
Abstract
Objective:
To characterize copeptin levels and to explore its prognostic importance in patients with acute myocardial infarction with newly detected glucose abnormalities.
Methods:
Copeptin was measured in 166 patients with acute myocardial infarction without known diabetes and in 168 age- and gender-matched controls. Participants were classified as having normal glucose tolerance or abnormal glucose tolerance (impaired glucose tolerance + type 2 diabetes mellitus) by oral glucose tolerance test. Study participants were followed over a decade for major cardiovascular event (acute myocardial infarction/stroke/congestive heart failure/cardiovascular death), cardiovascular and total death.
Results:
Median copeptin level was higher in patients (10.5 pmol/L) than controls (5.9 pmol/L; p < 0.01). Patients with abnormal glucose tolerance had higher copeptin (12.2 pmol/L) than those with normal glucose tolerance (7.9 pmol/L; p < 0.01) but levels of copeptin did not differ in controls with abnormal glucose tolerance or normal glucose tolerance. Copeptin predicted major cardiovascular events [n = 64; hazard ratio = 1.15 (1.01–1.32; p = 0.04)], cardiovascular mortality [n = 29; hazard ratio = 1.24 (1.06–1.46; p = 0.01)] and total death [n = 51; hazard ratio = 1.21 (1.05–1.40; p = 0.01)] in unadjusted Cox regression analyses in the patient cohort. In controls, copeptin predicted major cardiovascular events [n = 26; hazard ratio = 1.17 (1.01–1.36; p = 0.03)].
Conclusion:
Copeptin levels are highest among acute myocardial infarction patients with glucose disturbances and predict an adverse prognosis in unadjusted analyses. These findings imply that raised copeptin reflects stress rather than acting as a pathogenic factor for glucose abnormalities.
Introduction
The mechanisms behind the predisposition in patients with type 2 diabetes mellitus (T2DM) to develop macrovascular complications and to have a more dismal prognosis when this occurs are not fully understood.1,2 This encourages investigations of potential pathophysiological pathways.
Activation of the arginine vasopressin system during stress, expressed as elevated levels of copeptin, a stable, inactive split product of the vasopressin pre-hormone, is associated with a poor prognosis after acute myocardial infarction (AMI) and in heart failure patients.3–5
In addition, elevated copeptin is related to risk factors of glucometabolic disturbances, such as obesity and hyperinsulinaemia, and independently associated with the risk of developing T2DM. 6
Elevated copeptin levels may be secondary to stress in these conditions, but an alternate hypothesis is that an amplified activation of the vasopressin system may be involved in the pathophysiology of cardiovascular disease, in particular among patients with glucose abnormalities, making it a factor of prognostic importance.
The aims of the present report, a substudy from the Glucose in Acute Myocardial Infarction (GAMI) study, are to (1) characterize the copeptin pattern in patients with AMI without previously known diabetes and compare them to age- and sex-matched healthy controls, (2) investigate if this pattern differs between individuals with normal glucose tolerance (NGT) or abnormal glucose tolerance (AGT) and (3) explore if copeptin has any prognostic implication.
Methods
Data source and study participants
The GAMI trial recruited patients who were admitted for AMI to two coronary care units in Sweden from November 1998 to December 2000. All individuals were free from previously known T2DM and had a baseline capillary blood glucose <11.1 mmol/L, serum creatinine <200 µmol/L and age ≤80 years. A detailed description of the patients has been presented elsewhere.7,8 A total of 181 participants were enrolled, of whom 168 were characterized before hospital discharge, by means of an oral glucose tolerance test (OGTT), as having NGT, impaired glucose tolerance (IGT) or T2DM according to the 1998 World Health Organization (WHO) classification. 9 The term AGT is used for the presence of either IGT or T2DM. Sex- and age-matched controls (n = 185) without previously known diabetes or cardiovascular disease except hypertension were recruited from the general Swedish population during January 2001 to July 2002. The patients and controls were followed until 31 December 2011. One patient and one control were lost to follow-up.10,11
This study comprises study participants who had blood samples from their recruiting hospitalization or baseline for controls, available for copeptin measurements (166 patients and 168 controls). In this subset, glucose categorization at discharge was available in 154 patients (NGT = 48,AGT = 106) and in all controls (NGT = 109, AGT = 59).
Laboratory analyses
Blood glucose and creatinine were measured as soon as possible after arrival to the coronary care unit and HbA1C (reported as MonoS) on the first morning after admission. Biochemical parameters, such as high-sensitivity C-reactive protein (hs-CRP) and copeptin, were analysed in fasting samples taken on the day after hospital admission. A detailed description of laboratory methods used in the GAMI study has been presented elsewhere. 7
Copeptin was analysed locally at the Cardiology Unit, Department of Medicine, Solna, Karolinska Institutet with an automated immunofluorescent assay (BRAHMS Copeptin ultrasensitive KRYPTOR) with a lower detection limit of 0.9 pmol/L, functional assay sensitivity <2 pmol and interassay coefficient of variation 20%.
Outcomes
In the present report, copeptin was studied in relation to three of the original endpoints: (1) total mortality; (2) cardiovascular mortality defined as death from myocardial infarction (MI), stroke, aortic dissection or sudden death without any obvious reason; and (3) major cardiovascular event defined as the first occurrence of AMI, stroke, severe congestive heart failure or cardiovascular death. The total time of follow-up was 11.6 years for patients and 10.4 years for controls.
Statistical methods
Continuous variables are presented as median and interquartile ranges (IQRs) and categorical data as number and percentages unless otherwise stated. Fisher’s exact test (dichotomous variables) and Wilcoxon two-sample test (continuous variables) were used to assess differences in baseline characteristics between patients and controls. Hettmansperger and Mckean linear model aligned rank tests were performed to adjust copeptin levels for differences in age when comparing levels between individuals with and without AGT. 12 The Wilcoxon two-sample test was used to study differences in copeptin levels in the subsets stratified by dichotomous variables [gender, previous MI, previous hypertension, previous heart failure and treatment with angiotensin-converting enzyme (ACE) inhibitor, thiazide or furosemide at admission for patients and at baseline for controls] (Supplementary Table 1, available online). Correlations between copeptin levels and continuous variables [age, body mass index (BMI), glucose, HbA1c, creatinine and hs-CRP] were assessed using Spearman’s rank correlation test (Supplementary Table 2, available online). Differences in copeptin level between individuals with and without events were assessed with Wilcoxon two-sample test. The relationship between an increase in one standard deviation (SD) of copeptin and events was assessed using Cox’s proportional hazard regression and is presented as hazard ratio (HR) and 95% confidence intervals (CIs). The SD was calculated separately for each subgroup at admission (patients) and study visit (controls) was used as baseline. Copeptin was separately adjusted for the following variables one at a time: age, admission creatinine (only available in patients), gender, previous congestive heart failure, previous MI, BMI and HbA1c. These covariates were selected based on results from a previous report by Mellbin et al. 13 on copeptin in patients with AMI and T2DM and in addition on clinical experience. 14 Multiple and step wise models were not performed due to low number of events. All analyses were done using SAS version 9.4 (SAS Institute).
Ethical considerations
The local ethics committee of the Karolinska Institutet, Stockholm, Sweden, approved the study protocol that complies with the Declaration of Helsinki. All recruited participants provided their written informed consent for the initial study and the follow-up.
Results
Patients’ characteristics
Baseline characteristics of patients and controls are presented in Table 1. In general, patients and controls were matched based on gender and age. The median age was 64 years, and about just below one-third were women in both groups. Patients were more often smokers with a family history of ischaemic heart disease (IHD), previous cardiovascular disease manifestations, more pharmacological treatments and had higher HbA1c values than controls. Patients with NGT were significantly younger and had lower blood glucose and copeptin levels than the AGT patients (data not shown). A similar subdivision of the controls revealed that those with NGT were younger, with lower HbA1c, a less frequent history of hypertension and less often prescribed β-blockers than controls with AGT (data not shown).
Baseline characteristics at admission or the day after hospital admission.
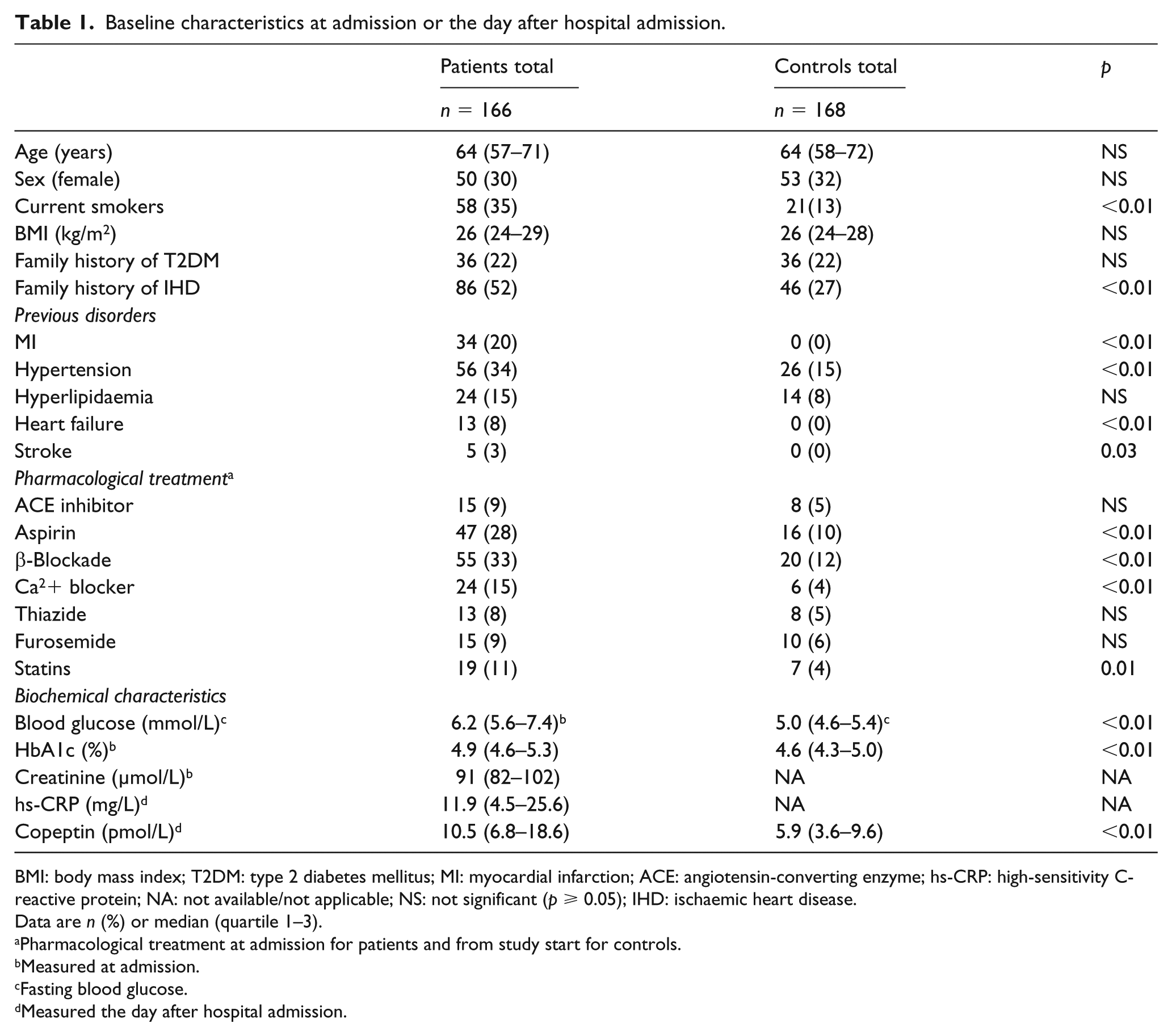
BMI: body mass index; T2DM: type 2 diabetes mellitus; MI: myocardial infarction; ACE: angiotensin-converting enzyme; hs-CRP: high-sensitivity C-reactive protein; NA: not available/not applicable; NS: not significant (p ≥ 0.05); IHD: ischaemic heart disease.
Data are n (%) or median (quartile 1–3).
Pharmacological treatment at admission for patients and from study start for controls.
Measured at admission.
Fasting blood glucose.
Measured the day after hospital admission.
Copeptin levels
The median copeptin level (Table 1) was significantly higher in patients (10.5 pmol/L) than controls (5.9 pmol/L; p < 0.001). As depicted in Figure 1, copeptin was lower in patients with NGT (7.9 pmol/L) compared to those with AGT (12.2 pmol/L; p < 0.01), a pattern that remained after adjustment for age (p = 0.03). In the control population, copeptin did not differ significantly between individuals with NGT (5.6 pmol/L) and AGT (6.5 pmol/L) as depicted in Figure 1. Copeptin did not differ between patients or controls with IGT (n = 58) and T2DM (n = 55; data not shown).
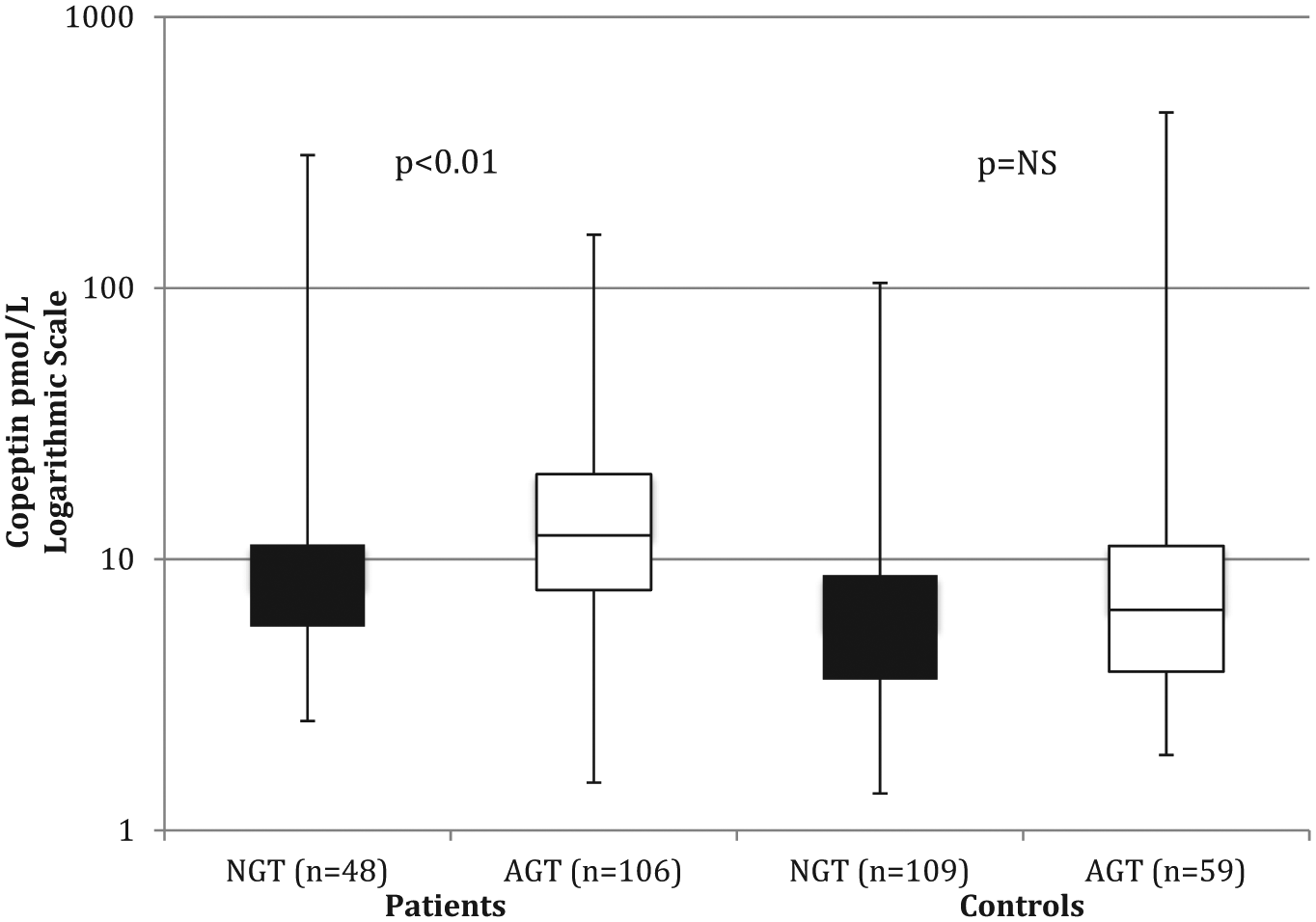
Copeptin levels (pmol/L) in the subset of patients (n = 154) and controls (n = 168) with known glucose categorization (defined by an OGTT). Boxes span the 25th–75th percentile and whiskers outline minimum and maximum levels. p-value = Kruskal–Wallis test.
Copeptin levels were higher in males than among females in the total patient population (males: 11.5 vs females: 8.5 pmol/L; p = 0.04) as well as for patients with NGT. Likewise, there was a gender difference in the same direction in the total control population (males: 7.1 pmol/L vs females: 4.4 pmol/L; p < 0.01) and after classification based on glucose category (Supplementary Table 1).
Patients with previous congestive heart failure in the total cohort had significantly higher values of copeptin compared to those without (21.0 vs 10.1; p < 0.01). No such difference was found in those with and without hypertension, previous MI, treatment with ACE inhibitors or diuretics neither in the patient nor in the control group, and there were no consistent differences in the subgroups with NGT and AGT (Supplementary Table 1).
There was a positive correlation between copeptin and age both among patients (r = 0.33; p < 0.01) and controls (r = 0.17; p = 0.04). This correlation remained significant for patients but not for controls following a subdivision in those with NGT and AGT (Supplementary Table 2). Creatinine levels correlated positively to copeptin in the total patient cohort (r = 0.27; p < 0.01) and in patients with AGT (r = 0.23; p = 0.02). BMI and HbA1c had a positive correlation with copeptin in the total control (r = 0.18; p = 0.02 and r = 0.20; p = 0.01 respectively) but not in the total patient cohort.
Prognostic influence of copeptin
The total number of events during the decade of follow-up is outlined in Table 2. Patients and controls who experienced any event had significantly higher copeptin levels than those who did not (Table 2). After a subdivision of the individuals with events into those with NGT and AGT, this pattern, higher copeptin among those with events, persisted although it did not reach statistical significance in all subgroups.
The median level (IQR) of copeptin (pmol/L) in patients and controls with and without events.
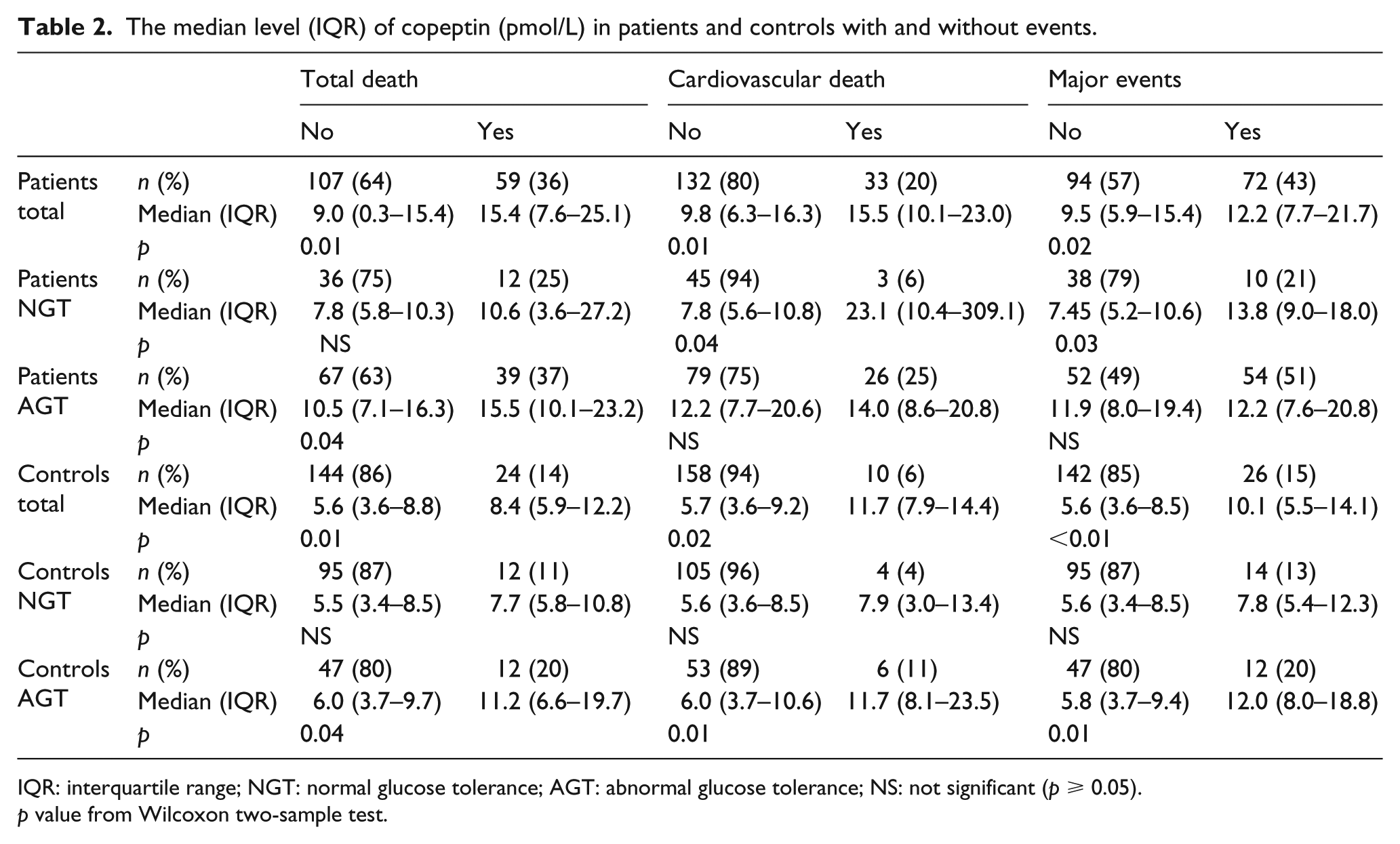
IQR: interquartile range; NGT: normal glucose tolerance; AGT: abnormal glucose tolerance; NS: not significant (p ≥ 0.05).
p value from Wilcoxon two-sample test.
In an unadjusted Cox regression analysis for patients, an increase of 1 SD of copeptin predicted major cardiovascular events (p = 0.04), cardiovascular death (p < 0.01) and total death (p < 0.01; Figure 2). Copeptin remained a significant predictor of total death and cardiovascular mortality among patients after adjusting for each of the following variables alone: gender, admission creatinine, previous congestive heart failure and HbA1c but failed to predict after adjusting for single adjustments for age, previous AMI and BMI (Supplementary Table 3, available online). Copeptin remained as a significant predictor of a major cardiovascular event only after adjusting for gender and HbA1c.
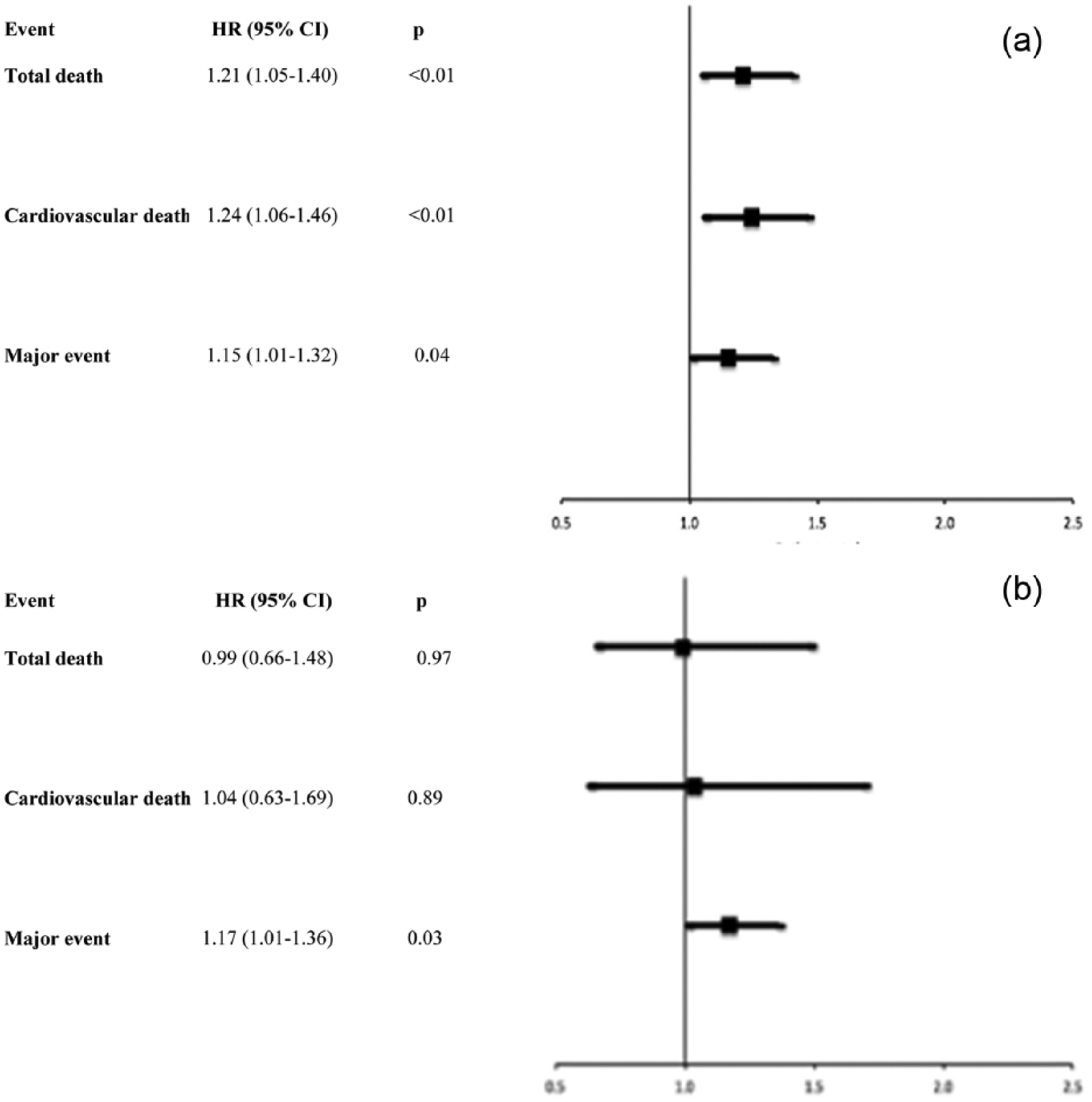
Unadjusted predictive ability of copeptin in the (a) total patient cohort and (b) total control cohort assessed by Cox’s proportional hazard regression (+1 SD). HR: hazard ratio; 95% CI: 95% confidence interval.
Since copeptin did not remain a predictor for any of the events after adjusting for AMI, and some of the other variables, further adjustments in multivariate models were not performed.
When patients were subgrouped by glucose category, copeptin predicted both total death [HR = 1.38 (95% CI, 1.03–1.84; p = 0.03)] and cardiovascular mortality [HR = 1.58 (95% CI, 1.12–2.24; p = 0.01)] in the NGT group but failed to predict major cardiovascular events [HR = 1.35 (95% CI, 1.00–1.83; ns)]. In the AGT subgroup, copeptin did only predict major cardiovascular events [HR = 1.28 (95% CI, 1.02–1.61; p = 0.04)], which was lost after adjusting for any of the covariates listed above except gender and HbA1c (Supplementary Table 3).
Among controls, copeptin predicted major cardiovascular events [HR = 1.17 (95% CI, 1.01–1.36; p = 0.03)] but none of the other endpoints (Figure 2). This remained after adjustments for each covariate separately, except BMI and gender (Supplementary Table 4, available online). Further adjustments were not performed due to the low number of events. When dividing controls into those with NGT and AGT, respectively, copeptin did not predict any events.
Discussion
The major finding was that copeptin was highest among patients with AMI in the presence of AGT. Controls had lower copeptin levels than patients with AMI, but there was no difference between controls with or without glucose abnormalities. In patients with AMI, copeptin was a weak predictor of cardiovascular events, cardiovascular and total mortality in unadjusted analyses and predicted cardiovascular events in AGT patients. The results indicate that patients with glucose abnormalities may be more susceptible to stress and the negative cardiac effects of vasopressin activation.
As vasopressin is a well-known stress hormone, 15 it is not surprising that copeptin levels were higher among patients than controls. The present data gets support by findings by Khan et al. 3 reporting on median levels of 7.0 pmol/L measured 3–5 days after admission for AMI, while controls had lower levels, 3.8 pmol/L.
Interestingly, GAMI patients with AGT had significantly higher copeptin levels compared to patients without glucose abnormalities. Khan et al. noted a similar pattern reporting that patients with known diabetes (21.8%) had significantly higher copeptin levels (median, 8.9 pmol/L) compared to those without diabetes (6.5 pmol/L). The current report shows that higher copeptin levels are also present in patients with newly detected AGT.
The AGT and NGT patients had quite similar baseline characteristics apart from that the former patients were older. Since copeptin and age correlate in the present analysis, age may be a confounder but copeptin remained higher in the AGT group even after adjustment for age.
The NGT patients had lower blood glucose but neither glucose nor HbA1c correlated to copeptin, which was the reason to abstain from further adjustments including these variables.
An intriguing question is whether the elevated copeptin level in patients with AGT, indicating activation of the vasopressin system, is a marker of increased response to stress or if vasopressin activation is a pathogenetic factor behind the glucose abnormalities. Copeptin predicted the development of diabetes independently from established clinical risk factors in a Swedish population-based study (n = 4742) with 12.6 years of follow-up. 6 Furthermore, patients with known diabetes at baseline had significantly higher copeptin values (6.9 pmol/L) than those with normal fasting glucose (5.1 pmol/L). The authors suggested that their result support that vasopressin activation may be involved in the pathophysiology of diabetes development, and there are indeed several potential pathways. It may, for example, be a direct effect via activation of the hepatic VIa vasopressin receptors that are linked to glucose metabolism or act through insulin resistance caused by activation of the V1b receptors.15,16 Another possibility is that the impact of vasopressin on glucose metabolism is mediated by other hormonal systems, such as the insulin-like growth factor/insulin-like growth factor-binding protein axis (IGF-I-IGFBP axis). Disturbances in this axis are associated with a susceptibility to development of glucose abnormalities.17,18 An association between IGFBP-1 and copeptin has been reported, and it appears as vasopressin can explain at least some of the prognostic capacity of IGFBP-1 as previously demonstrated in patients with AMI and T2DM. 13 This association was, however, not confirmed in the Beta-cell function in Glucose Abnormalities and Myocardial Infarction (BEGAMI) study, comprising a similar study population as in the GAMI, which may relate to the small sample size in the BEGAMI. 19 In contrast to the previously mentioned Swedish population-based study, there were no significant differences in the copeptin levels between individuals with NGT and AGT in the present control group. 6 A possible explanation for discrepancy may be differences in samples size. In contrast, copeptin levels differed in patients with NGT and AGT. These findings are in line with the possibility that vasopressin should be seen as marker of stress rather than a direct pathogenetic factor for diabetes. One may speculate that patients with glucose abnormalities are more susceptible to stress induced by the AMI and in parallel to the subsequent vasopressin activation. This may explain why patients with AGT have higher copeptin values than those with NGT and the lack of a difference in the less stressful control setting. It may, however, also be that patients with AGT are at a higher risk for a more extensive myocardial damage provoking increased copeptin levels. Unfortunately, the present data do not allow further elaboration on this issue.
Copeptin has previously been described as a predictor of cardiovascular outcome for patients with AMI, both with and without diabetes.3,13 Furthermore, copeptin predicts heart disease caused by diabetes and mortality in diabetes outpatients. 20 This was partly confirmed by this study in which copeptin was a significant predictor for all studied outcomes among patients although it did not remain statistically significant after separately adjusting for confounders, in particular previous AMI. Furthermore, copeptin did not consistently predict all studied events in the control group. This may be a result of lack of power due to a relatively low number of events notably among controls, a limitation of the present analyses. It may also be that other factors, for example, previous AMI, are more important in this setting than vasopressin.
In the AGT patient group, copeptin predicted major cardiovascular events. As already speculated upon, AGT patients may be more susceptible to AMI-related stress which may result in increased vasopressin activation. Vasopressin has known direct detrimental cardiac effects such as vasoconstriction, increasing the preload and afterload and also stimulation of myocardial hypertrophy. 15 Such effects may be particularly threatening in the presence of glucose abnormalities since such patients are known to have an increased risk of congestive heart failure and subsequent mortality.21,22 Furthermore, vasopressin has prothrombotic effects23,24 and, since diabetes per se is a prothrombotic condition, vasopressin activation may be particularly harmful in patients with AGT. 25 In addition, a possible negative impact on glucose metabolism induced by vasopressin activation directly or indirectly as mentioned above may further deteriorate the prognosis in patients with glucose abnormalities.
Conclusion
Copeptin levels were highest among AMI patients with glucose disturbances and did in unadjusted analyses predict an adverse prognosis during the following decade. As discussed, the most likely explanation to the present results is that vasopressin activation is a reflection of stress rather than causally involved in the pathophysiological process of the progression of dysglycaemic disorders. In addition, patients with AGT may be more susceptible to vasopressin activation, making negative cardiac consequences particularly harmful in such patients, who already are prone to develop congestive heart failure and who have an increased thrombogenicity.
Footnotes
Acknowledgements
The authors wish to thank Christina Edman Jönsson, RN, at the Cardiology Unit at Karolinska University Hospital Solna for performing the copeptin analyses.
Declaration of conflicting interests
Dr Gyberg reports personal fees from MSD Sweden and grants from Swedish Heart and Lung Foundation, outside the submitted work. Dr Rydén reports grants from Swedish Heart Lung Foundation, grants from Swedish Diabetes Foundation and grants from Karolinska Institutet Funds, during the conduct of the study. Dr Mellbin reports personal fees from MSD Sweden and other from Sanofi Aventis, grants from Bayer AG, outside the submitted work. Dr Norhammar reports grants from Swedish Heart Lung Foundation, grants from Swedish Diabetes Foundation and grants from Karolinska Institutet Funds, during the conduct of the study. Other authors have no competing interests.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.