
Abstract
Objective:
To study the clinical characteristics related to metabolic disorders and complications in type 2 diabetes mellitus patients hospitalized in the Qingdao Endocrine and Diabetes Hospital from 2006 to 2012 in Qingdao, China.
Patient population and methods:
Data from 14,289 (51% males) type 2 diabetes mellitus patients hospitalized between 2006 and 2012 were collected and analysed. Information on patients’ demographic, anthropometric, laboratory and disease histories were extracted from electronic medical records.
Results:
The mean age of the patients was 60.5 years, with median diabetes duration of 9.0 years. Mean haemoglobin A1c was 8.4%, where <30.0% of patients had haemoglobin A1c <7.0%. In all, 34.5% of patients had low-density lipoprotein cholesterol lower than 2.6 mmol/L and 31.9% had hypertriglyceridaemia. Retinopathy was diagnosed in 51.1% of patients, nephropathy in 21.6%, neuropathy in 50.4%, hypertension in 77.4%, coronary heart disease in 27.6% and peripheral vascular disease in 58.6%. Once hospitalized, 71.1% of patients underwent insulin injection treatments, either mono-therapy or combined with other anti-diabetic drugs. Metformin was prescribed to 36.9% of patients, followed by acarbose 29.9%, thiazolidinediones 18.1%, meglitinides 14.8% and sulfonylureas 10.7%.
Conclusion:
Inadequate control of hyperglycaemia, poor metabolic profiles and diabetic complications were common challenges for long-term diabetes management in Chinese patients with type 2 diabetes mellitus.
Keywords
Introduction
Diabetes care casts an enormous challenge to the public health of China.1,2 Besides a rapid increase in prevalent cases,3–5 a number of studies have reported that diabetes management is inadequate in China. Approximately 57% of patients with diagnosed diabetes have been reported to be inadequately treated, and 79% have poor glucose control. 6 Previous research among Chinese subjects has shown high blood pressure levels above the recommended target goal [systolic blood pressure (SBP) <130 mmHg and diastolic blood pressure (DBP) <80 mmHg] in 72% of the patients and 57% had low-density lipoprotein cholesterol (LDL-c) higher than 2.6 mmol/L. 7 It is expected that due to poor diabetes management in China, an increasing number of subjects with type 2 diabetes mellitus (T2DM) will develop diabetic complications of epidemic proportions. In 2002, it was reported that 73.2% of hospitalized diabetes patients had at least one diabetic micro- or macro-vascular complication. 8 In a study recently published, neuropathy, retinopathy and nephropathy were detected in 29%, 25% and 16% of all patients, respectively. 9
Most of these previous studies were based on patient registry data or health surveys, which were performed in a research setting. Few studies, as far as we know, were performed in a real-world clinical practice setting. We performed our current study with data collected from hospital-acquired electronic medical records (EMRs) in order to understand the disease characteristics of Chinese patients with T2DM and to review current treatment patterns in a real-world clinical practice.
Methodology
All the EMRs were acquired from the Qingdao Endocrine and Diabetes Hospital (the Hospital), a public non-profit tertiary hospital. The Hospital was established in 2002 and is located in the downtown area of Qingdao city, one of the biggest cities along the east coast of China. The Hospital is the only one specializing in the treatment of diabetes not only in Qingdao but throughout the region with a catchment area of approximately 100 km, which covers 7.2 million people. The majority of these patients were Han Chinese residing in Qingdao city and the surrounding regions. Less than 1% of patients were national ethnic minorities or of foreign origin. In general, doctors hospitalized patients when the patients were suspected to have experienced acute diabetic complications (ketosis, ketoacidosis, diabetic hyperosmolality, etc.), uncontrolled hyperglycaemia for a certain period and at least one chronic complication, or significantly worsening of chronic complication (rental haemorrhage, significant elevated albuminuria and/or serum creatinine, acute myocardial infarction, etc.).
EMRs have been applied in the hospital to document the course of treatment for all patients since 2005. By the end of November 2012, a total of 24 815 patients had been admitted for the first time into the inpatient department of the Hospital, accounting for the same number of EMRs. The patients hospitalized in 2005 (n = 1956), as part of an assessment pilot for the EMR system at the Hospital, were excluded from the current analyses. Among the 22,859 patients hospitalized from January 2006 to November 2012, 19,759 patients were diagnosed with T2DM. Excluding 73 patients who were younger than 20 years and not Han Chinese, we further dropped 5397 patients (accounting for 27.4%) from this study due to a large portion of missing data for key variables such as haemoglobin A1c (HbA1c), plasma lipids, blood pressure and urinary albumin excretion rate (UAER). The final population selected for this study consisted of 14,289 patients (7240 males). This study was approved by the ethics committee of Qingdao Endocrine and Diabetes Hospital.
All data were collected by reviewing the EMRs which recorded the first admission of a patient to Qingdao Endocrine and Diabetes Hospital. Data of repeated admission were all excluded from the current analyses. Demographic information included the date of birth, date of hospitalization and discharge, sex, education level, occupation, medical insurance and marital status. History of previous medical conditions and events, anthropometric measurements (weight, height, waist and hip circumference), blood pressure and heart rate were extracted from corresponding parts of the EMRs. The results of 62 laboratory tests were collected, including plasma glucose (fasting or postprandial), HbA1c, serum insulin (fasting or post-challenged), serum C-peptide (fasting or post-challenged), fasting plasma lipids, plasma liver enzymes, fasting plasma uric acid and UAER, among others. Detailed information from electrocardiogram (ECG), echocardiography, ultrasound imaging of the liver, kidney and large arteries, funduscopy and fundus fluorescence were extracted and processed using standardized protocols. Information on the drugs administered after patients were admitted to the Hospital was also collected.
HbA1c was measured with high-performance liquid chromatography (Arkray, ADAMS tm A1c HA8180). Fasting plasma lipids were determined using the enzyme method (Beijing Leadman Biochemistry Co., Ltd, Leadman, Hitachi 7080). When the levels of fasting and post-meal glucose were well controlled, fasting serum C-peptide was measured with chemiluminescence immunoassay (Siemens, Siemens Immulite 1000). The 24-h UAER was measured with chemiluminescence immunoassay (Siemens, Siemens Immulite 1000) from 24-h urine samples. All laboratory tests were regularly audited by the Qingdao Quality and Technology Supervision Bureau, which is a local governmental authority.
Diabetes, diabetic complications and comorbidities were diagnosed by physicians of the Hospital according to Chinese guidelines for diabetes management. 10 Diabetes mellitus was diagnosed when at least one of the following conditions were met: (1) repeated fasting plasma glucose levels were equal or higher than 7.0 mmol/L, (2) post-challenged glucose levels were equal or higher than 11.1 mmol/L, (3) HbA1c was equal or higher than 6.3% and/or (4) had a prior history of diabetes and was taking anti-diabetic medicines. A standardized oral 75 g glucose tolerance test might be performed when the diagnosis of diabetes was not definitive. If type 1 diabetes was suspected, C-peptide, auto-antibodies and clinical characteristics were reviewed to classify the type of the disease. Diabetic nephropathy (DKD) was defined by a condition where UAER is equal to or higher than 30 mg/24 h, and/or if DKD was previously diagnosed.11,12 Diabetic retinopathy (DR) was diagnosed by an ophthalmologist based on funduscopy and/or fundus fluorescence findings. 13 Diabetic neuropathy (DN) was diagnosed by physicians according to clinical findings including symptoms, physical examinations and prior history of disease. 14 Hypertension was diagnosed in patients when the repeated SBP measures were equal to or higher than 140 mmHg, DBP was equal to or higher than 90 mmHg and/or when patients reported a prior history of hypertension and were taking anti-hypertensive medicine at the moment. 15 Diagnoses of coronary heart disease (CHD), stroke and peripheral atherosclerosis disease (PAD) were based on clinical findings from physical examinations, ECG, echocardiography, ultrasound or X-ray imaging and prior history of cardiovascular events.
Values of glucose, HbA1c, total cholesterol, triglyceride and other laboratory measures mentioned previously were log transformed to acquire a normal distribution and geometric means were presented. All the means of continuous variables were calculated with a general linear model except for age. The mean difference of continuous variables between groups was tested with analysis of variance (ANOVA). Chi-square testing was employed to assess the difference in proportions between groups.
Results
Demography and socio-economic status
As shown in Table 1, demographic and socio-economic status varied slightly among patients admitted to the Hospital over the years. Compared to patients entered into EMRs during the first 3 years, those hospitalized in later years were more likely to have social medical insurance coverage. Additionally, patients admitted in the later years were on average older and had a longer duration of diabetes at their initial hospitalization. Regarding patient’s socio-economic data, more than half of the patients had a primary school education (equal to 6 school years), while approximately 5% were illiterate, and 3% had achieved a university education (⩾12 school years). The occupational status between patients hospitalized before and after 2012 could not be compared because the Hospital coding system changed the EMR occupational codes in 2012.
Demographic and clinical characteristics of patients with type 2 diabetes.
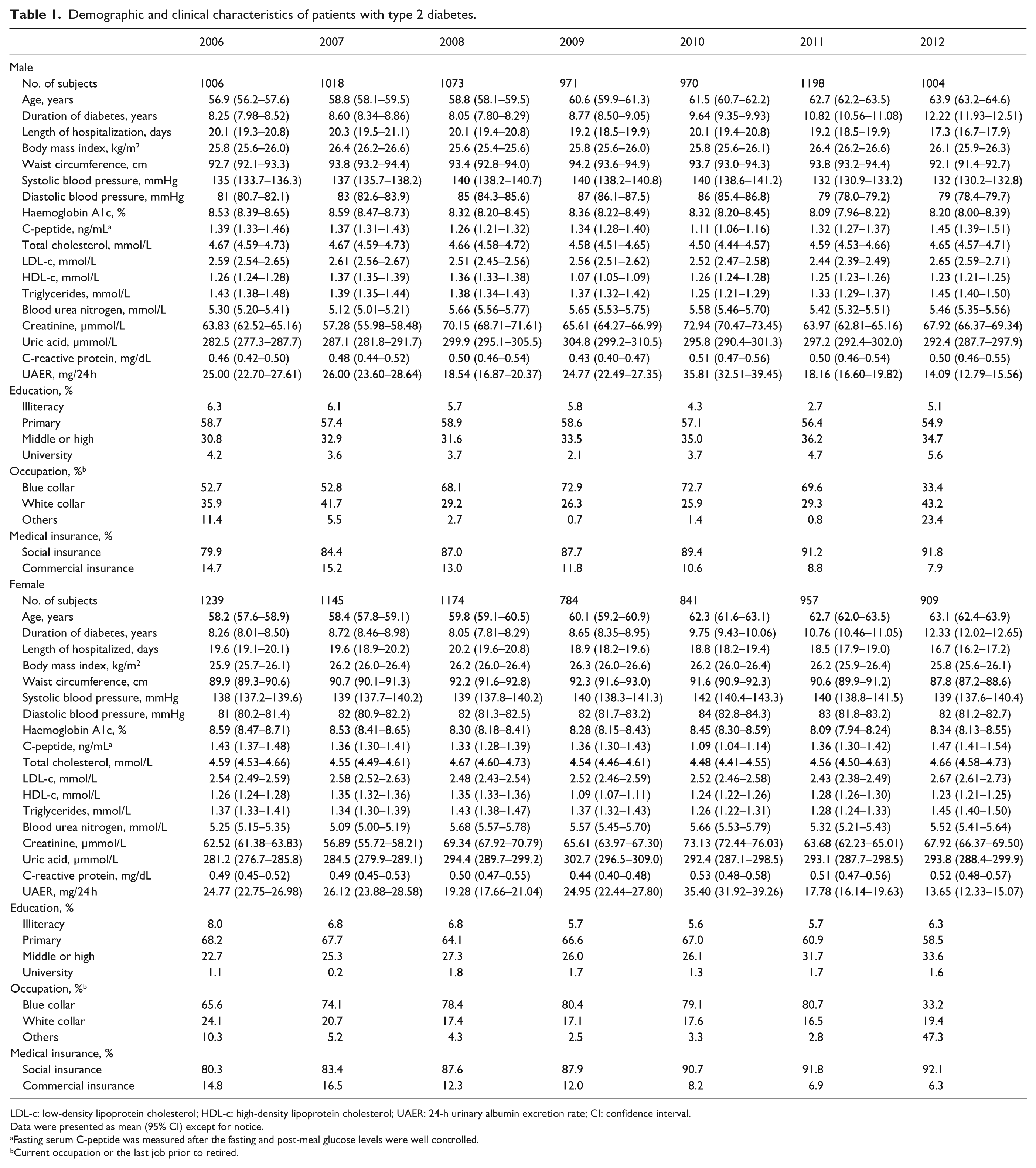
LDL-c: low-density lipoprotein cholesterol; HDL-c: high-density lipoprotein cholesterol; UAER: 24-h urinary albumin excretion rate; CI: confidence interval.
Data were presented as mean (95% CI) except for notice.
Fasting serum C-peptide was measured after the fasting and post-meal glucose levels were well controlled.
Current occupation or the last job prior to retired.
Clinical characteristics and management of metabolic disorders
The mean level of body mass index (BMI), waist circumference, blood pressure, HbA1c and blood lipids varied from year to year (Table 1); however, no secular trends were observed. For most of the patients, their metabolic control was poor prior to admission to the Hospital (Tables 1 and 2). The mean levels of HbA1c were above 8.1% and less than 30.0% of patients had an HbA1c level under 7.0%. Except for male patients hospitalized in 2012, the levels of blood pressure were higher than the optimal values (SBP ⩾ 140 mmHg and/or DBP ⩾ 80 mmHg) in about 75% of the patients. In addition, weight and cholesterol levels were markedly above the guideline recommendations. 10 For instance, over 60% of patients were overweight or obese (BMI ⩾ 24 kg/m2) and about 60% of the patients had LDL-c levels above the optimal values [LDL-c ⩾ 2.6 mmol/L in patients with cardiovascular disease (CVD) or ⩾1.8 mmol/L in those with CVD]. Only 8.2% of the patients achieved all of the targeted HbA1c, blood pressure and LDL-c values.
Prevalence of uncontrolled metabolic disorders in patients with type 2 diabetes.
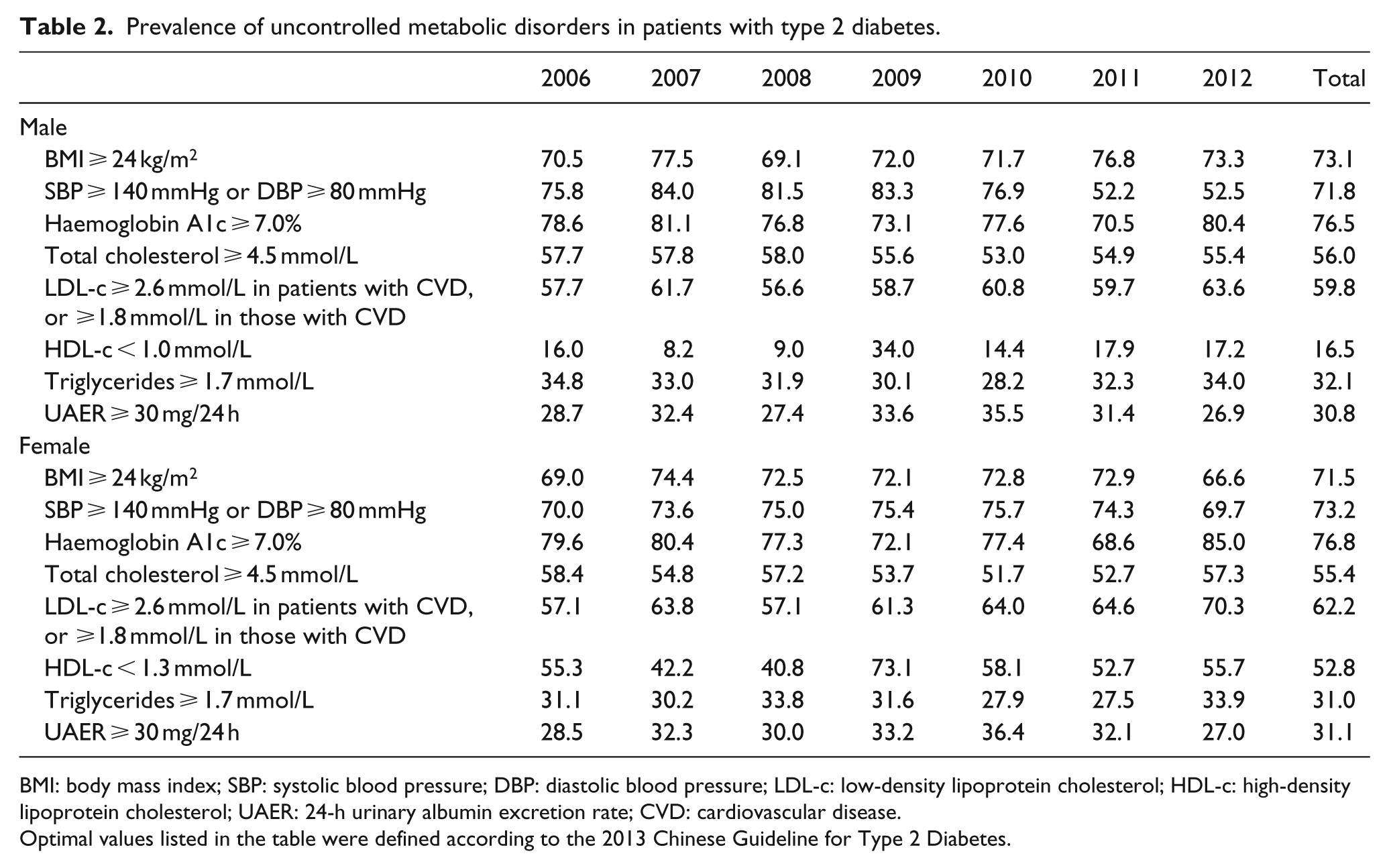
BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; LDL-c: low-density lipoprotein cholesterol; HDL-c: high-density lipoprotein cholesterol; UAER: 24-h urinary albumin excretion rate; CVD: cardiovascular disease.
Optimal values listed in the table were defined according to the 2013 Chinese Guideline for Type 2 Diabetes.
Comorbidities and chronic diabetic complications
Within this patient population, the most prominent complications were DR, DN and peripheral artery atherosclerosis, which occurred in over half of patients (Table 3). Acute diabetic complications including diabetic ketoacidosis, diabetic hyperosmolarity (with coma or not) or diabetic lactic acidosis occurred in approximately 7% of patients. The proportion of patients with an estimated glomerular filtration rate (eGFR) < 60 mL/min/1.73 m2 was greater in females than in males (p < 0.05), while there was no significant gender disparity in the prevalence of micro- or macroalbuminuria. Additionally, the prevalence of CHD was also higher among females (p < 0.05).
Prevalence of comorbidities and diabetic complications among type 2 diabetes patients.
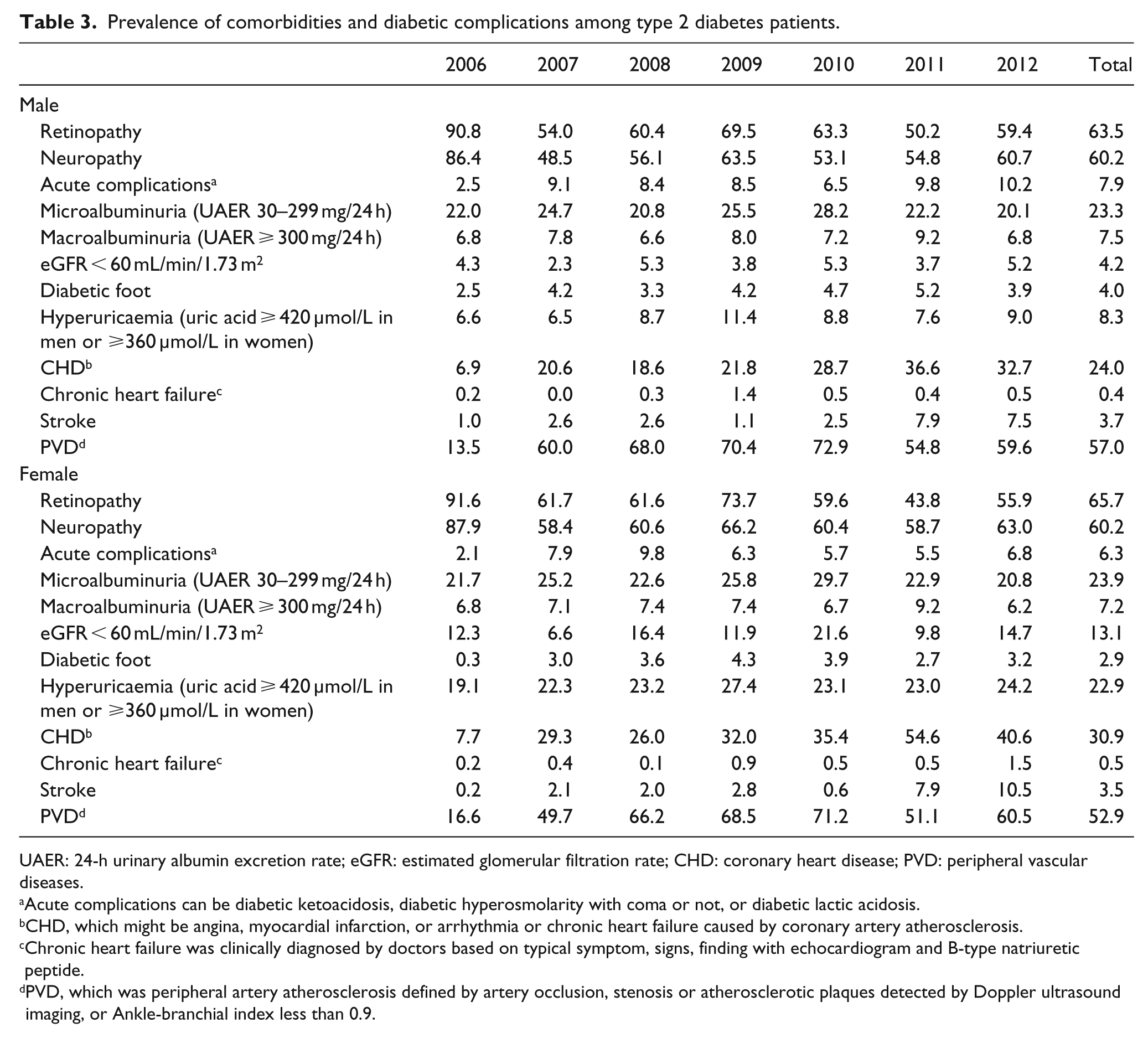
UAER: 24-h urinary albumin excretion rate; eGFR: estimated glomerular filtration rate; CHD: coronary heart disease; PVD: peripheral vascular diseases.
Acute complications can be diabetic ketoacidosis, diabetic hyperosmolarity with coma or not, or diabetic lactic acidosis.
CHD, which might be angina, myocardial infarction, or arrhythmia or chronic heart failure caused by coronary artery atherosclerosis.
Chronic heart failure was clinically diagnosed by doctors based on typical symptom, signs, finding with echocardiogram and B-type natriuretic peptide.
PVD, which was peripheral artery atherosclerosis defined by artery occlusion, stenosis or atherosclerotic plaques detected by Doppler ultrasound imaging, or Ankle-branchial index less than 0.9.
Glucose-lowering drugs
The treatment patterns of glucose-lowering drugs varied little over the study period of 6 years (Table 4). After admission to the hospital, 65%–75% of the patients were prescribed with injectable insulin, either as mono-therapy or combined with other anti-diabetic drugs. Less than 10% of patients received mono-therapy non-insulin anti-diabetic treatment, while two or more non-insulin anti-diabetic drugs were prescribed to 35% of patients. The proportion of patients taking metformin, acarbose, thiazolidinediones, meglitinides and sulfonylureas was 36.9%, 29.9%, 18.1%, 14.8% and 10.7%, respectively. The glucagon-like peptide-1 receptor agonists were prescribed to 3.1% of the patients after it was introduced since November 2009. About 2.7% of the patients took dipeptidyl peptidase 4 inhibitors after it was introduced in October 2011. Furthermore, almost 75% of patients were being treated concomitantly with lipid modulation drugs, 65%–70% received anti-hypertensive drugs and 70%–80% were given anti-platelet agents.
Drug treatment pattern for patients with type 2 diabetes.
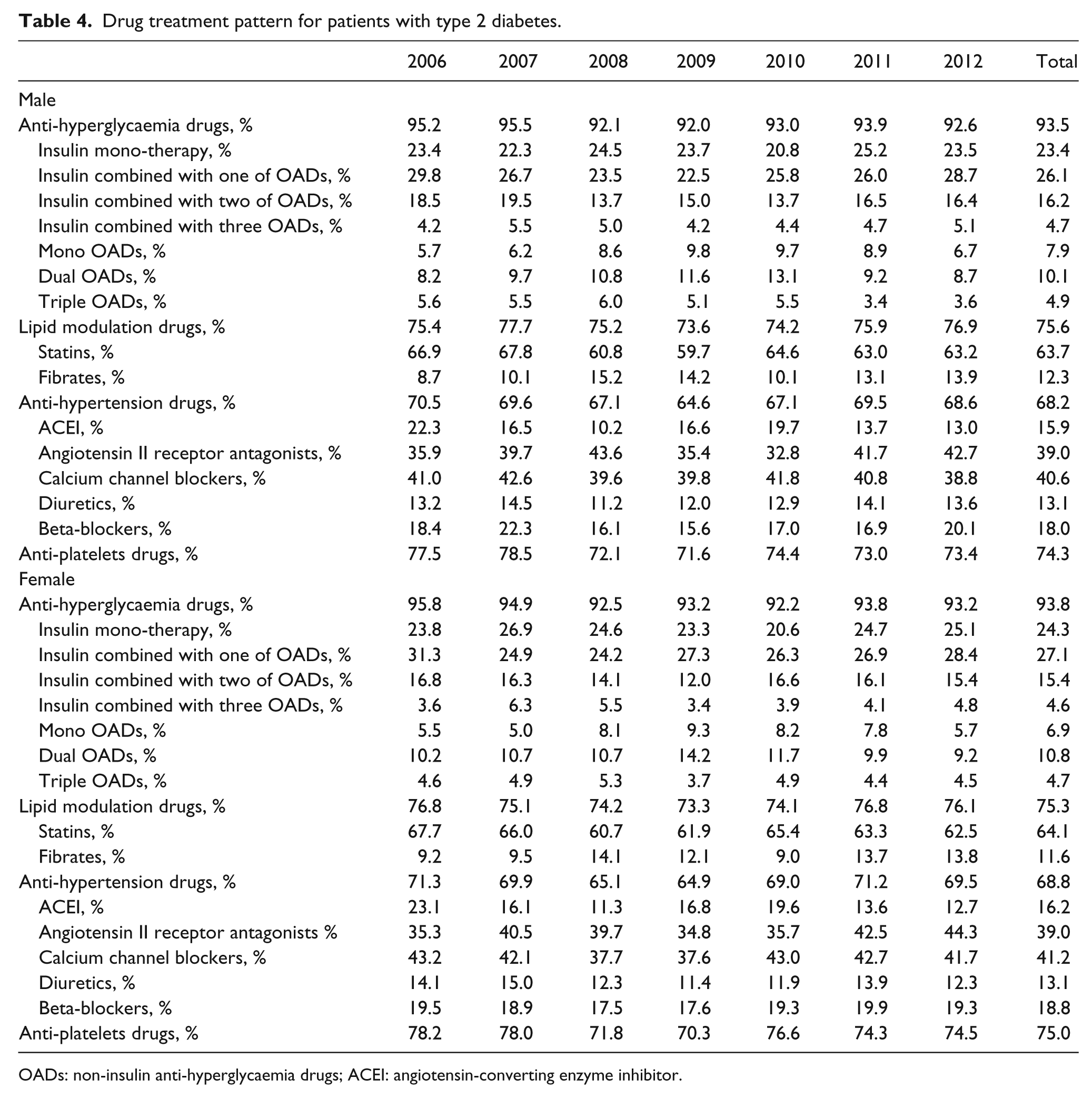
OADs: non-insulin anti-hyperglycaemia drugs; ACEI: angiotensin-converting enzyme inhibitor.
Discussion
Metabolic control was poor among this hospitalized Chinese patient population. Diabetic complications, both micro- and macro-vascular, were prevalent; but no secular trends were observed over this 6-year period. DR, DN and peripheral artery atherosclerosis were the most prevalent comorbidities. Insulin injection was intensively prescribed and combinations of two or more anti-hyperglycaemia agents were common prescription pattern. In addition to anti-hyperglycaemic drugs, most patients received lipid modulation, anti-hypertension and anti-platelets agents. These treatment patterns were quite stable from 2006 to 2012.
The Chinese Diabetes Society conducted four cross-sectional surveys in 1998, 2001, 2003 and 2006 to determine the diabetes control, management and complication status in Chinese diabetic patients, which was known as the Diabcare-China study.9,16 Those surveys were performed in patients who had a mean age of around 60 years and a mean duration of diabetes spanning 8.2–8.7 years and were treated in the study hospitals for at least 1 year. From 1998 to 2006, a decline in mean HbA1c levels were observed from 8.8% to 7.6% and an increase in number of patients who attained the recommended HbA1c treatment goal of <7.0%, from 17.8% in 1998 to 41.1% in 2006. 9 Another Nationwide Assessment of Cardiovascular Risk Factor: Blood Glucose, Blood Pressure, and Blood Lipid in Chinese Patients with Type 2 Diabetes study (3B study) 7 lent support to the Diabcare-China study by showing that 47.7% of the patients had a HbA1c <7.0%. 10 The inpatient cohort in our study had poorer glycaemic control than those included in the two nation-wide studies.
Our inpatient cohort also had a higher prevalence of diabetic complications than those reported in the 3B study 7 and a large-scale cross-sectional Chinese national survey performed in 2011. 17 The prevalence of DN and DR were presented in 15.2% and 16.5% of the patients in the 3B study 7 and 11.0% and 8.3% in the 2011 national survey. 17 However, a study conducted in 2002, which consisted of inpatients, also revealed a highly comorbid population with prevalence estimates similar to those found in our study. In all, 61.8% of the inpatients in their study were diagnosed with DN, 35.7% had diabetic eye diseases and 34.7% had DKD. 8 It is inadvisable to compare these studies directly due to the discrepancies in patient inclusion and exclusion criteria, geographic variations, economic development levels, insurance schemes and capacities in referring and receiving inpatients.
In the Diabcare-China study, it was observed that the prevalence of proteinuria (urinary protein >30 mg/dL) significantly decreased from 20.9% in 1998 to 16.5% in 2006. 9 The reason for the decline was suggested due to better diabetes care including diabetic education, diet and lifestyle changes, improvement in living conditions and economic status, control in blood pressure and lipid levels, in addition to intensive glycaemic control. There was a significant decrease in the mean level of HbA1c over time in this study in spite of the fact that the duration of diabetes of the patients admitted to the hospital has augmented in recent years. However, there were no secular trends in prevalence of diabetic complications in our study population.
In our study, 71.4% of patients received insulin injections at admission and more than 70% were also treated with anti-hypertensive, lipid modulation and anti-platelets drugs, which was much higher than those reported in previous studies. In the Diabcare-China study in 2006, 48.8% of the patients received insulin prescriptions, 9 while it was 35.7% in the 3B study in 2011. 7 The proportion of patients who took anti-hypertensive, lipid modulation and anti-platelets drugs was 42.9%, 23.1% and 18.5%, respectively, in the 3B study. 7 These differences were partially due to more diseased inpatients in our study compared to the other studies mentioned above. In addition, it may also reflect the more favourable attitude towards prescription of insulin injection by Chinese doctors.18,19 Overall, insulin was more frequently administered to patients with T2DM in China than in other countries or regions. For example, the proportion of patients treated with insulin (mono or combined) has been reported to be about 21% in European countries 20 and 23%–25% in Japan. 21
It should be borne in mind when interpreting the results that only patients who had uncontrolled hyperglycaemia, complications and other serious conditions were admitted to the inpatient department for monitored therapy. This partially explains the greater number of diabetic complications observed in our cohort than in other studies7,9,17,22 and the high proportion of patients that received insulin injection. But whether insulin injection was maintained and how long it was maintained after discharge from the hospital cannot be examined from the database where only the first hospital admission was recorded. In addition, as the criteria for admission might be varied among hospitals, it shall be caution to generalize the current finding to other Chinese institutes.
In the current analyses, we excluded about 27% of the patients due to missing key measurements. In order to assess the impact of selection bias, we compared patients included in the study with those excluded and found there was no difference in key characteristics such as mean age, socio-economic status, duration of diabetes, glucose, HbA1c, UAER, lipids and the prevalence of DR, DN and hypertension (data were not shown). Qingdao Endocrine and Diabetes Hospital is a specific hospital, and patients visited the hospital might be different from encounters in a general hospital. Considering China is such a large country with huge differences in dietary cultures and lifestyles, climate, education and economic development status, caution must be taken prior to generalizing the findings from one, although large, hospital to Chinese type 2 diabetes population in general.
Conclusion
In summary, inadequate control of glycaemia, poor metabolic profiles and diabetic complications were common among this inpatient population, revealing the serious consequences of long-term diabetes and the challenge to treat these patients properly in order to prevent disabilities and premature deaths. After hospitalization, patients received intensive treatments to control hyperglycaemia, hypertension and dyslipidaemia. Insulin injections were actively prescribed to the patients and were the most commonly used anti-hyperglycaemia therapy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
Both Y.D. and L.Z. received an unrestricted research grant from AstraZeneca. W.G., J.W., N.H., C.S.C., X.W. and Q.Q. are current employees of AstraZeneca.