
Abstract
Background:
The effects of sodium–glucose co-transporter type 2 inhibitors on home blood pressure were examined in type 2 diabetes with nephropathy.
Methods:
The patients with diabetic nephropathy were screened from medical records in our hospitals. Among them, 52 patients who measured home blood pressure and started to take sodium–glucose co-transporter type 2 inhibitors were selected. Clinical parameters including estimated glomerular filtration rate, albuminuria and home blood pressure for 6 months were analysed.
Results:
Sodium–glucose co-transporter type 2 inhibitors (luseogliflozin 5 mg/day or canagliflozin 100 mg/day) reduced body weight, HbA1c, albuminuria, estimated glomerular filtration rate and office blood pressure. Although sodium–glucose co-transporter type 2 inhibitors did not alter morning blood pressure, it reduced evening systolic blood pressure. Regression analyses revealed that decreases in evening blood pressure predicted decrements in albuminuria.
Conclusion:
The present data suggest that sodium–glucose co-transporter type 2 inhibitors suppress sodium overload during daytime to reduce evening blood pressure and albuminuria.
Introduction
Blood pressure exhibits circadian rhythm; however, this pattern is disrupted in diabetes.1,2 We showed that morning and evening blood pressures were similar in diabetic nephropathy. 2 Non-dippers suffer from high cardiovascular risk. 1 Beneficial actions of sodium–glucose co-transporter type 2 (SGLT2) inhibitors on cardiovascular outcomes in type 2 diabetes were recently demonstrated. 3 Home blood pressure measurements have higher reproducibility over ambulatory blood pressure monitoring (ABPM). Home blood pressure is therefore a superior predictor of cardiovascular prognosis and the preferred method when evaluating the effects of drugs on blood pressure. 4 However, the effects of SGLT2 inhibitors on home blood pressure have not been assessed yet. Thus, we examined the effects of SGLT2 inhibitors on home blood pressure in type 2 diabetes with nephropathy.
Methods
Patients with diabetic nephropathy were screened using medical records in our hospitals. We identified 52 patients who measured home blood pressure and started to take SGLT2 inhibitors (luseogliflozin 5 mg/day or canagliflozin 100 mg/day). We routinely recommend measuring home blood pressure for patients with hypertension and/or chronic kidney disease (CKD). Clinical parameters including estimated glomerular filtration rate (eGFR), albuminuria, and home blood pressure were analysed over 6 months. 2 We welcome the patients to take breakfast on visiting day. The study was approved by the ethical committees of International University of Health and Welfare (No. 15-S-17). The patients who changed medications other than SGLT2 inhibitors were excluded.
Before measuring home blood pressure, the patients had brought their own pressure measuring devices to the office. The attending physicians checked the device by a sphygmomanometer, and the devices showing the differences less than 5 mmHg were allowed to use. Patients were asked to measure home blood pressure twice a day: once in the morning (after void before breakfast) and the other in the evening. 1 Thus, 28 blood pressure measurements for 14 days in each period (control, 3 and 6 months after SGLT2 inhibitors) were used for comparisons.
Results
The mean age, height, duration of diabetes and low-(LDL-C) and high-density lipoprotein cholesterol were 55 ± 2 years old, 169 ± 3 cm, 10 ± 2 years, 115 ± 5 mg/dL and 47 ± 2 mg/dL, respectively. Males comprised 60% of our study sample. Metformin, dipeptidyl peptidase-4 inhibitors, α-glucosidase inhibitors, sulphonylureas and glinides were prescribed for 73%, 60%, 17%, 21% and 13% of patients, respectively. Angiotensin receptor blockers (ARBs), calcium antagonists, diuretics, β-blockers and α-blockers were taken by 55%, 46%, 15%, 32% and 19% of patients, respectively. Statin and fibrate were given for 46% and 23% of patients. In addition, enrolled patients were classified as having either stage 1 CKD (n = 2), stage 2 CKD (n = 26) or stage 3 CKD (n = 24). SGLT2 inhibitors for 3 months reduced body weight, HbA1c [Figure 1(a)] without significant changes in casual plasma glucose (185 ± 85 to 172 ± 68 mg/dL). About two-thirds of patients ate breakfast on visiting day. Albuminuria and eGFR were also reduced by after treatment with SGLT2 inhibitors for 3 months [Figure 1(b)]. After 3 months, 16 patients became normoalbuminuric out of 33 microalbuminuric, and 8 patients became microalbuminuric from 19 macroalbuminuric. In addition, SGLT2 inhibitors decreased office systolic blood pressure [Figure 1(c)] and home evening systolic blood pressure [Figure 1(d)] after 3 months without significant changes in morning systolic blood pressure [Figure 1(e)]. SGLT2 inhibitors did not significantly alter diastolic blood pressures. These trends continued until 6 months. No serious adverse reactions such as acute renal failure or urinary infection were reported.
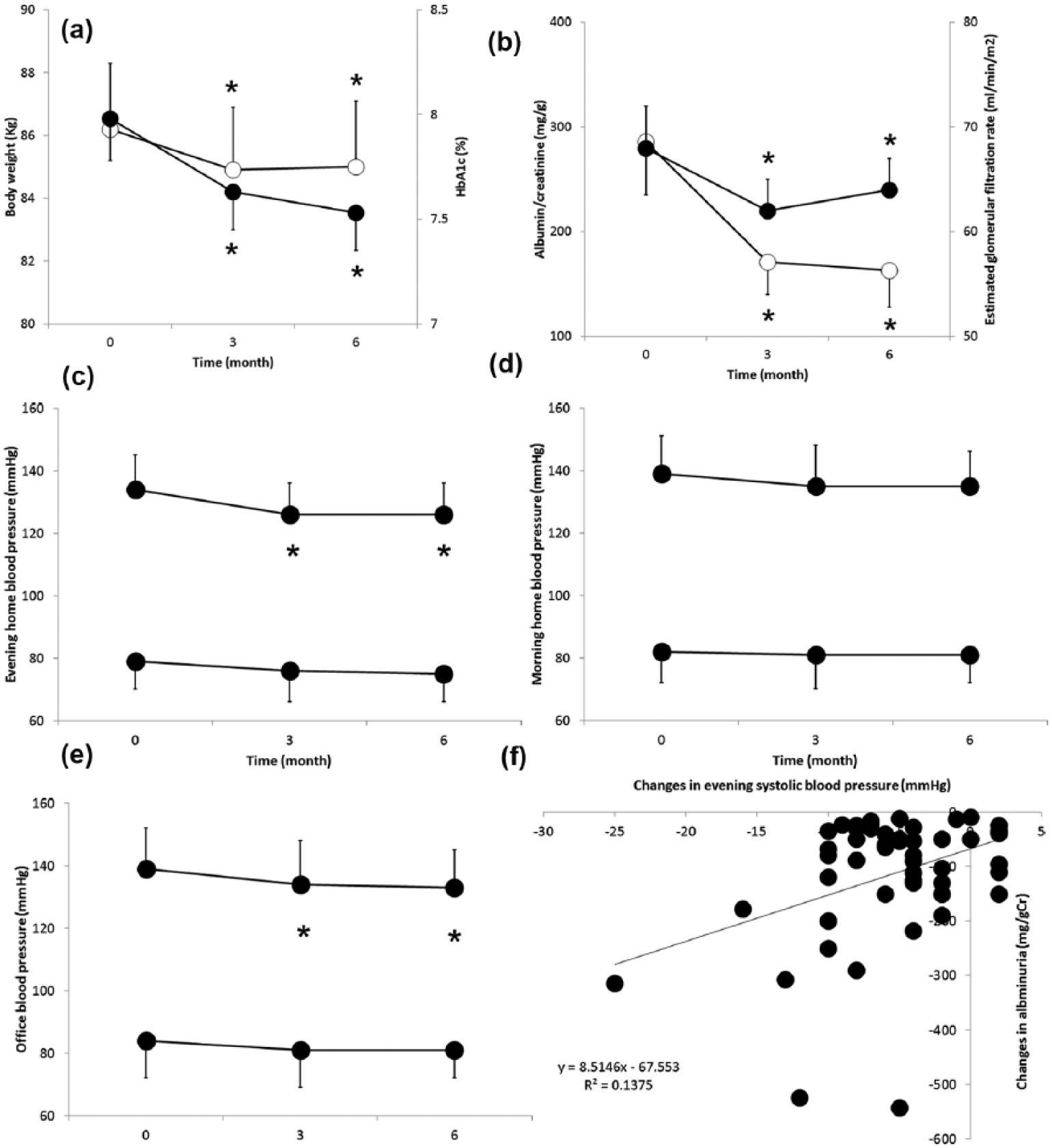
The effects of SGLT2 inhibitors on body weight (open circles, a), HbA1c (closed circles, a), albuminuria (open circles, b), estimated glomerular filtration rate (eGFR, closed circles b), office blood pressure (c), morning home blood pressure (d) and evening home blood pressure (e). *A significant change from the respective value at time 0. The relationship between the changes in evening home systolic blood pressure at 3 months and changes in albuminuria at 6 months (f). Simple regression indicates a linear relationship between the two parameters.
Multivariate regression analysis regarding patient backgrounds and albuminuria was significant (R2 = 0.91, p < 0.0001) and revealed that reductions in albuminuria at 6 months were independently correlated to age (p < 0.05), LDL-C (p < 0.01) and ARB usage (p < 0.05). A second multivariate regression model that assessed relationship between the changes in clinical parameters at 3 months and reductions in albuminuria at 6 months was significant (R2 = 0.97, p < 0.0001). We found that the reductions in evening home blood pressure (p < 0.05) and albuminuria at 3 months (p < 0.001) were the strongest predictors of the decrease in albuminuria at 6 months [Figure 1(f)]. However, the third multivariate regression analysis failed to show significant correlations between the changes in clinical parameters at 6 months and the reductions in albuminuria at 6 months.
Discussion
Tubuloglomerular feedback (TGF) is required to maintain glomerular capillary pressure and filtration rate during blood pressure variations. 5 In response to increases in distal delivery of sodium chloride following blood pressure elevations, TGF constricts afferent arterioles to impede direct transduction of systemic pressure to glomeruli. The tubular hypothesis was first proposed to account for abnormal renal haemodynamics in type 1 diabetes. 6
In diabetes, the glomerular ultrafiltrate possesses more glucose, and this is reabsorbed with corresponding amounts of sodium through SGLT, enhancing proximal tubular reabsorption. Thus, both distal delivery of sodium and TGF are diminished in diabetes, attenuating autoregulatory afferent arteriolar resistance with resultant glomerular hypertension and hyperfiltration.
SGLT2 inhibitors reduce albuminuria and improve renal outcomes in diabetic nephropathy. 7 In addition, the anti-albuminuric effect of empagliflozin was largely independent of the known metabolic and systemic haemodynamic effects of this drug class. 8 Our previous data indicate that hyperglycaemia enhances proximal sodium reabsorption via SGLT2 to diminish distal delivery and TGF in type 2 diabetes,9,10 thereby inducing glomerular hypertension and hyperfiltration. The present observations that the decrement in albuminuria was not related to those of blood pressure or HbA1c when measured on the same visiting day support the direct renal haemodynamic effects of SGLT2 inhibitors that recover TGF, constricting afferent arterioles to reduce albuminuria and eGFR. Thus, SGLT2 inhibitors may have additional simultaneous benefits beyond lowering blood pressure and promoting euglycaemia at the level of the kidney. Together, the present results are consistent with the tubular hypothesis6,9,10 and suggest that SGLT2 inhibitors normalize renal sodium handling to get tubular control of TGF back from diabetes, thereby ameliorating albuminuria.
Our study is the first to demonstrate that SGLT2 inhibitors effectively reduce evening home blood pressure, as well as body weight, in diabetes. Our findings support the idea that volume retention due to sodium reabsorption through SGLT2 during the day contributes to the maintenance of evening blood pressure in diabetes. A study using ABPM showed that SGLT2 inhibitors preferentially reduced nocturnal blood pressure, 11 providing evidence that SGLT2 inhibitors effectively decrease postprandial blood pressure that further protects the kidney. In addition, the changes in evening blood pressure by SGLT2 inhibitors independently predicted to those of albuminuria [Figure 1(f)]. Collectively, these indicate that improvements in home blood pressure due to SGLT2 inhibitors can ameliorate albuminuria in future and suggest that SGLT2 inhibitors are the treatment of choice for diabetic non-dippers, leading to an efficient reduction in cardiovascular risk. 3
Renin release is controlled partly by TGF 9 and can be influenced by postprandial hyperglycaemia despite of sodium retention through SGLT2 in diabetes, inappropriately activating renin–angiotensin system that contributes to hypertension. SGLT2 inhibitors and/or ARBs would disrupt this vicious cycle. Indeed, combined use of ARB and SGLT2 inhibitor tended to induce the greater reduction in albuminuria. However, aged, hypercholesterolemic diabetes manifested greater decrements of albuminuria by SGLT2 inhibitors, suggesting judicious application of SGLT2 inhibitors for patients with advanced atherosclerosis to avoid acute renal failure as well as stroke. 12
The study had several limitations. Since the patients enrolled in this study were diligent in measuring home blood pressure, cautions are required to generalize the results. The study lacks in control group arm. The patients are all Japanese, being bias for patient selection. However, the present pilot study on the data from clinical practice suggests that the anti-albuminuric effects of SGLT2 inhibitors involve their direct actions on the kidney and their hypotensive influence on home blood pressure. Future prospective trials that assess the actions of SGLT2 inhibitors on blood pressure and kidney function including Lithium clearance, 10 with simultaneous applications of continuous glucose monitoring and ABPM, are warranted.
Footnotes
Acknowledgements
Some of the data in this manuscript was presented at the 39th annual scientific meeting of the Japanese Society of Hypertension in October Sendai Miyagi Japan and was published as an abstract.
Author contribution
T.T. collected data and wrote the manuscript. M.K. collected data and contributed to the discussion. M.O. and O.T. collected and analysed data. H.S. collected data, and reviewed and edited the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
Our department received research funds from Taisho-Toyama Pharmaceutical Co., Ltd, Daiichi-Sankyo Co., Ltd, Astellas Pharmaceutical Co., Ltd., Takeda Pharmaceutical Co., Ltd, Chugai Pharmaceutical Co., Ltd, Mitsubishi Tanabe Pharma Corporation and Torii Pharmaceutical Co., Ltd.