
Abstract
Aims:
To assess the effects of sodium-glucose co-transporter type 2 inhibitors on central blood pressure, an important determinant of cardiovascular events.
Methods:
Canagliflozin, Empagliflozin or Luseogliflozin was given for 102 type 2 diabetic patients with hypertension and nephropathy. Central blood pressure was evaluated by radial tonometry. Clinical parameters were followed for 6 months.
Results:
Three differing sodium-glucose co-transporter type 2 inhibitors similarly reduced brachial and central blood pressures, casual blood sugar, haemoglobin A1c, estimated glomerular filtration rate and albuminuria without significant changes in pulse rate and lipid profiles. Central systolic blood pressure was associated with the decreases in albuminuria by sodium-glucose co-transporter type 2 inhibitors.
Conclusion:
Comparable influences of various sodium-glucose co-transporter type 2 inhibitors on central blood pressure suggest class effects.
Introduction
Sodium-glucose co-transporter type 2 (SGLT2) inhibitors improve cardiovascular prognosis in type 2 diabetes.1,2 Central systolic blood pressure (SBP) rather than brachial SBP contributes to cardiovascular outcomes. 3 Although SGLT2 inhibitors reduce office brachial SBP,1,2,4,5 the effects on central SBP remain poorly examined.
Methods
Type 2 diabetic patients with nephropathy and hypertension were screened from medical records in our hospitals. We identified 102 patients who measured radial tonometry and started to take SGLT2 inhibitors (Luseogliflozin 5 mg/day in 33 cases, Empagliflozin 10 mg/day in 34 cases or Canagliflozin 100 mg/day in 35 cases). We routinely assessed central SBP with radial tonometry for patients with hypertension and/or chronic kidney disease (CKD). Clinical parameters including estimated glomerular filtration rate (eGFR), albuminuria, and central SBP were mined over 6 months.5–7 We welcome the patients to take breakfast on visiting day. This retrospective study was approved by the ethical committees of the International University of Health and Welfare (no.15-S-17). The patients who changed medications other than SGLT2 inhibitors were excluded.
To evaluate central SBP, radial tonometry was used.6,7 Brachial SBP and diastolic blood pressure (DBP) were measured using oscillometric methods (HEM-9000AI; Omron Healthcare, Kyoto Japan) in a sitting position after at least a 5-min rest. Radial tonometry was automatically performed to obtain the pulse waveform by applying multiple tonometers on the wrist and assessing second peak of SBP (SBP2) on the same occasion as BP measurement. The algorithm of HEM-9000AI calculates the second maximum of the fourth derivative of the radial waveform to determine SBP2. The calibration of the waveform was performed with brachial SBP and DBP as the peak and bottom of radial pressure waveform, respectively. Recently, Sharman et al. 8 demonstrated that SBP2, which was measured by HEM-9000AI, was almost identical to central SBP estimated by the SphygmoCor system.
The data were expressed as mean ± standard deviation (SD). Statistical analyses were performed appropriately using chi-square test with Yate correction, Student’s t-test, regression analysis and analysis of variance (ANOVA). The probability less than 5% was considered significant (IBM SPSS, Statistics version 24).
Results
The patient backgrounds are detailed in Table 1. Mean age, gender, duration of diabetes, height and body weight did not differ among patients receiving three differing SGLT2 inhibitors. Usage of metformin, dipeptidyl peptidase-4 inhibitors, α-glucosidase inhibitors, sulphonylureas and glinides was analogous among three groups (by chi-square). Antihypertensive medications including angiotensin receptor blockers (ARBs), calcium channel blockers (CCB), diuretics, β-blockers and α-blockers, as well as lipid-lowering drugs such as statins and fibrates, were similarly given for three groups.
Patient backgrounds.
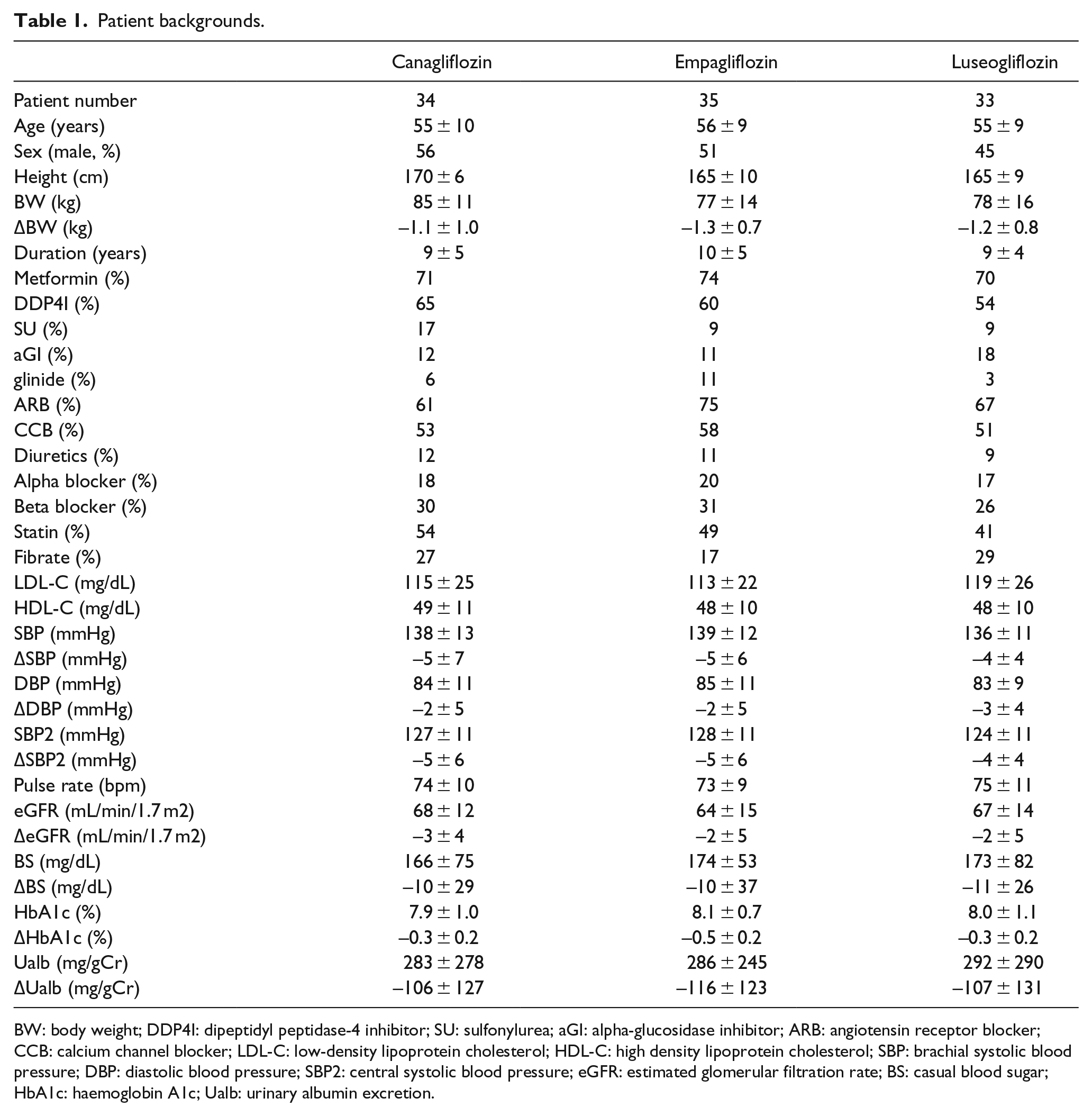
BW: body weight; DDP4I: dipeptidyl peptidase-4 inhibitor; SU: sulfonylurea; aGI: alpha-glucosidase inhibitor; ARB: angiotensin receptor blocker; CCB: calcium channel blocker; LDL-C: low-density lipoprotein cholesterol; HDL-C: high density lipoprotein cholesterol; SBP: brachial systolic blood pressure; DBP: diastolic blood pressure; SBP2: central systolic blood pressure; eGFR: estimated glomerular filtration rate; BS: casual blood sugar; HbA1c: haemoglobin A1c; Ualb: urinary albumin excretion.
At the baseline, SBP, DBP, SBP2, pulse rate, casual blood sugar, haemoglobin A1c (HbA1c), eGFR, albuminuria and low- and high-density lipoprotein cholesterol were comparable among three groups (by ANOVA). Among the above parameters, the variations of the parameters are described in Table 1 when the addition of SGLT2 inhibitors altered them in 6 months. The administration of SGLT2 inhibitors significantly reduced body weight, SBP, DBP, SBP2, casual blood sugar, HbA1c, eGFR and albuminuria without considerable changes in pulse rate and lipid profiles. However, any SGLT2 inhibitors did not alter SBP-SBP2 (Canagliflozin group: 11 ± 4 to 11 ± 4 mmHg, Empagliflozin group: 11 ± 3 to 12 ± 3 mmHg, Luseogliflozin group: 12 ± 3 to 12 ± 4 mmHg).
Since there were no significant differences among three groups, the data were combined. Multivariate regression analysis regarding patient backgrounds and albuminuria reduction was significant (R2 = 0.71, df(26,75), F = 6.7, p < 0.001), and revealed that reductions in albuminuria were independently correlated to age (p < 0.001), SBP2 (p < 0.05), the usage of ARB (p < 0.005) and metformin (p < 0.01). Second multivariate regression model that assessed relationship between the changes in clinical parameters and reductions in albuminuria at 6 months was also significant (R2 = 0.18, df(7,94), F = 2.2, p < 0.05), and the changes in eGFR correlated to those of albuminuria (p < 0.05).
Discussion
Vasodilating antihypertensive agents, including CCBs, ARBs, converting enzyme inhibitors and alpha-adrenergic blockers, which widen SBP-SBP2, preferentially reduce the central blood pressure rather than the brachial blood pressure. 6 In contrast, non-vasodilating antihypertensive medications, such as diuretics and beta-adrenergic blockers, which uphold SBP-SBP2, similarly reduce the central and brachial blood pressures. Thus, the administration of vasodilator antihypertensive agents to hypertensive patients more efficiently lowers the central blood pressure, compared to non-vasodilator antihypertensive medications, thereby ameliorating albuminuria and preventing the development of atherosclerotic cardiovascular diseases.3,7
Central SBP participates more importantly in cardiovascular events rather than brachial SBP. 3 Similar reductions in central blood pressure with the use of three different SGLT2 inhibitors suggest that this is a class effect. The greater SBP-SBP2 indicates the preferential action of the agent on central rather than peripheral blood pressure. 6 However, both SBP-SBP2 and pulse rate remained unchanged by the treatment with SGLT2 inhibitors. Thus, the actions of SGLT2 inhibitors on central haemodynamics resemble to those of diuretics, non-vasodilating antihypertensive medication. 6 Our data constitute new findings that SPB2 predicted the reductions in albuminuria by SGLT2 inhibitors. Albuminuria represents an intermediate phenotype of cardiovascular risk. 9 The reduction in albuminuria during treatment translates to the reduction in cardiovascular events. 9 SGLT2 inhibitors improve cardiovascular outcomes in type2 diabetes.1,2 Hospitalization for heart failure was one of endpoints in these studies.1,2 Central blood pressure reduction can have potential impacts in heart failure beyond just brachial blood pressure reduction. Taken together, these suggest that the reductions in central SBP by SGLT2 inhibitors are involved in the cardiovascular protection.
Hyperglycaemia enhances proximal sodium reabsorption via SGLT2 to diminish distal delivery and tubuloglomerular feedback (TGF) in type2 diabetes,10,11 thereby inducing glomerular hypertension and hyperfiltration. The present observations that the decrement in albuminuria was related to those of eGFR, but not those of either blood pressure or glycaemic parameters support the direct renal haemodynamic effects of SGLT2 inhibitors that recover TGF, constricting afferent arterioles to reduce both albuminuria and eGFR.5,11,12 Collectively, these suggest that the improvements in albuminuria can partly account for cardiovascular protection by SGLT2 inhibitors in type 2 diabetes. Thus, SGLT2 inhibitors appear to be the treatment of choice for diabetic nephropathy, leading to an efficient reduction in cardiovascular risk as well as the progression of nephropathy.1,2,4
Renin release is controlled partly by TGF 10 and can be influenced by postprandial hyperglycaemia despite of sodium retention through SGLT2 in diabetes, inappropriately activating renin–angiotensin system that contributes to hypertension. SGLT2 inhibitors and/or ARBs would disrupt this vicious cycle. Indeed, combined use of ARB and SGLT2 inhibitor tended to induce the greater reduction in albuminuria in this study. Our observations support that the combination of metformin and SGLT2 inhibitors may induce greater reductions in albuminuria, a cardiovascular risk factor. However, elderly diabetes manifested greater decrements in albuminuria by SGLT2 inhibitors, suggesting judicious application of SGLT2 inhibitors for elderly patients to avoid acute renal failure. 5
The study had several limitations. The study lacks in control arm. Thus, only relative influences of SGLT2 inhibitors were examined, and cautions are required to generalize the results. The patients are all Japanese, being relatively short and bias for patient selection. However, this pilot study on the data from clinical practice suggests that cardiovascular protective actions of SGLT2 inhibitors involve their direct actions on the kidney to reduce albuminuria and their hypotensive influence on central blood pressure. Future prospective trials that assess the actions of SGLT2 inhibitors on central blood pressure (cardiovascular risk reduction) and kidney function (albuminuria reduction) are warranted.
Footnotes
Acknowledgements
Parts of the data in this manuscript were presented at 40th annual meeting of Japanese Society of Hypertension in Matsuyama, Ehime October 2017, and was published as an abstract. T.T. wrote the manuscript and researched data. Y.O. researched data and contributed to the discussion. H.S. contributed to the discussion and reviewed/edited the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Our department received research funds from Astellas Pharma, Mochida Pharmaceutical Co., Ltd, Taisho-Toyama Pharmaceutical Co., Ltd, Daiichi-Sankyo Co., Ltd, Takeda Pharmaceutical Co., Ltd, Eli Lilly Japan K.K, Chugai Pharmaceutical Co., Ltd, Otsuka Pharmaceutical Co., Ltd, and Torii Pharmaceutical Co., Ltd.