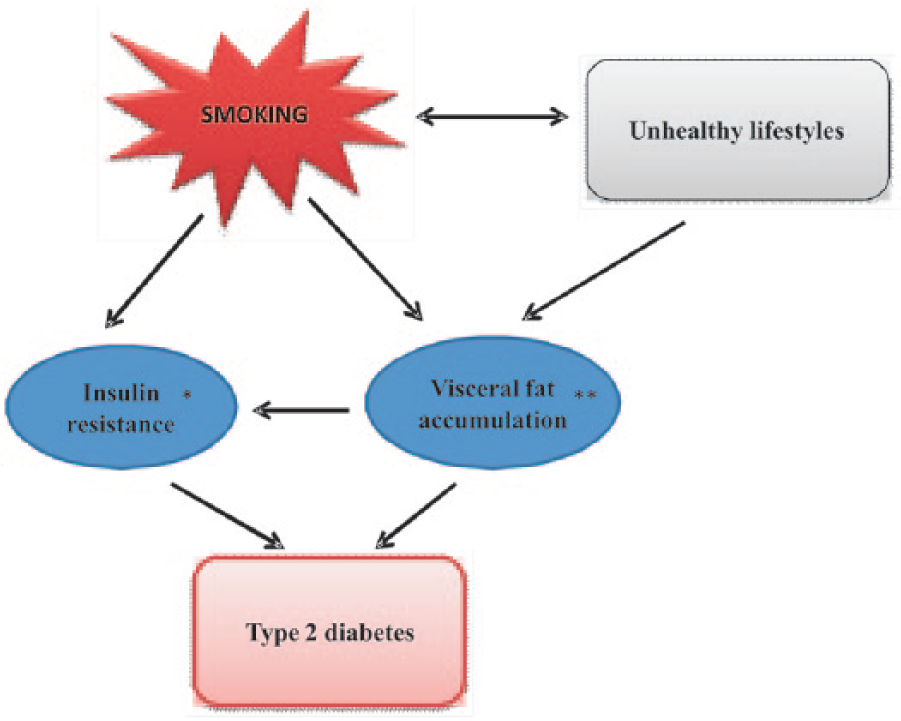
A growing body of the literature has shown links between tobacco use and the development of diabetes. However, this literature is wide ranging and complex as tobacco products such as cigarettes contain 7357 chemical compounds and 1015 to 1017 free radicals, and this is in addition to the well-known compounds such as carbon monoxide, tar, arsenic, lead and nicotine,18–22 leading to multiple pathways that may be involved in the pathogenesis. To complicate matters, each of these pathways is neither mutually exclusive nor linear, and there are a vast number of interactions between chemicals, and interconnectivity between the inflammatory and biochemical pathways that they induce (Figure 1). Since nicotine is the critical substance which exerts most of the adverse effects of smoking, we will concentrate on the role of this substance in this review.
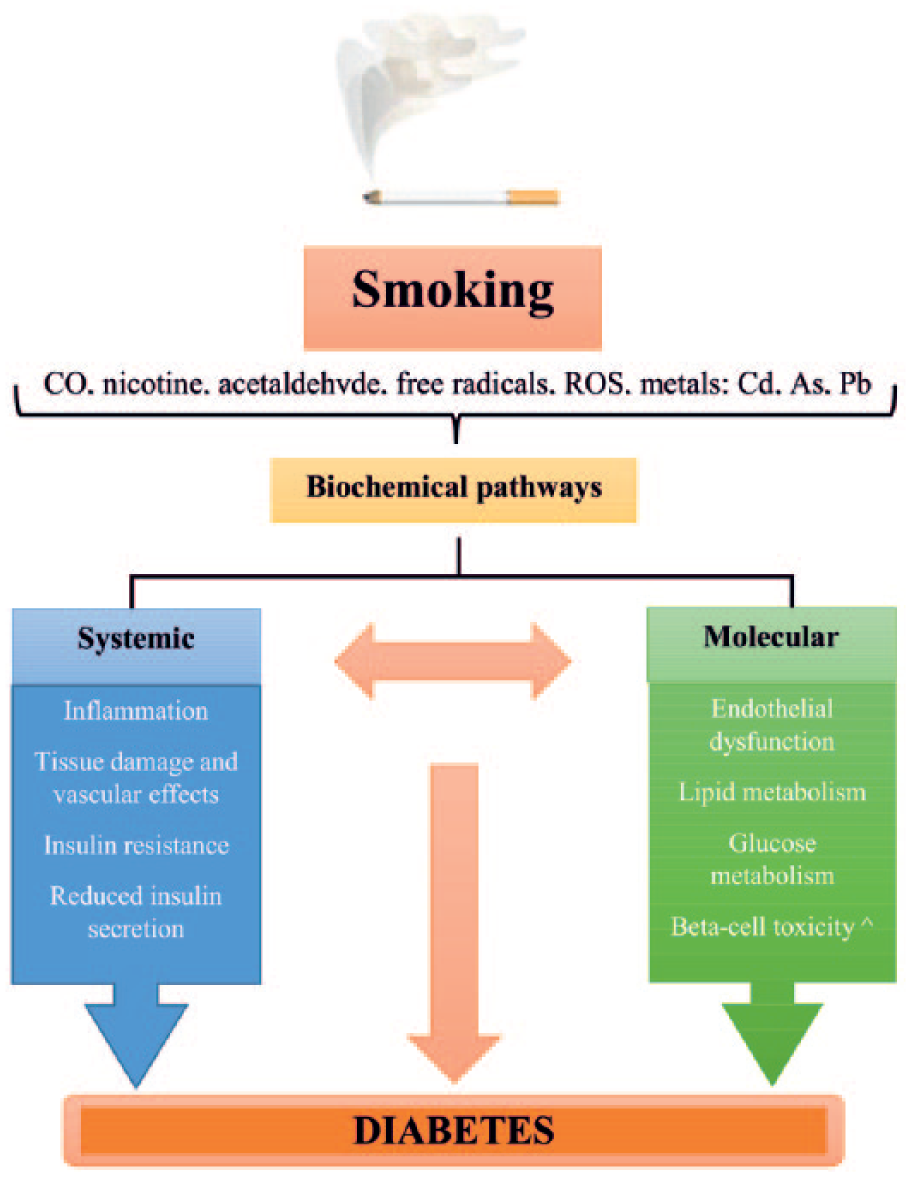
Summary of pathways that link smoking cigarettes with diabetes pathophysiology.
The prevalence of smoking in youth and adults is still high and remains one of the major health problems. 1 Many previous studies documenting the impact of smoking on health did not discuss separately the results for subgroups of patients with diabetes, suggesting an estimated risk of complications that is similar to the general population. Understanding the hazardous effects of smoking on diabetes mellitus may lead to increased emphasis on smoking prevention and smoking cessation as important strategies in the management of this condition.
The relationship between diabetes and smoking
Diabetes is one of the most common metabolic disorders, underpinned by a combination of genetic, environmental and lifestyle factors. Many epidemiological studies indicate that cigarette smoking is an independent risk factor for type 2 diabetes.23–29
The 5-year-long Insulin Resistance Atherosclerosis Study confirmed the significant effect of cigarette smoking on the development of diabetes in adults. In the analysed study, there were nearly a thousand non-diabetic and declared healthy individuals examined. The study comprised a sample with 25% smoking and 14% non-smoking persons with diabetes. After considering the anthropometric, behavioural, metabolic, gender, race and hypertension-related factors, it was found that the risk of type 2 diabetes for smokers was statistically higher than for non-smokers. In addition, a higher risk of diabetes was observed in smokers with normal glucose tolerance. There was also a positive correlation between the risk of developing type 2 diabetes and smoking duration. Periods of intensive cigarette smoking favour the occurrence of hyperglycaemia, hyperinsulinaemia and hypertension. 23
Other work has also shown that cigarette smoking is a risk factor for type 2 diabetes. Men who smoke more than two packs of cigarettes per day have a 45% higher risk of developing diabetes when compared to men who never smoked. In contrast, women who smoke over 40 cigarettes per day have a risk of developing diabetes that can be as much as 75% higher when compared to non-smoking women. Quitting smoking reduces the risk to the level observed in non-smokers within 5 years for women and more than 10 years for men. 24
Specific studies on the effect of smoking on the risk of diabetes in women have been scarce. The results from the Nurses’ Health Study in the United States (114,247 women, 1,227,589 person-years follow-up) showed that the risk for diabetes in smokers was 1.42 after adjustment for other risk factors. 25 Others have found that current and past smoking are associated with a risk of diabetes mellitus essentially in men, but much less in women, and the relationship between fasting glucose and smoking appears different in men and women. 26 The longitudinal study of Japanese males from 1984 to 1992 estimated the risk of developing type 2 diabetes was increased by threefold in those who smoked 16–25 cigarettes a day compared with those who never smoked, after controlling for other risk factors including alcohol consumption and obesity. 27 A follow-up study of this Japanese male cohort, conducted from 1994 to 1999, has established that the level of consumption and the number of years smoked were positively correlated with the development of type 2 diabetes and also to impaired fasting glucose, which often progresses to type 2 diabetes. 29
The study by Wannamethee et al. has demonstrated similar findings; the researchers studied 7124 men aged 40–59 years over a period of 17 years. The cases of diabetes were determined on the basis of questionnaires sent systematically by the primary care physician. Over the course of the study, 290 cases of diabetes were observed. After taking into account factors such as age, body mass index (BMI), and others influencing the onset of diabetes, cigarette smoking was statistically demonstrated to increase the risk of this disease. In this study, however, there was no significant relationship between the duration of smoking habit and its intensity nor the likelihood of developing diabetes. 28 The association of cigarette smoking with development of type 2 diabetes was documented in Table 1.
The relative risk (RR) of diabetes, current smokers compared with non-smokers.
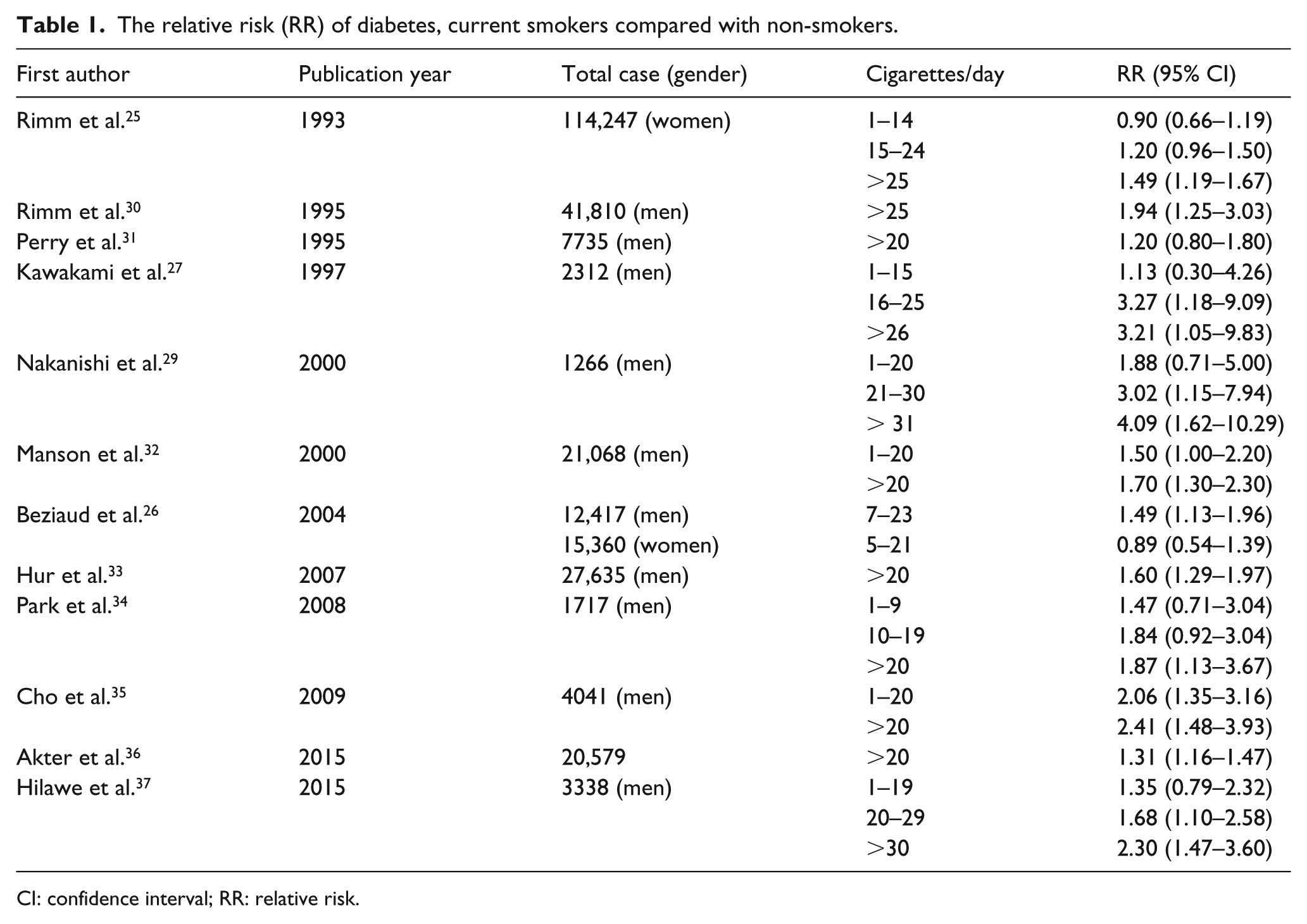
CI: confidence interval; RR: relative risk.
In summary, most studies do find a dose–response relationship between diabetes and cigarette smoking. A meta-analysis of data from 46 studies assessing the association between smoking and the incidence of type 2 diabetes established that active smokers had an increased risk of developing type 2 diabetes compared with non-smokers, with a pooled relative risk (RR) of 1.37 (95% confidence interval (CI): 1.31–1.44). 38 Additionally, this meta-analysis investigated the dose–response effect by dividing the respondents according to the intensity of smoking. The quantitative summary shows that as the smoking intensity increases (defined by the number of cigarettes smoked/day), the RR of diabetes increases in a dose-dependent manner. As shown in Figure 2, the RR increased with higher levels of smoking intensity. When compared with those who had never smoked, former smokers had an RR of 1.14 (95% CI: 1.09–1.19). When compared with non-smokers, light smokers had an RR of 1.25 (95% CI: 1.14–1.37) and heavy smokers had an RR of 1.54 (95% CI: 1.40–1.68). Furthermore, the meta-analysis found that former smokers had a lower risk of developing diabetes than current smokers. 38
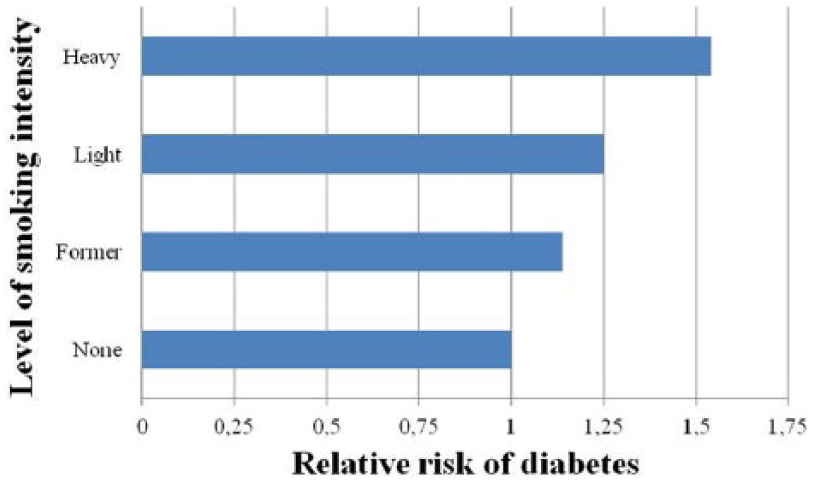
Pooled RR of diabetes associated with smoking intensity. Light smoking defined in most studies as current smoking of 0–19 cigarettes/day and heavy smoking defined in most studies as current smoking of 20 or more cigarettes/day. 38
Therefore, studies published so far show a good correlation between the ‘intensity’ of smoking and the risk of developing diabetes with those quitting smoking having a clear reduction in risk.
Reduced insulin secretion
The presence of neuronal nicotinic acetylcholine receptors (nAChRs) was discovered in the β cells of pancreatic islets. It was found that on the surface of islet cells in the pancreas, there are subunits of nAChRs, such as α-2, α-3, α-4, α-5, α-7 and β-2. Both in the case of acute (60 min) and chronic (48 h) exposure to nicotine, decreased β cell insulin secretion was observed. The findings suggest that nAChRs play an important role in controlling the hormone release by β cells. It was further found that exposure to nicotine concentrations above 1 µmol/L inhibits insulin secretion in isolated human islet cells. 39
These findings indicate that functional nicotinic receptors are present in pancreatic islets and β cells and nicotine could, at least in part, negatively affect pancreatic β-cell function. Thus, the presence of neuronal nicotinic receptors sensitive to nicotine in pancreatic cells may be explained by the mechanism of toxic influence of nicotine on insulin-secreting β cells.
Many animal studies have demonstrated that nicotine may affect the development of pancreatic cells and contribute to the development of diabetes. Several studies have shown that nicotine can increase apoptosis of islet β cells in nicotine exposed animal models. In an experiment using an animal model, the impact of prenatal and postnatal exposure to nicotine on the function of β cells of pancreatic islets was analysed. The study was conducted on pregnant rats that were injected with a solution of hydrogen tartrate nicotine, with the control group being injected with saline. The administration of nicotine and saline continued until the end of lactation, that is, for 21 days after birth. The study revealed that nicotine exposure can cause β-cell dysfunction and increased β-cell apoptosis, mediated via the mitochondrial and/or death receptor pathway, which led to the development of impaired glucose metabolism. 40 Another study indicated that maternally derived nicotine can act via pancreatic nAChRs during foetal and neonatal development, leading to oxidative stress that in turn results in loss of pancreatic β cells. These results support the concept that β-cell apoptosis in foetal and neonatal pancreas can be induced by a direct effect of nicotine via nAChRs, and that this effect may be mediated through increased oxidative stress. 41
Others found that exposure to nicotine during foetal and neonatal life stages caused an increase in body fat and dysglycaemia. In experimental animal models, glucose metabolism disturbances appeared at the age of 7 weeks in rates and persisted until the age of 26 weeks in rats exposed to nicotine during their prenatal and neonatal stages of life, with insulin resistance playing a role. Therefore, smoking can induce diabetes both by increasing insulin resistance and through reduction of insulin secretion. 42
Each cigarette smoked leads to an inflammatory response in the body and if continued, chronic pancreatitis. Prolonged smoking destroys the exocrine part of the pancreas (the pancreas decreases morphologically), while the pancreatic islets become restricted and then destroyed.14,16,17,43 The studies conducted by Sarles et al. 44 showed that smokers are more predisposed to pancreatic calcification than non-smokers. This fact was also confirmed by Cavallini et al, who showed that for smoking patients with chronic pancreatitis, there was a 20% increased risk of pancreatic calcifications when compared to non-smoking patients. Furthermore, it was observed that pancreatic calcifications are formed earlier in smokers than in non-smokers (median: 4.5 years earlier). 45
Studies evaluating the pancreatic exocrine function in smoking patients with chronic pancreatitis showed a significant impairment in the activity of the pancreatic enzymes.46–50 For many years, it was thought that both parts of the pancreas – the endocrine and the exocrine – operated independently and had different functions in the body. Recent studies suggest that there is an interaction between the endo- and exocrine function of the pancreas. For example, insulin affects the synthesis and the secretion of enzymes by the exocrine pancreas in the acini receptor mechanism. 51 Immunohistochemical localization of insulin and glucagon in pancreatic samples differs in smokers and non-smokers with chronic pancreatitis,17,43 with reduced insulin detection in the former group, particularly in the tail of the pancreas.
The significantly lower levels of insulin and the higher blood glucose levels in smokers with chronic pancreatitis in comparison to non-smokers coincided with the progression of changes in the structure and dysfunction of the endocrine organ 17 (Figure 3).
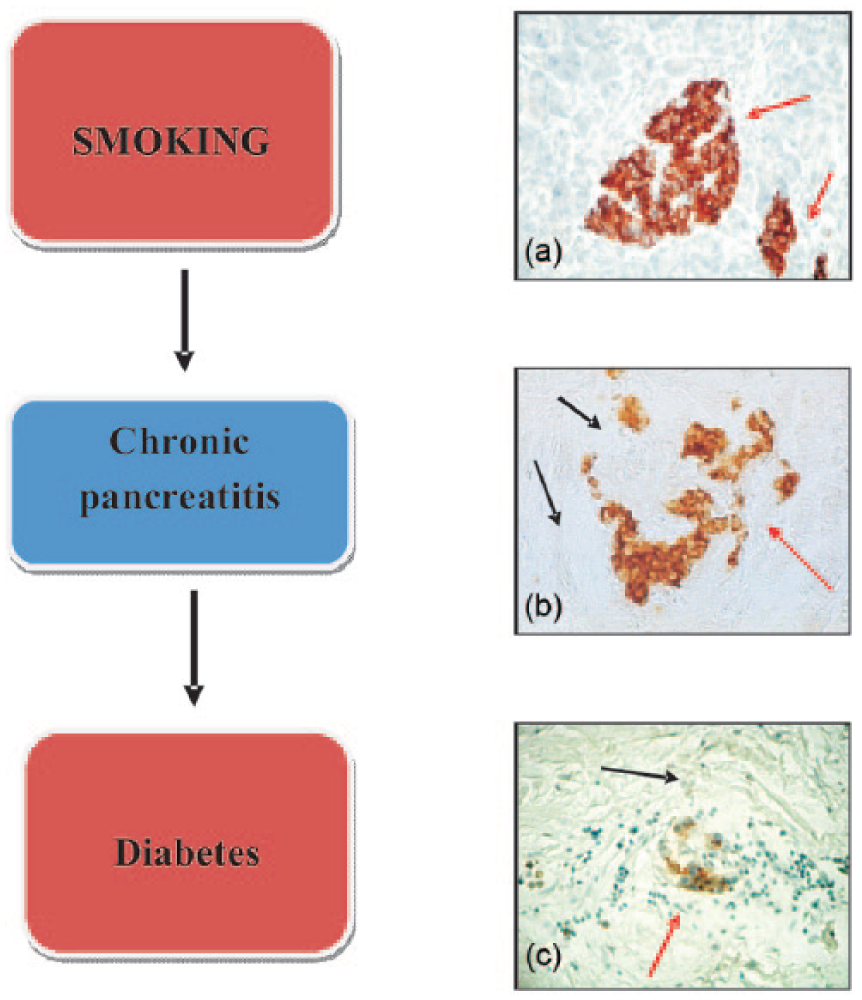
The relationship between smoking, chronic pancreatitis and diabetes. Immunohistochemical localization of insulin in pancreas. (a) Normal pancreas. The islet was predominantly composed of well-granulated β cells heavily stained for insulin. (b) Smoking patient without diabetes suffering from chronic pancreatitis: moderate, diffuse expression of the hormone in cells located in the damaged islet; many fibroses inside the islet. (c) Smoking diabetic patient with chronic pancreatitis: Weak immunohistochemical reaction for insulin in β cells in a damaged islet. Around the islet, inflammatory infiltration and advanced stage fibrosis of the pancreas are visible (photography from own study; 210×; arrows: red: pancreatic islets; black: fibrous lesions in the sub-layer).
Chemical components of tobacco smoke may have direct toxic effects on the pancreas and β-cell function, both in foetal life and adulthood. Because higher levels of inflammatory markers [C-reactive protein and interleukin-6 (IL-6)] herald the development of diabetes, 52 smoking may also contribute to the development of diabetes by increasing levels of inflammatory markers. 16 Furthermore, mitochondrial dysfunction, oxidative stress and inflammation are involved as underlying mechanisms for the direct toxicity induced by nicotine via nAChRs.
Increased insulin resistance
In healthy people, glucose levels are maintained within the normal range through proper insulin secretion by β cells and the sensitivity of peripheral tissues to the action of this hormone.53,54 Insulin resistance, metabolic syndrome and glucose intolerance are regarded as disturbances with a common background and strong interrelations. 55 Increasing insulin resistance seems to be the primary factor especially in the pathogenesis of type 2 diabetes, which occurs many years before the appearance of overt hyperglycaemia. In the early stages of increased insulin resistance, the islet β cells ‘try’ to compensate increasing secretion of insulin. 54 Current evidence indicates that smoking increases insulin resistance, although exact mechanisms remain to be elucidated (Table 2; Figure 4).
Pathophysiological changes associated with smoking having an impact on insulin resistance.
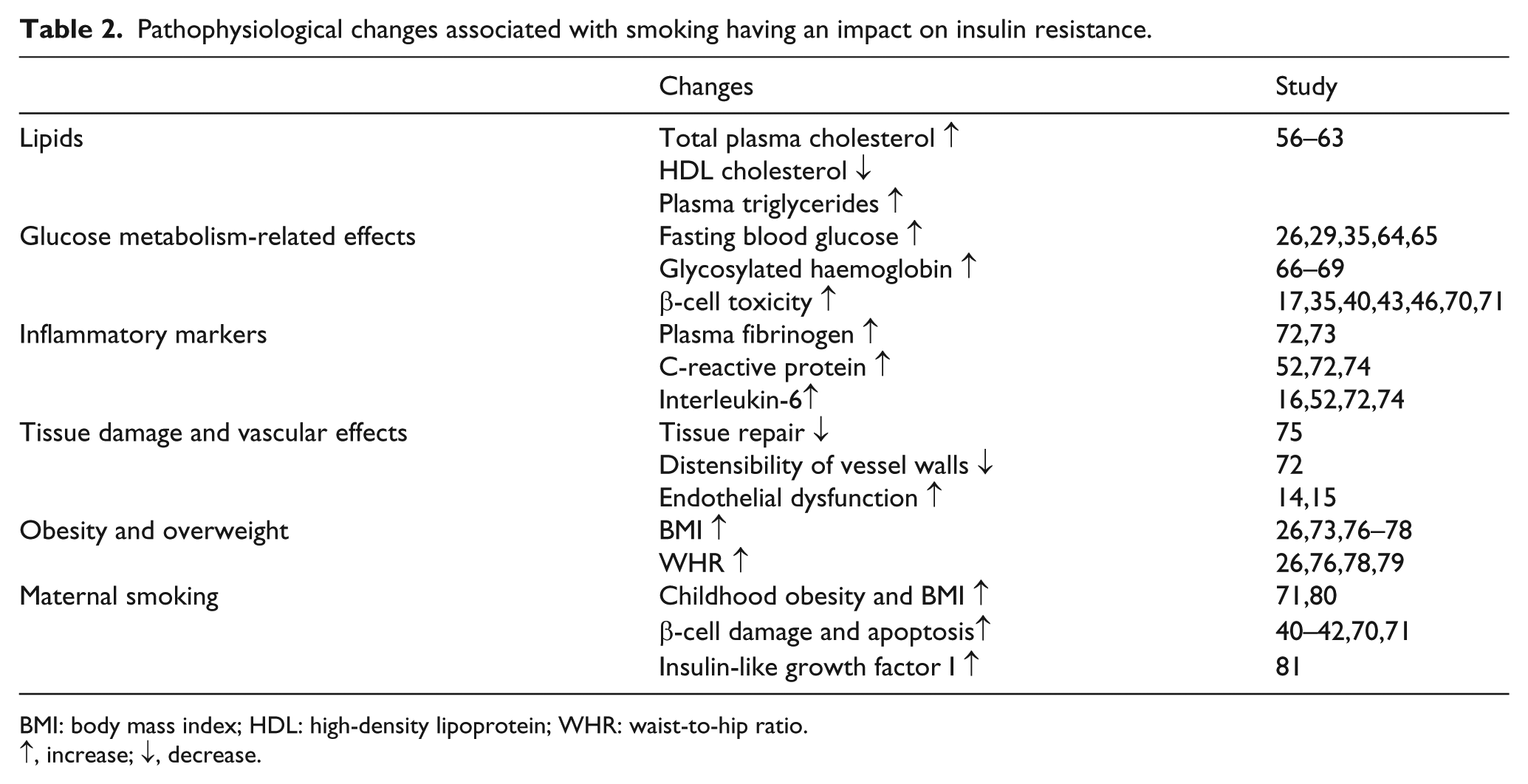
BMI: body mass index; HDL: high-density lipoprotein; WHR: waist-to-hip ratio.
↑, increase; ↓, decrease.
Numerous studies have shown the negative effects of cigarette smoking on peripheral insulin action,53,59 which appears to be ‘dose dependent’. 58 In healthy young men, acute smoking showed an increased insulin resistance. 86 Smokers had a significantly increased homeostatic model assessment insulin resistance index an hour after smoking. 87 The smoking reduced insulin-mediated glucose uptake by 10%–40% in men who smoked compared with non-smoking men.58,59 Additionally, in healthy men, chronic smoking was associated with high plasma insulin concentrations, independent of other factors known to influence insulin sensitivity. This observed increase in insulin resistance in smokers may be related, at least in part, to nicotine as long-term use of nicotine gum use is associated with hyperinsulinaemia and insulin resistance. 82
The chronic smoking effect on insulin sensitivity was also evaluated in patients with type 2 diabetes, and the results of this study showed decreased peripheral glucose metabolism in smoking patients when compared to non-smokers. Insulin and C-peptide responses to oral doses of glucose were significantly higher in smokers than non-smoking patients, while the blood glucose was not significantly different. Thus, chronic cigarette smoking seems to increase significantly insulin resistance in type 2 diabetes, 85 which may have implications for treating these patients. Human experiments using the glucose-clamp technique have found that an acute infusion of nicotine aggravates the insulin resistance response in people with type 2 diabetes, 83 further implicating this agent in the observed changes in insulin sensitivity in smokers.
On the positive side, the effect of smoking on insulin sensitivity may be partially reduced after quitting smoking. 84 In non-obese men, insulin sensitivity improved 8 weeks after smoking cessation, despite an increase in body weight. 59
Cigarette smoking also creates an unfavourable lipid profile by increasing plasma concentrations of triglycerides coupled with a decrease in high-density lipoprotein (HDL), secondary to hyperinsulinemia and insulin resistance. 57
Many epidemiological studies have shown that smoking is independently associated with an increased risk of central obesity. 13 Central obesity is a well-established risk factor for insulin resistance and diabetes. The accumulation of visceral adipose tissue is influenced by the concentration of cortisol, and smokers tend to have higher concentrations of fasting plasma cortisol than non-smokers, which might be a consequence of the stimulation of activity in the sympathetic nervous system induced by smoking. 88
Prenatal nicotine exposure increases the expression of genes of transcription factors responsible for the deposition of fat, such as CCAAT/enhancer-binding protein α (C/EBPα), peroxisome proliferator activated receptor γ (PPARγ) and sterol regulatory element-binding proteins (SREBP). Early changes in the tissue lead to the development of significant metabolic changes in adulthood, manifested in an increase in the body weight, changes in body fat distribution and impaired carbohydrate metabolism, including insulin sensitivity. The results of these studies indicate a direct link between the prenatal exposure to nicotine metabolic syndrome and the emergence of developmental disorders of fat tissue and pancreatic cancer. 71 A relationship between the intensity of smoking and the risk of obesity has been shown, which is probably related to unhealthy lifestyle resulting in increased waist-to-hip ratio. 76
Others have shown that smoking is associated with worsening visceral adiposity independently of changes in BMI, 73 which helps explain the paradox of increased metabolic risk associated with visceral adiposity, despite overall weight loss. However, the incidence of metabolic syndrome may not be increased if weight loss is associated with a net loss of central adiposity. 89
The differential effects of tobacco smoking on sex hormones may help to explain the positive association between smoking and the accumulation of fat around the midsection. Smoking has independent effects on sex hormones (oestrogens and androgens in women, testosterone in men). 90 These effects may promote the accumulation of abdominal fat, especially in men. With smoking cessation, the risk of diabetes decreases over time, 33 but it may also paradoxically increased in association with the weight gain that occurs during the first 3–5 years following smoking cessation. 91 Mechanisms for smoking-induced insulin resistance are listed in Figure 5.
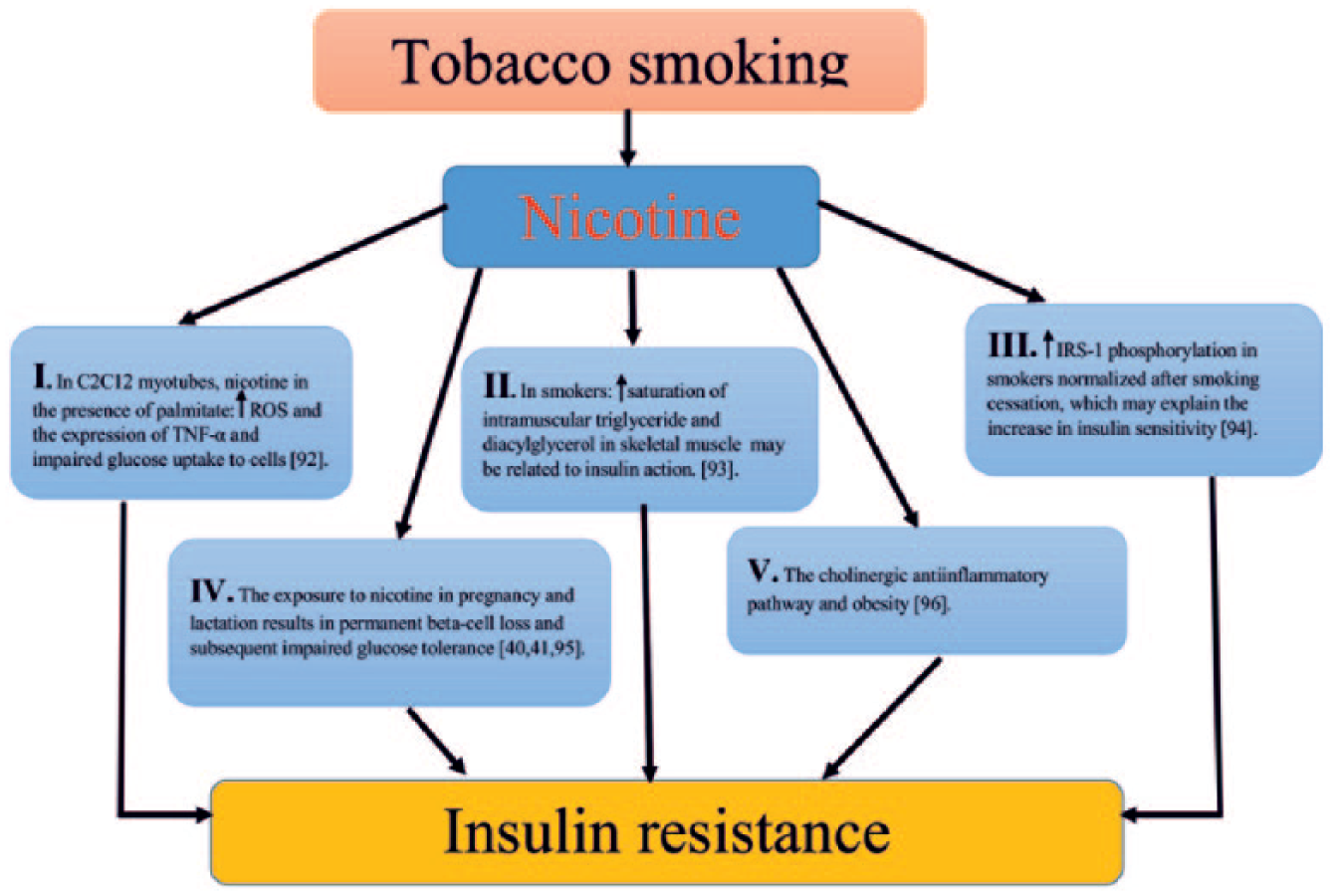
Potential mechanisms of nicotine-induced insulin resistance (↑ – increase).
Taken together, smoking increases blood glucose in patients with diabetes but it can also precipitate hypoglycaemia. The relationship between smoking and severe hypoglycaemia may be due to an effect of smoking on insulin clearance. However, smoking has been shown to increase the secretion of hormones (i.e. growth hormone, arginine vasopressin and cortisol) that counteract insulin action, leading to an increased insulin requirement. Smokers have been found to require more insulin than non-smokers to achieve the same level of glycaemic control. 95
Smoking and diabetes complications
For patients with diabetes, smoking is associated with an increased risk of cardiovascular events and death. A meta-analysis of prospective studies on diabetes reported that smoking increased the risk of death by 48%, coronary heart disease (CHD) by 54%, stroke by 44% and myocardial infarction by 52%. 5 The risk for CHD, stroke and proteinuria is directly related to the number of cigarettes smoked per day.2–4
It was found that cessation smoking by patients with diabetes reduces the risk of death and cardiovascular events compared with those who continue to smoke. 5 Additionally, smoking cessation generally decreases vascular risk for newly diagnosed diabetes mellitus. 96
Microvascular complications
Smoking is also associated with the premature development of microvascular complications: neuropathy, nephropathy and retinopathy. Interestingly, the adverse effect of smoking on renal disease may be independent of the glycaemic effect. Even 30 years ago, there was a significantly higher incidence of diabetic kidney disease in smokers than non-smokers with diabetes. 97 Smokers in diabetes are more likely to develop micro-or macroalbuminuria and low glomerular filtration rate (GFR) when compared with non-smoking patients. 98 The last study shows a clear dose–response effect of cigarette smoking on development of proteinuria in male type 2 diabetic patients. Compared with non-smokers, those who had smoked 15–30 or more than 30 pack-years were, respectively, 2.78 (95% CI: 1.34–5.76) and 3.20 (95% CI: 1.74–5.86) times more likely to develop proteinuria. The dose–response effect of tobacco exposure on the development of proteinuria was highly significant in all subjects and in subgroups with relatively short duration of diabetes mellitus, good blood pressure control and those of young age. 3 Progression of microalbuminuria to overt proteinuria and subsequent terminal renal failure are higher in case of smokers. Similar to type 2 diabetes, patients with type 1 diabetes were more likely to develop nephropathy if they were smokers.67,99 In addition, studies indicate that the relationship between cigarette smoking and renal injury is usually more pronounced in patients with type 1 diabetes, although the progress of chronic kidney disease is faster in smokers with both type 1 and type 2.
The mechanism of how smoking impairs the renal excretory function is not fully understood. It is assumed that the components of tobacco are likely to have a negative impact on the structure and the function of the glomerulus. 100 Recent studies have shown that heavy metals such as lead and cadmium accumulate in the blood while smoking may cause damage to the glomeruli. 101 In one study, the histopathological kidney tissue taken during a biopsy of smoking patients showed that there was a progressive thickening of the basement membrane associated with mesangial expansion and renal arteriolar hyalinization. 102
The general detrimental effects of smoking on the vasculature are in large part due to the induction of endothelial dysfunction. 23 Substances present in the tobacco smoke are associated with free radical processes, which undoubtedly lead to endothelial dysfunction characterized by decreased production or availability of nitric oxide associated with overproduction of endothelin-1 (ET-1).14,15,103 The imbalance between nitric oxide and endothelin, induced by smoking, increases vascular inflammation, which in turn predisposes to atherosclerosis. 104
The role of genetic predisposition in the inflammatory response in smokers is not entirely clear. However, based on recent studies, it has been shown that elevated levels of IL-6 in the blood can be a predictor of type 2 diabetes. In addition, a few studies indicate a significant association of the IL-6 C-174G single-nucleotide-598G polymorphism with type 2 diabetes. 105
Damage to organs in patients with diabetes has been linked to lipid peroxidation of cellular structures due to increased free radical activity. Plasma levels of malondialdehyde, a product of lipid peroxidation, have been shown to be higher in type 1 diabetes patients who smoked than patients with type 1 diabetes who did not. 106 In another study, it was found in the blood of smokers compared to non-smokers increase in the F2-isoprostanes level, which is associated with renal damage. 107
The association of smoking and diabetic retinopathy has not been clear. It was reported that retinopathy has been associated with glycaemic control and not smoking state 108 and therefore, the relationship between smoking and retinopathy may be purely glycaemia related.
However, some studies show the negative association between glycaemia and smoking. The data from the United Kingdom Prospective Diabetes Study (UKPDS) show that incidence of retinopathy was strongly associated with glycaemia, blood pressure and inversely with smoking. 109
Smoking may affect diabetic neuropathy differently according to the type of diabetes. 8 In type 2 diabetic patients, smoking was not a risk factor in the presence of polyneuropathy or sensory neuropathy as diagnosed by symptom and sign.8,9
By contrast, in a case-control study, it was found that in patient with type 1, but not with type 2, current or ex-smokers were significantly more likely to have neuropathy than individuals who had never smoked, and the prevalence of neuropathy increased with increasing number of pack-years smoked. After adjustment for covariates, smoking patients with type 1 for more than 30 pack-years are 3.32 times more likely to neuropathy (CI: 1.15–9.58). 8
Macrovascular disease
The development of CVD and CHD are a major complication in type 2 diabetes, as well as clinical CVD may also precede the development of diabetes.10,11 Therefore, there is a hypothesis that the CVD and the risk of type 2 diabetes is linked with the existence of the same factors, one of which is cigarette smoking. The RR of death and myocardial infarction is increased by twofold in smokers with diabetes compared with patients who do not smoke and stopping smoking significantly reduces the risk.110–112 In the London cohort of the prospective (8-year follow-up) World Health Organization Multi-national Study of Vascular Disease in Diabetics, it was shown that smoking is significantly associated with an increased risk of CHD, but not for stroke, in both type 1 and type 2 diabetic patients. 113 Other studies have shown that smoking does increase the risk for CHD in type 2 diabetic patients. In the Nurses’ Health Study, in women with type 2 diabetes, it was demonstrated that cigarette smoking was associated in a dose-dependent manner with an increased mortality and CHD. Compared with never-smokers, the RR for CHD was 1.66 (95% CI: 1.10–2.52) for current smokers of 1–14 cigarette per day and 2.68 (95% CI: 2.07–3.48) for current smokers of 15 or more cigarettes per day. 114
A recent systematic review and meta-analysis of prospective cohort studies assessed the relationship between active smoking and risk of mortality and cardiovascular events among patients with diabetes. A total of 89 cohort studies were included and RR was 1.55 (1.46–1.64) for total mortality and 1.49 (1.29–1.71) for cardiovascular mortality, while RR was 1.44 (1.34–1.54) for total CVD, 1.51 (1.41–1.62) for CHD, 1.54 (1.41–1.69) for stroke, 2.15 (1.62–2.85) for peripheral arterial disease and 1.43 (1.19–1.72) for heart failure. 115 Moreover, cigarette smoking was associated with a general increase in mortality and macrovascular complications younger patients (18–28 years) with type 1 diabetes. Interestingly, smokers with type 1 diabetes were hospitalized three times more likely than non-smokers, after adjusting for age and sex [odds ratio (OR): 3.13; 95% CI: 1.48–6.61]. 116
Other studies have also confirmed that smoking increases the risk of stroke in patients with diabetes.112,117 In the General Practice Research Database study, smoking conferred an additional risk for stroke in patients with type 2 diabetes. 118 A 4-year prospective study also showed that smoking was an independent predictor of stroke among the type 2 diabetes patients without a history of a previous event. 119
Summary
Clinical and experimental studies describe a strong relationship between active smoking and the pathogenesis of diabetes as well as the development of micro- and macrovascular complications. Smoking results in changes in insulin secretion by the β cell of the pancreas and can also mediate insulin resistance, resulting in impaired glucose metabolism that can lead to diabetes. Moreover, smoking-induced endothelial dysfunction has a key role in the development of vascular complications in this condition.
Despite the persuasive facts on the harmful effects of smoking in diabetes, it is unclear why patients with diabetes continue to smoke with at least the same frequency as the general population. This may be related to a general unhealthy lifestyle or may simply reflect the lack of an effective patient education programme in this group. Quitting smoking gradually reduces the risk of developing diabetes or vascular complications in those with established disease. Therefore, more emphasis should be placed on stopping smoking in the high-risk group of patients with diabetes, although the most effective smoking cessation strategy is yet to be determined.
Key messages
Cigarette smoking as a risk factor for type 2 diabetes
Smoking and insulin resistance
Smoking, chronic pancreatitis and diabetes
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.