
Abstract
We present clinical, electroencephalographic and low-resolution electromagnetic tomography data that support combined treatment with insulin and a monoamine oxidase inhibitor in a patient with type 1 diabetes. We suggest that brain imaging data can identify a subgroup of patients who are likely to benefit from an insulin regimen and monoamine oxidase inhibition to improve glycaemic control, cardiovascular function, normalize the circadian rhythm and restore perception of glycaemic awareness.
Keywords
Introduction
Treatment of type 1 diabetes (T1D) is directed towards reducing glucose levels with insulin analogues, yet hypoglycaemia is a common, often life-threatening complication. 1 The ability to perceive hypoglycaemic episodes becomes blunted after repeated bouts of hypoglycaemia by counter-regulatory responses and abnormal secretion of catecholamines and glucagon. 2 The neurobiological basis of hypoglycaemic detection and impaired hypoglycaemic awareness is complex.2,3 This study describes the clinical treatment of a T1D patient with erratic glucose levels, further complicated by his loss of hypoglycaemic perception. Electroencephalographic (EEG) features with low-resolution electromagnetic tomography (LORETA) analyses identified a neurophysiologic subtype of low brain electrical activity suggesting reduced monoamine signalling associated with irregular glucose levels and defective glucose counter-regulation.
Case report
A 21-year-old male suffered the onset of type 1 diabetes mellitus during college. He was treated with a daily dose of 32 U of Lantus and an average of 20 U of Humalog. Subsequently, there was cessation of prior protective percepts of darkened vision, diaphoresis and tremors that had warned him of a low glucose level (2.5−3.9 mmol/L). His glucose levels became increasingly labile, and he experienced onset of primary and secondary insomnia, anxiety, reduced energy and inefficiency at work.
His clinical data indicated a body mass index (BMI) of 24.6, resting state blood pressure of 130/82 mmHg and an average pulse rate of 65 beats/min. His fasting blood glucose (FBS) was 10 mmol/L and his haemoglobin-A1c (HbA1c) was 6.5%. His Quality of Life Scale (QOLS) was 78 and Patient Health Questionnaire (PHQ-9) was 5, indicative of mild depression. A baseline EEG was extracted during a normal glycaemic interval (6.7 mmol/L).
Quantitative EEG (qEEG) data showed diffusely low absolute voltages across frequencies (−1.5 to −2 Ζ-scores), increased relative voltages in the low-frequency (delta and theta) bands and decreased voltages in relative alpha frequencies across regions (Figure 1(a)). Current source densities (CSDs) in Talairach space with LORETA confirmed reduced brain electrical activity across all regions. There was significantly reduced delta activity in the subcallosal gyrus, reduced theta activity in the middle temporal gyrus, and reduced bilateral alpha1, alpha2, beta1, beta2 and beta3 activities in the middle and superior temporal gyri with asymmetrically increased beta3 activity in the brain’s visual processing centre, the lingual gyrus (Figure 1(b)).
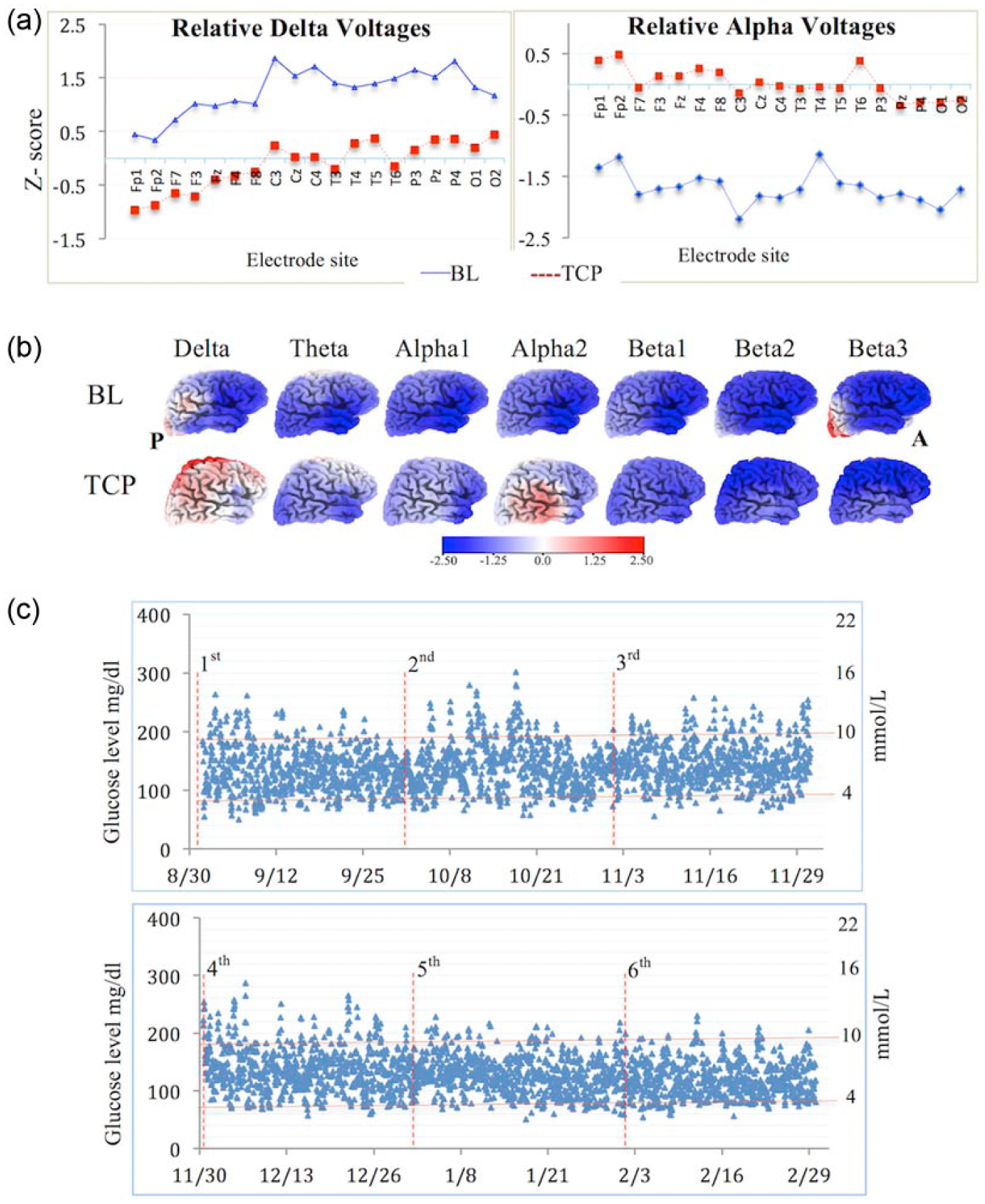
qEEG, LORETA data and glucose levels before and with tranylcypromine. (a) Graphs showing differences in qEEG relative delta and alpha at a given electrode. Z-scores indicate differences between baseline (solid blue line) and treated (dashed red line) measures. (b) Three-dimensional images showing current density in Talairach space obtained by LORETA for baseline (BL) and tranylcypromine (TCP). Differences in seven frequency bands (delta: 1 Hz, theta: 7 Hz, alpha1: 9 Hz, alpha2: 11 Hz, beta1: 16 Hz, beta2: 21 Hz and beta3: 29 Hz) are shown. Blue areas correspond to reduced brain activity and red areas to increased activity (A: anterior, P: posterior). (c) Plasma glucose levels using a continuous glucose-monitoring device during 6 months with tranylcypromine. Blue dots denote hourly glucose levels. Vertical lines represent each month of treatment and horizontal lines correspond to hypo- and hyper-glycaemic thresholds.
Low-voltage qEEG measures inferred an overall deficiency in monoamine signalling in limbic brain regions, likely contributing to the brain’s insulin resistance and impaired glycaemic control. 4 A non-selective monoamine oxidase (MAO) inhibitor that prevents breakdown of serotonin and catecholamine signalling would likely improve the patient’s intrinsic brain activity. Thus, the MAO inhibitor, tranylcypromine, was prescribed at 20 mg/day.
Two weeks following tranylcypromine treatment, the patient reported improved energy, focus and resolution of insomnia. His BMI reduced to 24.5, blood pressure decreased to 126/63 mmHg, pulse rates increased to 74 beats/min and PHQ-9 reduced to a normative score of 1 with a normative increase in QOLS to 89. After 2 months with tranylcypromine, a follow-up EEG/qEEG showed reduction of excessive slow waves (delta and theta) and normalized relative alpha voltages across brain regions (Figure 1(a)). LORETA analysis revealed asymmetric shifts in localization with most changes occurring in the right hemisphere. Delta voltages normalized in the right hemisphere and mildly increased in the left. Theta, alpha1 and alpha2 voltages normalized in the right hemisphere. Beta1 and beta2 voltages mildly improved, particularly in the right pre-central gyrus. Bilateral beta3 excess in the lingual gyri of the occipital lobe also normalized (Figure 1(b)).
The patient had been using continuous glucose monitoring (CGM) to provide a clearer picture of the magnitude and frequency of glucose measures. His blood glucose decreased over several weeks and he reduced his Lantus regimen from 32 to 28 U/day. In addition, he began inhaled insulin at an average of 30 U/day to reduce his risk of nocturnal hypoglycaemia. During the third month, he decreased his daily average insulin to 22 U of Lantus and 14 U of Humalog per day (Figure 1(c), top panel). During the fifth and sixth months from baseline, he reduced the average daily dose of Lantus to 18 U and replaced Humalog with 34 U of inhaled insulin per day maintaining plasma glucose levels between 4.0 and 10.0 mmol/L (Figure 1(c), bottom panel). More importantly, his ability to perceive the onset of hypoglycaemia was restored during the fifth month with a HbA1c at 5.4%.
Discussion
A T1D patient with a low absolute voltage qEEG showed improved glycaemic control and restored hypoglycaemic perception with MAO inhibition. This work further supports the effects of MAO inhibitors on glucose homeostasis as previously reported by Adnitt 5 and Barrett. 6 In addition, this study demonstrates that EEG/qEEG subtyping identified neurophysiologic parameters for selection of MAO inhibition.
Hypoglycaemic states have been associated with increased qEEG voltages in the lower banded frequencies (delta and theta) and reduced qEEG voltages in alpha7,8 as well as beta banded frequencies.4,8 Increased voltages in the lower frequency bands associated with hyper- or hypoglycaemia are comparable to qEEG abnormalities observed in other syndromes, including sleep, cognitive and mood dysfunctions.7,8 This suggests that similar neurobiological circuits are involved. The patient’s low-voltage EEG measures did not improve during euglycaemia, indicating that insulin alone is insufficient to fine-tune brain activity, consistent with other reports that qEEG features do not significantly change in T1D patients when rendered hypoglycaemic. 7 After several months of improved glycaemic control, the patient regained perception of low plasma glucose levels. This is consistent with evidence that reduced hypoglycaemic episodes are associated with a better neurophysiologic epinephrine response.
MAO isoforms have emerged as major sources of oxidative stress in cardiovascular dysfunction. 9 The non-selective MAO inhibition in this patient reduced systolic and diastolic blood pressures (−4/−19) and increased the average pulse rates from 65 to 74 beats/min. Patients with cardiovascular disorders are often empirically treated with beta blockers that reduce brain electrical activity. MAO inhibitors can offer a therapeutic alternative to a subtype of patients with low-voltage qEEG measures.
This study describes a clinical approach to improve cardiovascular function and achieve glycaemic control by using EEG/qEEG and LORETA data. We suggest that neurophysiologic subtyping can improve brain activity, cardiovascular function and insulin sensitivity in a subgroup of patients with diabetes.
Footnotes
Acknowledgements
The authors are grateful to Dr Meyer Proler and Matthew Kwasman for their expertise.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.