
Abstract
Objectives:
We aimed to determine the prevalence of echocardiographic abnormalities and their relation to clinical characteristics and cardiac symptoms in a large, contemporary cohort of patients with type 2 diabetes.
Results:
A total of 1030 patients with type 2 diabetes participated. Echocardiographic abnormalities were present in 513 (49.8%) patients, mainly driven by a high prevalence of diastolic dysfunction 178 (19.4%), left ventricular hypertrophy 213 (21.0%) and left atrial enlargement, 200 (19.6%). The prevalence increased markedly with age from 31.1% in the youngest group (<55 years) to 73.9% in the oldest group (>75 years) (p < 0.001) and was equally distributed among the sexes (p = 0.76). In univariate analyses, electrocardiographic abnormalities, age, body mass index, known coronary heart disease, hypertension, albuminuria, diabetes duration and creatinine were associated with abnormal echocardiography along with dyspnoea and characteristic chest pain (p < 0.05 for all). Neither of the cardiac symptoms nor clinical characteristics had sufficient sensitivity and specificity to accurately identify patients with abnormal echocardiography.
Conclusion:
Echocardiographic abnormalities are very common in outpatients with type 2 diabetes, but neither cardiac symptoms nor clinical characteristics are effective to identify patients with echocardiographic abnormalities.
Introduction
Despite improvements in preventive care for patients with type 2 diabetes, cardiovascular disease remains the most common cause of death among these patients.1,2 To address this, the European guidelines recommend that echocardiography should be considered in the diagnostic work-up of patients with type 2 diabetes even in the absence of known cardiovascular disease 3 – not least because of a high prevalence of subclinical cardiac abnormalities in these patients.4,5 The cardiac changes associated with diabetes are thought to comprise thickening of the myocardium and is characterised by predominantly diastolic dysfunction, the diabetic cardiomyopathy. Accordingly, a number of studies have reported a high prevalence of diastolic dysfunction in this patient group.4,6,7 In addition, because of advancing age and comorbidities, including hypertension and obesity, patients with type 2 diabetes are also prone to other cardiac pathologies affecting prognosis including but not limited to left ventricular hypertrophy,8,9 reduced left and right ventricular ejection fraction, 10 dilated left atrium 11 or valve disorders. 12
However, previous reports on prevalence of echocardiographic findings were based on populations that were either small6,7,13,14 from the primary care setting/general population4,15,16 or included patients before the era of modern multifactorial treatment. 17 Even more, contemporary, intensive treatment of hypertension, hyperglycaemia, dyslipidemia and lifestyle factors 18 may have changed the risk profile for having echocardiographic abnormalities making it difficult to choose which patients to refer to echocardiography. Thus, knowledge on echocardiographic abnormalities and their association with cardiac symptoms and clinical characteristics from a large, contemporary cohort of patients with type 2 diabetes is lacking.
Therefore, we set out to (1) determine the prevalence of echocardiographic abnormalities in a large cohort of multifactorially treated outpatients with type 2 diabetes followed at large secondary care centres using comprehensive, up-to-date echocardiographic methods, (2) determine their relation to cardiac symptoms and clinical characteristics and (3) evaluate these as basis of referral to echocardiography.
Methods
Study population
The Thousand & 2 Study is a representative sample of patients with type 2 diabetes initiated in October 2011 at the Department of Cardiology, Herlev and Gentofte Hospital, University of Copenhagen. Patients were recruited from Steno Diabetes Center (SDC) – which is an integrated part of the Danish health care system – and Center for Diabetes Research (CfD), Department of Medicine, Herlev and Gentofte Hospital, University of Copenhagen. Both are high volume centres; SDC provides care to approximately 2500 patients with type 2 diabetes and CfD to approximately 1200 patients. Patients from the primary sector with inadequate glycaemic control or diabetes-related complications are referred to the centres to optimise medical treatment. Patients with less well-controlled type 2 and/or increasing severity of complications and/or co-morbidity are followed continuously with specialised and multidisciplinary treatment in the outpatient clinics.
All patients with type 2 diabetes followed at either centre were eligible to participate. Invitations were sent by mail and the patients were subsequently contacted by telephone or email. From October 2011 to March 2012, all patients (n = 747) from CfD were invited to participate and 409 accepted (54.7%). From April 2012 to December 2013, 1411 patients from SDC were invited and 621 accepted (44.0%) yielding an overall participation rate of 47.8%. Data on baseline characteristics of responders versus non-responders are shown in supplemental Table 1.
The study was conducted in accordance with the Helsinki Declaration, approved by The Danish National Committee on Biomedical Research Ethics, amendment to protocol no. H-3-2009-139. 19 All participants gave written informed consent.
Study visit
Prior to the study visit, patients received study information and answered questionnaire on diabetes duration, presence of diabetic complications, current medication, prior heart disease (myocardial infarction, percutaneous coronary intervention, coronary artery bypass grafting, congestive heart failure and atrial fibrillation), prior stroke and peripheral artery disease, hypertension, hypercholesterolaemia, family history of coronary artery disease, known lung disease (asthma and chronic obstructive lung disease), smoking habits, exercise, alcohol consumption, height and weight. At the visit, the questionnaire including current medication was reviewed with the patient. Cardiac symptoms, dyspnoea and chest pain were evaluated with the patient by investigator P.G.J. Dyspnoea was graded mild when corresponding to New York Heart Association class II and moderate/severe when class III–IV. Chest pain was graded characteristic when reported as central, oppressive and occurring in relation to physical exercise and uncharacteristic when not. A 12-lead electrocardiogram was collected (Cardiosoft version 6.61, GE Healthcare) and interpreted at a time later than the study visit and, thus, independently of the echocardiographic examination by a single experienced interpreter (P.G.J.). Electrocardiographic abnormalities were defined as pathologic/abnormal Q-waves, ST-segment and T-wave changes and left and right bundle branch block.
Blood pressure was measured in supine position with a cuff adjusted to arm circumferential after at least 15 min of rest. Hypertension was defined as patients receiving antihypertensive medication or systolic blood pressure >140 mm Hg or diastolic blood pressure >90 mm Hg. Atrial fibrillation was considered present when either self-reported or present at the time of the echocardiography.
Biochemistry
For patients from CfD, laboratory values, including haemoglobin A1c (HbA1c), lipid profile and creatinine were measured prior to each visit and for patients from SDC, laboratory values were measured at the visit at SDC preceding the study visit. Measurements of urine albumin/creatinine ratio or 24 h urine albumin excretion rate were performed at least once per year and repeated in case of elevated levels. Microalbuminuria was defined as urine albumin/creatinine ratio between 30 and 300 mg/g or urine albumin excretion rate between 30 and 300 mg/day, and macroalbuminuria as urine albumin/creatinine ratio above 300 mg/g or urine albumin excretion rate above 300 mg/day in two consecutive measurements. Albuminuria was considered as present when either micro- or macroalbuminuria was present.
Echocardiography
Echocardiography was performed with General Electric, Vivid 7 and Vivid E9 (GE Vingmed Ultrasound, Horten, Norway). The offline analyses were performed using GE EchoPAC software, BT13. The echocardiograms were performed (>95%) and interpreted by P.G.J. and validated the same day by a cardiologist with specialty in echocardiography blinded to patient data. Chamber quantification was done in accordance with the recommendations of the European Association of Echocardiography (EAE) and the American Society of Echocardiography (ASE). 20 Left ventricular (LV) mass was calculated using the formula LV mass = 0.8 × [1.04((LV internal diameter + posterior wall thickness + septal wall thickness) 3 − (LV internal diameter) 3 )] + 0.6 g and indexed according to height 2 . 7 Hypertrophy was defined as ⩾45 g/m2 for women and ⩾49 g/m2 for men. 21 Left atrial (LA) end-systolic size was calculated using the area-length method, where left atrial volume = 8/3 × π (LA area in 4 chamber view × LA area in 2 chamber view/shortest long axis length in either view) and increased atrial size indexed for body surface area was defined as >34 mL/m2. 20 Aortic measurements were performed in the aortic root and the ascending aorta and evaluated according to age and body surface area corrected normal values. 20 LV ejection fraction was assessed using Simpson’s biplane method, and reduced LV ejection fraction was considered when <50%. Diastolic dysfunction was considered present when the ratio of early mitral valve inflow velocity to septal early diastolic tissue Doppler velocity (E/e′) was >15. This cut-off was chosen because it accurately identifies patients with elevated filling pressures 22 and because it accurately identifies high-risk type 2 diabetes patients. 23 Right ventricular function was assessed using tricuspid annular plane systolic excursion and considered reduced when <1.7 cm. Presence and grading of valvular heart disease was performed with an integrative approach as suggested by the EAE24,25 and was considered present when more than moderate. Systolic anterior motion (SAM) of the anterior mitral valve leaflet was visually identified and if present, Doppler measurements of left ventricular outflow tract gradients during Valsalva were recorded. An echocardiogram was considered abnormal when at least one of the above-mentioned was present.
Statistics
Continuous variables were compared using Welsh’s t-tests or analysis of variance when more than one group. In case of non-normal distribution, Mann-Whitney U tests or Kruskall-Wallis tests were used, where appropriate. Missing data were omitted from the analyses. Categorical variables were compared using Chi-square tests. Univariate and multivariate associations with abnormal echocardiograms were tested using logistic regression. Variables that were significantly associated with echocardiographic abnormalities (p < 0.05) were entered in the multivariable model. For continuous variables, the optimal cut-off point for sensitivity and specificity was determined as the shortest distance to the upper left corner of the receiver operating characteristics curve. Statistics were calculated using R for Mac, version 2.15.3 (R Project for Statistical Computing, Vienna University of Economics and Business Administration, Wien, Austria).
Results
A total of 1030 patients with type 2 diabetes were included from SDC and CfD in the study (Figure 1). The clinical characteristics of this population are shown in column 1 in Table 1.
Flow chart of inclusion of patients with type 2 diabetes in the Thousand & 2 Echo Study.
Clinical characteristics of the study population.
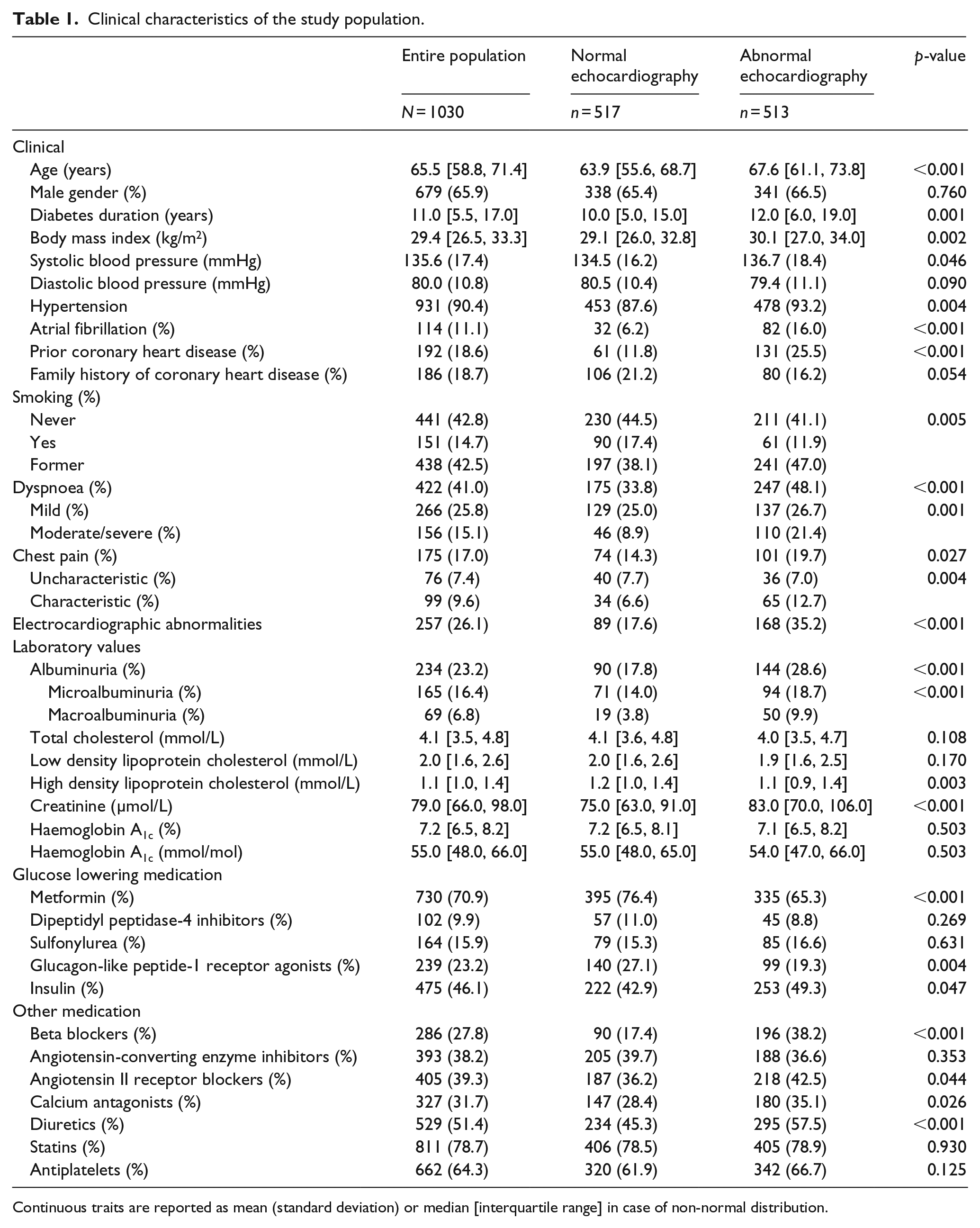
Continuous traits are reported as mean (standard deviation) or median [interquartile range] in case of non-normal distribution.
Echocardiographic findings
An abnormal echocardiogram was found in 49.8% of the patients, with hypertrophy, diastolic dysfunction and left atrial enlargement accounting for the largest part with a prevalence of about 20% for each, but also, 12.5% of the population had systolic dysfunction. Valvulopathy was not common and was present in only 3.6% of the population. Patients with abnormal echocardiography were older, had longer diabetes duration, larger body mass index, higher systolic blood pressure, more often had atrial fibrillation, coronary heart disease, dyspnoea, electrocardiographic abnormalities, albuminuria, higher levels of serum creatinine and lower levels of high-density lipoprotein cholesterol. In addition, they were more often treated with insulin, beta-blockers, angiotensin II receptor blockers, calcium antagonists, diuretics and less frequently with metformin and glucagon-like peptide-1 receptor agonists.
Women had borderline-significant more diastolic dysfunction and hypertrophy than men, whereas men more often than women had reduced left ventricular ejection fraction, reduced right ventricular function and increased atrial size (Table 2). The prevalence of abnormal echocardiogram in the population increased sharply with age, from 31.1% in the youngest group (<55 years) to 73.9% in the oldest group (>75 years), predominantly caused by sharp increases in prevalence of diastolic dysfunction, hypertrophy, reduced right ventricular function and increased left atrial size (Table 3).
Echocardiographic findings of the entire population of outpatients with type 2 diabetes and stratified by sex.
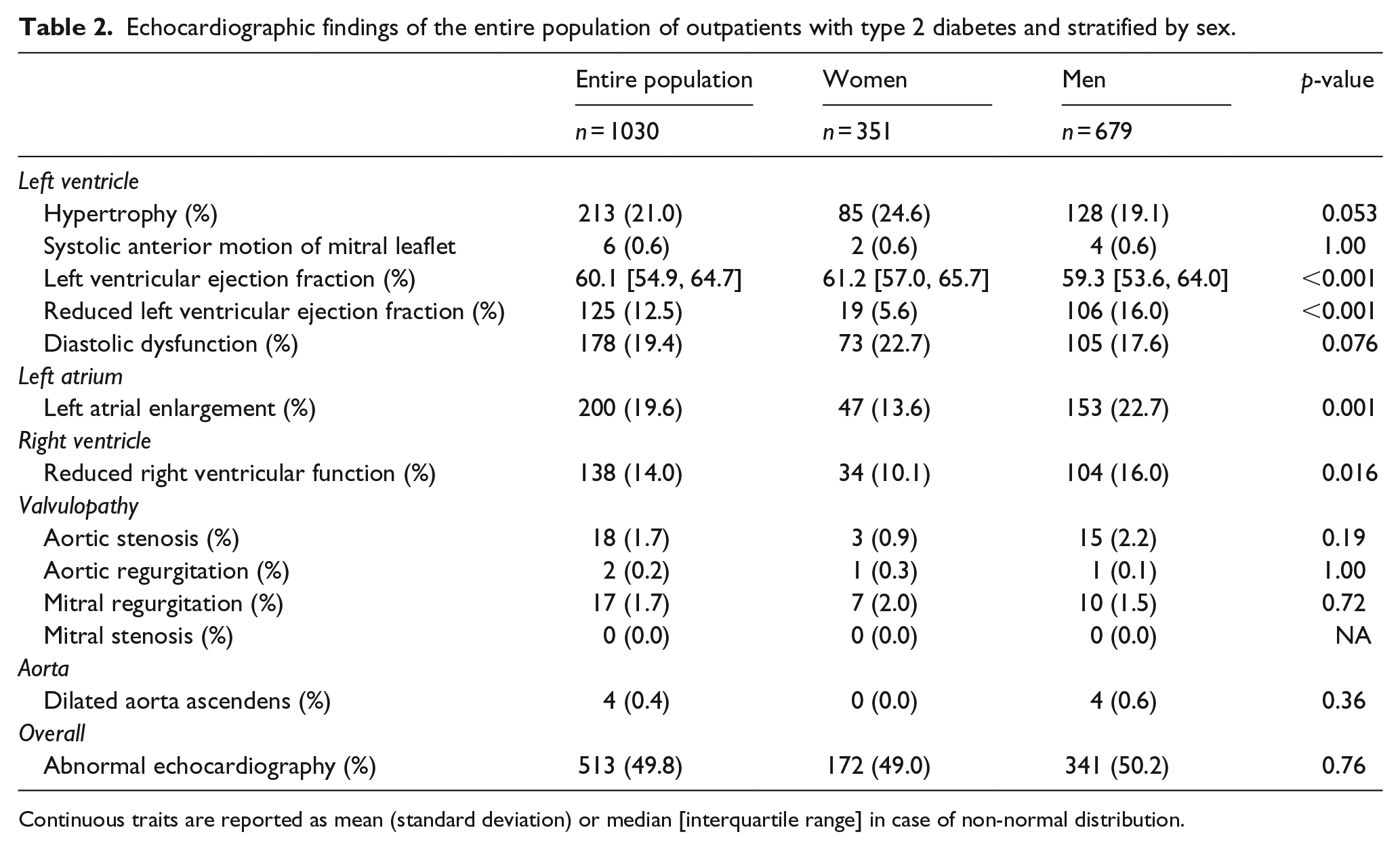
Continuous traits are reported as mean (standard deviation) or median [interquartile range] in case of non-normal distribution.
Echocardiographic findings of outpatients with type 2 diabetes stratified by age.
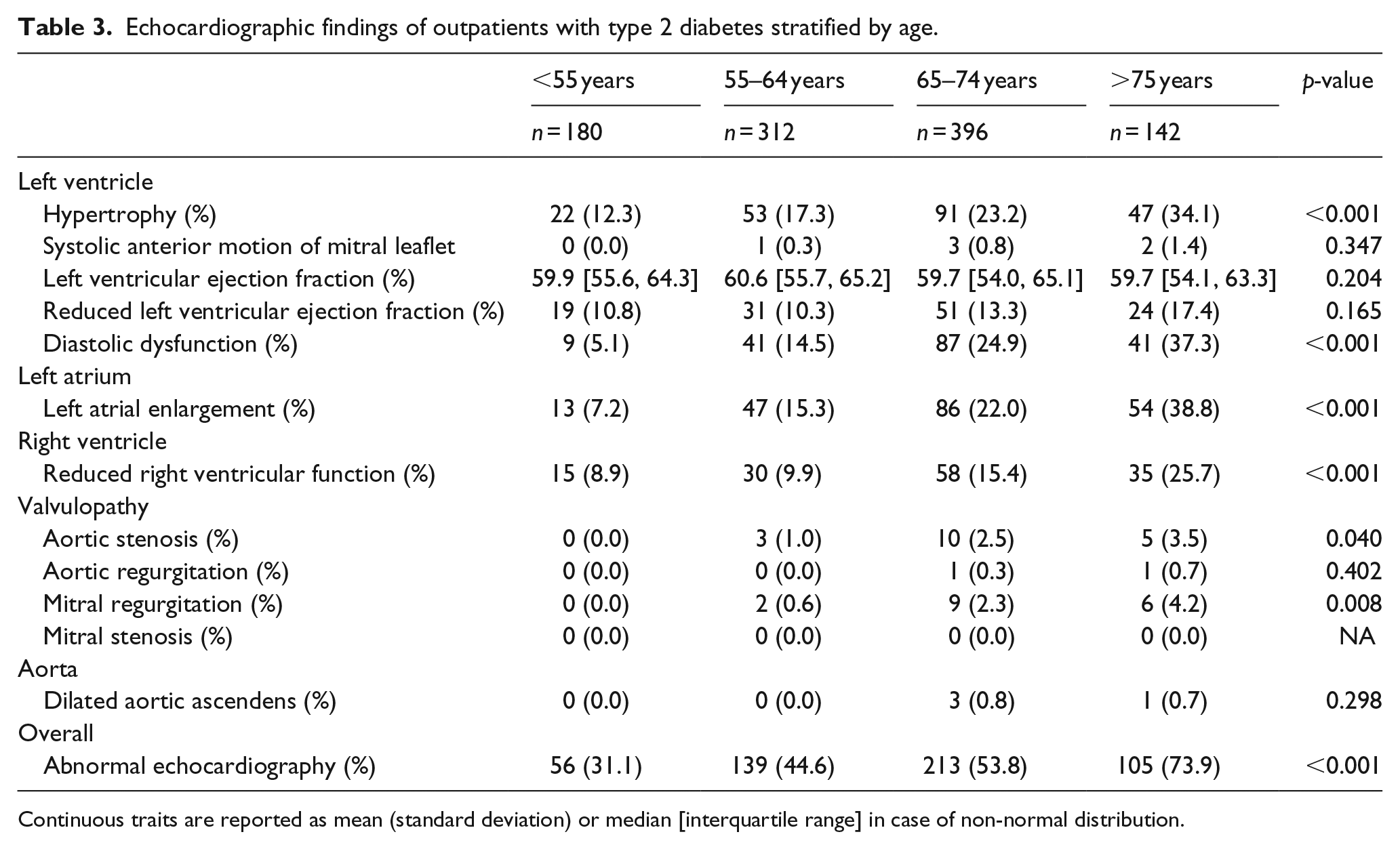
Continuous traits are reported as mean (standard deviation) or median [interquartile range] in case of non-normal distribution.
Univariable factors associated with abnormal echocardiography
Univariable associations of cardiac symptoms and clinical characteristics are shown in Figure 2. Complaining of either dyspnoea or chest pain was associated with an abnormal echocardiogram especially when the dyspnoea was moderate to severe, which had the strongest association with abnormal echocardiography of both symptoms and clinical characteristics. However, chest pain was only associated with abnormal echocardiography when characteristic in which case an approximate twofold increase in risk was observed. In addition, patients with electrocardiographic abnormalities had an approximate 2.5-fold increased risk of having echocardiographic abnormalities, which was similar to known coronary heart disease. Also, increasing age, hypertension, body mass index, diabetes duration, albuminuria, creatinine levels and insulin treatment were significantly associated with abnormalities. On the contrary, we did not find an association with HbA1c, male sex or total-cholesterol.
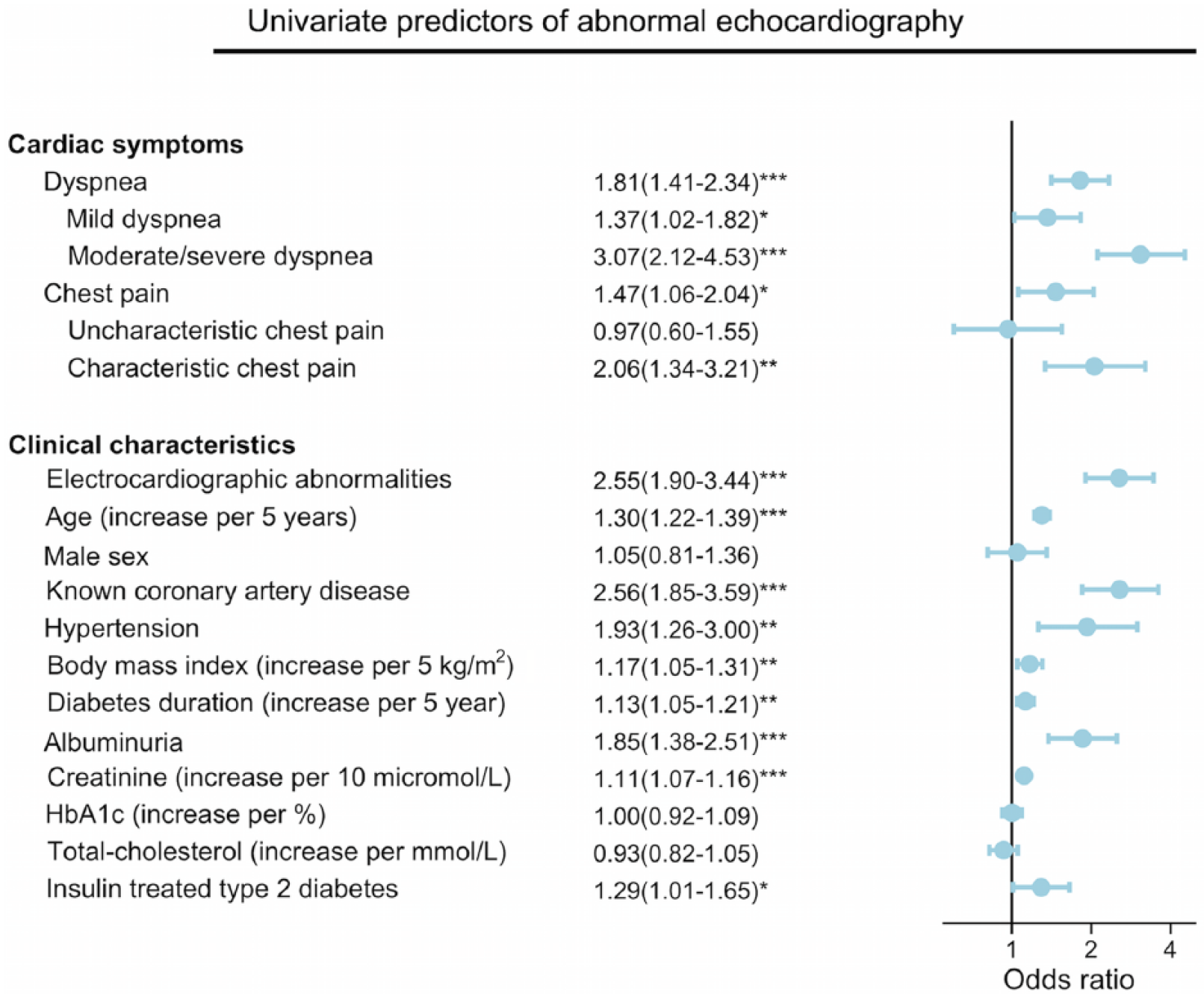
Univariate predictors of abnormal echocardiography in outpatients with type 2 diabetes.
The sensitivity, specificity, positive and negative predictive value of cardiac symptoms and statistically significant predictors are shown in Table 4. For all cardiac symptoms, a low sensitivity (12.7%–48.1%) and negative predictive value (51.8%–56.3%) was found, whereas specificity and positive predictive values were moderate for overall dyspnoea (66.1% and 58.3%) and chest pain (85.5% and 57.7%) and good for moderate/severe dyspnoea (91.1% and 70.5%) and characteristic chest pain (93.4% and 65.7%). Of clinical characteristics, the same pattern was repeated for electrocardiographic abnormalities, known coronary heart disease and albuminuria. For hypertension, on the other hand, a high sensitivity was found (93.2%), but at the cost of a very low specificity (12.4%).
Sensitivity, specificity, positive and negative predictive value of univariate statistically significant clinical characteristics and cardiac symptoms for abnormal echocardiography in outpatients with type 2 diabetes.
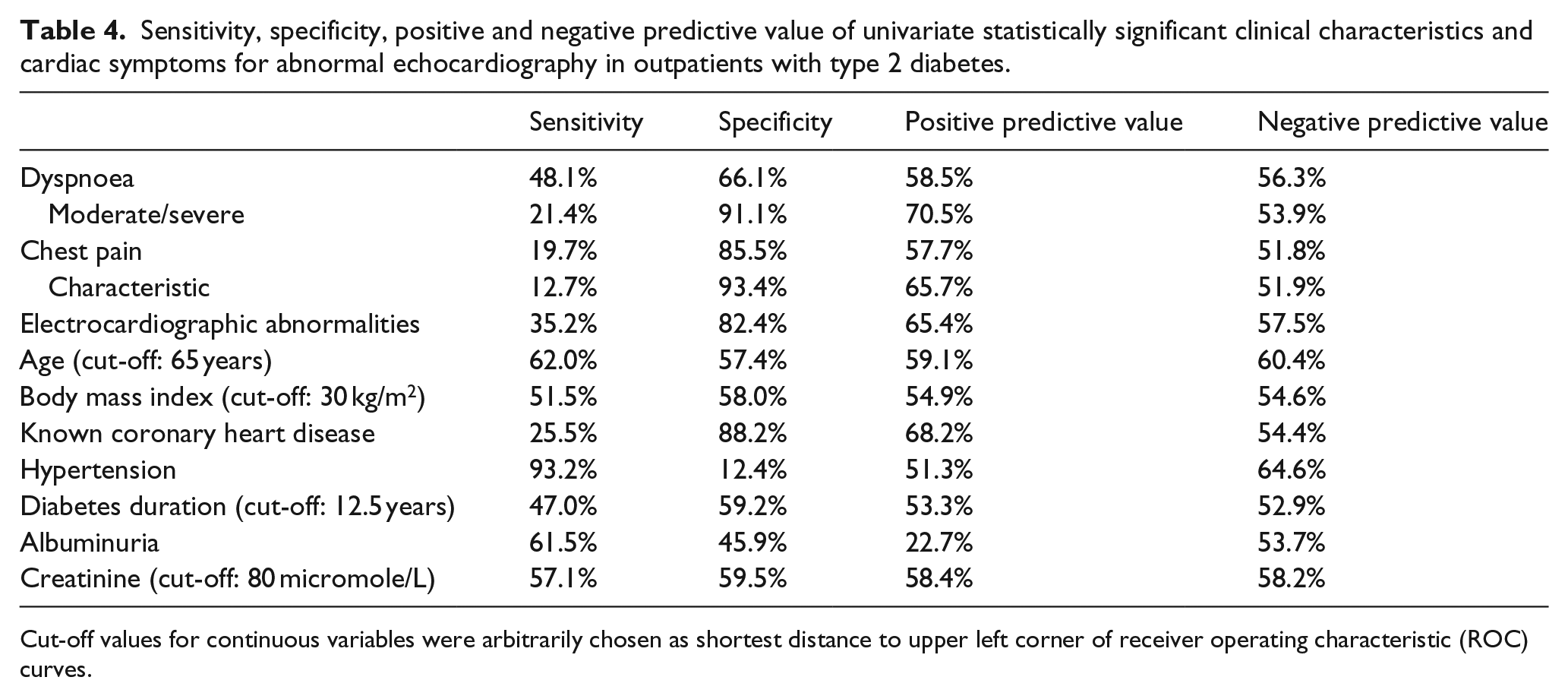
Cut-off values for continuous variables were arbitrarily chosen as shortest distance to upper left corner of receiver operating characteristic (ROC) curves.
Adjusted analyses
In multivariate, logistic regression – including cardiac symptoms and clinical characteristics that were significantly associated with abnormal echocardiography in univariate analyses – we found that age (per 5 year increase) [odds ratio (OR): 1.25 (95% confidence interval (CI): 1.25–1.35), p < 0.001], electrocardiographic abnormalities [OR: 1.83 (95% CI: 1.32–.54), p < 0.001], known coronary heart disease [OR: 1.63 (95% CI: 1.11–2.40), p = 0.01], body mass index (per 5 kg/m2 increase)[OR: 1.24 (95% CI: 1.09–1.41), p < 0.001] and albuminuria [OR: 1.55 (95% CI: 1.10–2.19), p = 0.013] independently were associated with abnormal echocardiography.
Discussion
This study is, to our knowledge, the largest study to date designed to specifically address the prevalence of echocardiographic abnormalities in patients with type 2 diabetes. Our primary findings are that echocardiographic abnormalities are present in about 50% of the population, and that this is driven mainly by the presence of myocardial abnormalities – including left ventricular hypertrophy, systolic and diastolic dysfunction – and subsequently dilated left atrium reflecting high filling pressures caused by the impaired myocardial function.
Also, we found that cardiac symptoms including dyspnoea and chest pain were associated with echocardiographic abnormalities, however, with very low sensitivity. Presence of electrocardiographic abnormalities, known coronary heart disease, hypertension, albuminuria, increasing age, body mass index, diabetes duration and creatinine levels were also associated with echocardiographic abnormalities but again with low sensitivity and negative predictive value. Hypertension, on the other hand, showed high sensitivity, but low specificity and positive and negative predictive value. Thus, relying on symptoms or clinical characteristics to decide which patients to refer to echocardiography will fail to identify a large proportion of patients with echocardiographic abnormalities except if presence of hypertension is used in which case about 90% of the patients would have to be referred.
Important determinants of echocardiographic abnormalities
In this study, we found a sex difference in echocardiographic abnormalities in patients with type 2 diabetes, with women tending to have more left ventricular hypertrophy and diastolic dysfunction, whereas men more often had reduced left ventricular ejection fraction, reduced right ventricular function and left atrial enlargement. Similar sex differences in cardiac structure and function have been reported previously in the Framingham cohort, where women with diabetes – but not men – had increased left ventricular mass and men with diabetes – but not women – had decreased fractional shortening, a measure of systolic function. 26 These findings, however, were not confirmed in the Strong Heart Study, where both men and women had increased left ventricular mass and decreased fractional shortening. 27
Also, besides sex differences, we have shown that the prevalence increases sharply with age and that abnormal echocardiography has a very high prevalence in patients with type 2 diabetes >75 years of age, driven mainly by left ventricular hypertrophy, left atrial enlargement and diastolic dysfunction. Hence, our study confirms that increasing age is a very important determinant of cardiac abnormalities, and further research is needed to address the specific effect of diabetes on cardiac structure and function in the ageing population.
Interestingly, presence of albuminuria was associated with echocardiographic abnormalities in both uni- and multivariable analyses. Accordingly, previous studies have suggested an association of high levels of urinary albumin excretion and development of heart failure in patients with type 2 diabetes and either microalbuminuria 28 or hypertension. 29 In addition, albeit in patients with type 1 diabetes, we have previously published a subtle decrease in cardiac function without known heart disease and albuminuria. 30 In this light, our study further underlines the importance of albuminuria as a marker of cardiac abnormalities in patients with type 2 diabetes.
Prevalence of systolic and diastolic dysfunction in patients with type 2 diabetes
Previous studies on echocardiographic abnormalities in patients with type 2 diabetes have primarily focused on the prevalence of systolic and diastolic dysfunction and heart failure to identify patients with diabetic cardiomyopathy.6,7,14 This is not restricted to type 2 diabetes, and we have previously reported a high prevalence of diastolic dysfunction in patients with type 1 diabetes without known heart disease, in which similar sex differences were found. 19 In type 2 diabetes, however, small-sized populations have reported considerable variation in the prevalence of diastolic dysfunction, ranging from 40% to 75%. One study has even reported no differences in diastolic function between healthy subjects and patients with type 2 diabetes free from hypertension, coronary artery disease and microangiopathic complications. 31 This was, however, with a much smaller sample size (n = 78) than in this study and using older criteria for diastolic dysfunction. In a recent study Boonman de-Winter et al. assessed both the prevalence of systolic and diastolic dysfunction in a primary care setting and found a prevalence of 0.7% and 25.1%, respectively, in 581 patients with type 2 diabetes without known heart failure. They also estimated the prevalence of cardiologist confirmed heart failure in this population and found that 96.3% of the patients with newly detected heart failure had diastolic dysfunction. 4 The discrepancy in prevalence between the previous and the present studies lies in the differences in the criteria for establishing the presence of diastolic dysfunction. In our study, we have used the ratio of early mitral valve inflow velocity to septal early diastolic tissue Doppler velocity (E/e′) that in previous studies has been linked to poor prognosis in patients with type 2 diabetes. 23 This measure, however, is more conservative as it will only classify patients with definitely abnormal diastolic function and not the patients with borderline abnormal diastolic function. This – of course – makes our estimates of prevalence more conservative, but on the other hand identifies a subgroup with verified increased risk.
Other cardiac abnormalities in patients with type 2 diabetes
Left ventricular hypertrophy is a well-established precursor both of systolic dysfunction 32 and overall cardiovascular disease.33,34 Though typically associated with hypertension, 8 its prevalence increases with increasing age, body mass index and presence of hypertension and diabetes; 9 all the characteristics of a population of outpatients with type 2 diabetes. Hence, left ventricular hypertrophy is a very relevant concern in this population, and in accordance, we found a prevalence of 24.6% in women and 19.1% in men. However, further research is needed to determine the isolated effect of diabetes in this population.
Left atrial enlargement reflects elevated left ventricular filling pressures in the ailing heart and is associated with stroke and mortality in the general population, patients with myocardial infarction and ischaemic cardiomyopathy.35–37 Of note, Poulsen et al. 11 recently found that left atrial enlargement is associated with a composite end-point of all-cause mortality and cardiovascular events in patients with type 2 diabetes. In this context, this overall increased risk can be assigned to approximately one-fifth of our population.
In contrast, we did not find increased prevalence of valvular heart disease when comparing to a large-scale community study. 12 In this study, the prevalence of valvular heart disease increased sharply from 1.9% in the 55–64 years old to as high as 13.2% in patients above 75 years. In accordance, we found a prevalence of 1.6% in the 55–64 years old and 8.4% in the patients above 75 years old. However, our study is likely to be underpowered for any accurate assessment of the prevalence of valvular heart disease in patients with type 2 diabetes.
Strengths and limitation
The study has great strength in that it was designed specifically to address echocardiography in a large cohort of outpatients with type 2 diabetes. Also, all examinations were comprehensive, reviewed by at least two observers and assessed using the latest published guidelines. However, an important limitation has to be mentioned: All patients were recruited from specialised outpatient clinics. Hence, the findings should not be extrapolated to all patients with type 2 diabetes especially not to those treated in primary care setting. Also, selection bias cannot be excluded in this study, though the overall characteristics of the responders and non-responders were quite similar as shown in supplemental Table 1.
Conclusion
In outpatients with type 2 diabetes, echocardiographic abnormalities are frequently found and associated to both cardiac symptoms and clinical characteristics. However, no single measure accurately identifies echocardiographic abnormalities with high sensitivity and specificity and, hence, referral to echocardiography should be considered in most patients regardless of cardiac symptoms and clinical characteristics.
Footnotes
Declaration of conflicting interests
Tina Vilsbøll has received lecture fees from AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Eli Lilly and Company, Merck Sharp & Dohme, Novo Nordisk, Novartis and Sanofi, and is a member of the Amgen, Advisory Boards of AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Eli Lilly and Company, Merck Sharp & Dohme, Novo Nordisk, and Sanofi. Peter Rossing reports grants from and shares in Novo Nordisk. Advisory boards in Merck Sharp & Dohme (MSD), AstraZeneca, Boehringer, Eli Lilly, Janssen, Novo Nordisk Astellas and Abbvie (all fees to institution). Lecture fee to institution from Bayer.
Funding
The study was supported by the Carl and Ellen Hertz foundation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.