
Abstract
Objective:
To investigate whether serum advanced glycation endproducts are associated with left ventricular systolic and diastolic function in participants with normal glucose metabolism, impaired glucose metabolism and type 2 diabetes mellitus.
Methods:
Participants from a cross-sectional, population-based study (n = 280 with normal glucose metabolism, n = 171 with impaired glucose metabolism, n = 242 with type 2 diabetes mellitus) underwent echocardiography. Serum protein-bound advanced glycation endproducts [i.e. Nε-(carboxymethyl)lysine, pentosidine and Nε-(carboxyethyl)lysine] were measured. Linear regression analyses were used and stratified according to glucose metabolism status.
Results:
In normal glucose metabolism, higher Nε-(carboxymethyl)lysine and pentosidine levels were associated with worse diastolic function (left atrial volume index and left atrial volume × left ventricular mass index product term) and higher Nε-(carboxymethyl)lysine and Nε-(carboxyethyl)lysine levels with worse systolic function (ejection fraction). In impaired glucose metabolism, a similar pattern emerged, though less consistent. In type 2 diabetes mellitus, these associations were non-existent for diastolic function or even reversed for systolic function.
Conclusion:
This suggests that serum advanced glycation endproducts are associated with impaired left ventricular function in normal glucose metabolism, but that with deteriorating glucose metabolism status, serum advanced glycation endproducts may not mirror heart failure risk.
Keywords
Introduction
Type 2 diabetes mellitus (T2DM) is associated with an increased risk of heart failure. 1 This increased risk is only partially understood as it is not fully explained by traditional cardiovascular disease (CVD) risk factors. 1
It has been suggested that advanced glycation endproducts (AGEs) play an important role in the pathobiology of heart failure.2,3 For example, AGEs may impair both diastolic and systolic left ventricular (LV) function directly, through extracellular matrix protein cross-linkage and/or altered calcium handling, and/or indirectly, through the interaction with cardiac AGE receptors, which in turn lead to low-grade inflammation, increased oxidative stress and altered gene expression.2–4 Consequently, AGEs may also unfavourably affect the process of LV remodeling.2–4 The impact of AGEs on LV function may be of particular importance in T2DM, as T2DM is characterized by chronic hyperglycaemia and hyperlipidaemia, which in turn can induce the formation of AGEs, as well as oxidative stress and low-grade inflammation, which can further enhance the formation of AGEs.2,4–6
However, previous studies on the association between circulating AGEs and LV structure and function showed mixed results. For example, some studies,7–9 but not all, 10 showed that higher circulating AGEs were associated with impaired diastolic function. Such mixed results were also seen for systolic function. For example, Berg et al. 8 reported positive associations of circulating AGEs with systolic function, whereas such associations were absent in a study by Steine et al. 11 In addition, only a few studies reported on the association between circulating AGEs and indices of LV structure.8,10 These studies were, in addition, small (i.e. n < 60),7–11 done in selected populations (e.g. patients undergoing coronary bypass surgery, 7 patients with type 1 diabetes8,9,11 or with end-stage renal disease 10 ) and did not investigate the role of deteriorating glucose metabolism on the association between circulating AGEs and LV function.8–11
Therefore, we investigated, in a large population-based cohort stratified according to glucose metabolism status (GMS), the associations between the serum AGEs, Nε-(carboxymethyl)lysine (CML), pentosidine and Nε-(carboxyethyl)lysine (CEL) and LV function and structure. We hypothesized that serum AGEs would be associated with impaired LV function and unfavourably altered LV structure. In addition, we hypothesized that any such association would be stronger in individuals with impaired glucose metabolism (IGM) and T2DM.
Methods
Study population
For the current study, we used data from the 2000 Hoorn Study. The Hoorn study, which started in 1989, is a population-based cohort study of GMS in relation to CVD risk factors. 12 In brief, 2484 men and women, aged 50–75 years, from the population register of the medium-sized Dutch town of Hoorn participated in the baseline examination. In 1996–1998, 1513 (73%) of all surviving participants agreed to participate in a follow-up visit. In 2000, all those who were diagnosed as having diabetes during the previous examinations (n = 176) and random samples of individuals with normal glucose metabolism (NGM) (n = 705) and IGM (n = 193) were invited, of whom 648 (60%) participated. To increase the number of individuals with T2DM, 188 individuals with T2DM from the Hoorn Screening study were added. 13 The total study population, therefore, consisted of 836 individuals. 14 The study complied with the Declaration of Helsinki. The Medical Ethical Review Committee of the VU University Medical Center, Amsterdam, has approved the research protocol, and written informed consent has been obtained from all participants.
Measurement of AGEs
AGEs were measured in serum samples, obtained from fasting venous blood, which were stored at −80°C until analysis. Protein-bound CML, CEL and lysine were measured by means of ultra-performance liquid chromatography tandem mass spectrometry, as described in detail elsewhere. 15 Intra- and interassay coefficients of variation were 4.8% and 7.0% for CML, 5.0% and 9.7% for CEL and 2.7% and 4.9% for lysine, respectively. 15 Protein-bound pentosidine was measured using high-performance liquid chromatography with fluorescent detection, as described in detail elsewhere. 16 Intra- and interassay coefficients of variation for pentosidine were 6.5% and 3.1%, respectively. 16 Concentrations of protein-bound CML, CEL and pentosidine were adjusted for levels of lysine and expressed as nmol/mmol lysine.
Echocardiography
Echocardiography was performed according to a standardized protocol consisting of two-dimensional and M-mode assessments as previously described. 17 A Hewlett-Packard SONOS 5500 echocardiography system (2–4 MHz transducer, Andover, MA, USA) was used. Measurements of LV structure [as determined by interventricular septum thickness, posterior wall thickness, LV end-diastolic diameter, relative wall thickness and left ventricular mass index (LVMI)] were performed in M-mode and determined according to the American Society of Echocardiography 2005 recommendations. 18 Systolic function was defined with the use of monoplane Simpson’s LV ejection fraction, calculated from the LV systolic and diastolic volumes in the apical four chamber view. For diastolic function, two markers were used: left atrial (LA) volume index and the LA volume × LVMI product term.19,20
Other measurements
Individuals’ GMS was defined according to the 1999 WHO criteria 21 with an oral glucose tolerance test as previously described. 14 Study covariates included age, sex, GMS, hypertension (defined as systolic/diastolic blood pressure greater than 140/90 mmHg and/or use of blood pressure-lowering medication 22 ), total cholesterol–high-density lipoprotein cholesterol ratio, triglycerides, use of lipid-modifying medication, prior CVD, current smoking, waist circumference, estimated glomerular filtration rate (eGFR), 23 homeostasis assessment model for insulin resistance (HOMA-IR), 24 use of insulin therapy and use of angiotensin-converting enzyme (ACE) inhibitors or other renin angiotensin aldosterone system (RAAS)-modifying medication, all determined as previously described.12,13
Statistical analysis
All analyses were performed with the statistical software package SPSS version 21.0 (SPSS IBM Corporation, Armonk, NY, USA). Descriptive statistics are presented as means ± standard deviations, or in case of a skewed distribution as median (interquartile range), or frequencies (percentages). Variables with a skewed distribution (i.e. CML, CEL, pentosidine, triglycerides, LA volume index, LA volume × LVMI product term) were log-transformed in order to meet normality criteria. For reasons of direct comparison, the individual AGEs Z-scores [individual value − population mean)/(population standard deviation] were calculated for CML, CEL and pentosidine. For descriptive purposes and legibility, LA volume index and LA volume × LVMI product term values were multiplied by −1 so that lower values indicate worse diastolic function.
We used linear regression analyses to investigate the associations between Z-scores of AGEs and LV structure and function. Adjustments were made first for age and sex (model 1). The results were then additionally adjusted prior to CVD, hypertension and/or the use of anti-hypertensive medication, total cholesterol–high-density lipoprotein cholesterol ratio, triglycerides, the use of lipid-modifying medication, current smoking, eGFR and waist circumference (model 2). Initial analyses showed a statistically significant interaction between AGEs and GMS in their association with LV function, and therefore, the analyses were stratified according to GMS. p < 0.05 was considered statistically significant, except for the interaction analyses, where p < 0.10 was used.
Results
Study population
For the present analyses, individuals were excluded with missing data on serum AGEs (n = 73), GMS (n = 5) or other covariates (n = 54). In the remaining 704 individuals, full data to determine LV dimension, LV systolic function and LV diastolic function were available in 693, 649 and 672 individuals, respectively. The final study population (n = 693) consisted of 280 individuals with NGM, 171 with IGM and 242 with T2DM. Individuals with missing data more frequently had diabetes and hypertension, had a higher waist circumference and higher levels of triglycerides (data not shown).
Characteristics
The characteristics of the study population stratified according to tertiles of diastolic function (i.e. tertiles of LA volume index) are given in Tables 1 and 2. With deteriorating diastolic function, participants were, in general, older, suffered more frequently from hypertension and used more anti-hypertensive medication (including ACE inhibitors). In addition, these participants more often had T2DM, prior CVD, albuminuria and lower low-density lipoprotein (LDL) cholesterol levels.
Characteristics of the study population according to tertiles of LA volume index (n = 672).
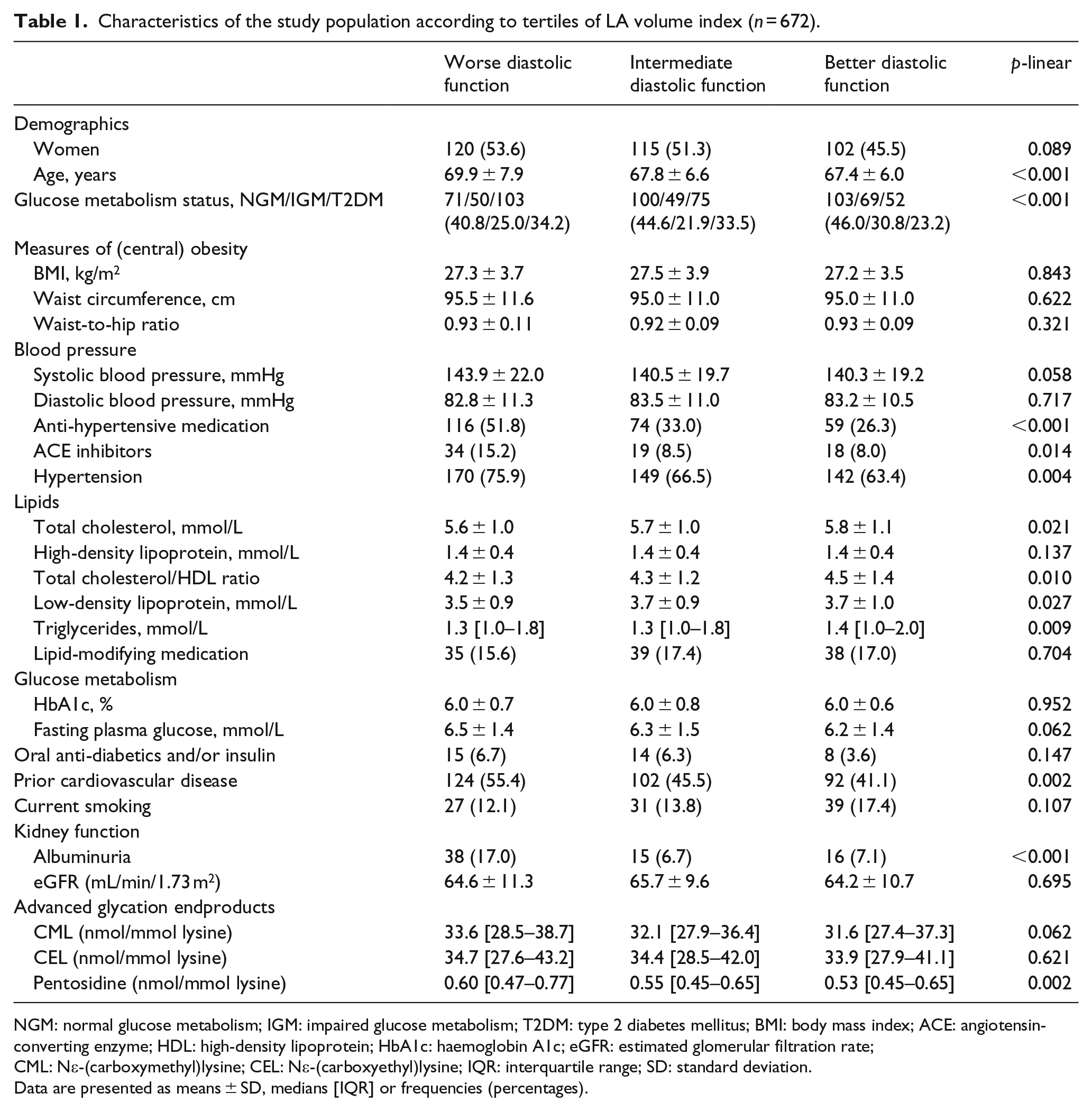
NGM: normal glucose metabolism; IGM: impaired glucose metabolism; T2DM: type 2 diabetes mellitus; BMI: body mass index; ACE: angiotensin-converting enzyme; HDL: high-density lipoprotein; HbA1c: haemoglobin A1c; eGFR: estimated glomerular filtration rate; CML: Nε-(carboxymethyl)lysine; CEL: Nε-(carboxyethyl)lysine; IQR: interquartile range; SD: standard deviation.
Data are presented as means ± SD, medians [IQR] or frequencies (percentages).
Echocardiographic indices of the study population according to tertiles of LA volume index (n = 672).
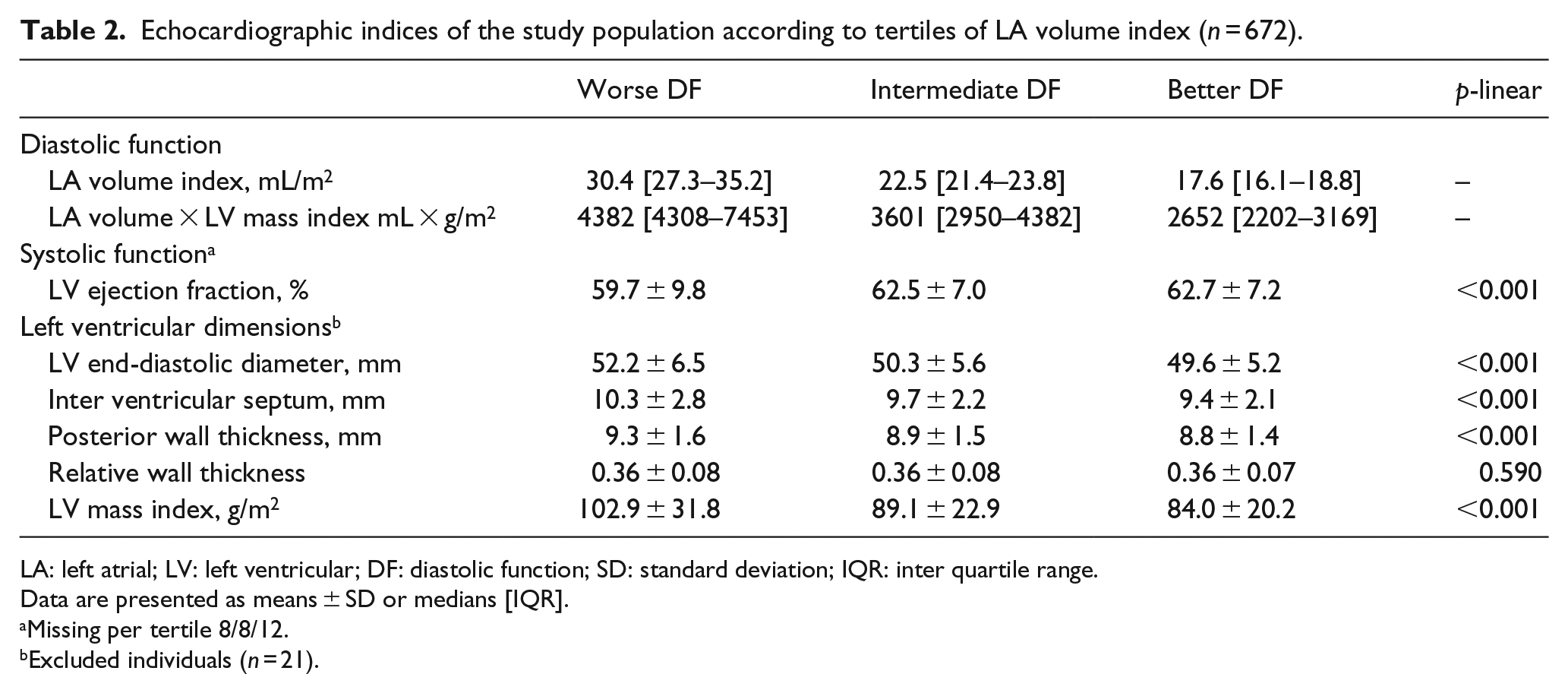
LA: left atrial; LV: left ventricular; DF: diastolic function; SD: standard deviation; IQR: inter quartile range.
Data are presented as means ± SD or medians [IQR].
Missing per tertile 8/8/12.
Excluded individuals (n = 21).
With deteriorating diastolic function, serum pentosidine increased (p for linear trend 0.002), whereas no linear trend was observed with serum CML and CEL (p = 0.062 and p = 0.621, respectively) (Table 1). These associations were not materially altered after additional adjustment for age and/or waist circumference 25 (data not shown). Deteriorating diastolic function was associated with lower systolic function, greater LV end-diastolic diameter, increased wall thicknesses and a greater LVMI (p for linear trend all <0.001) (Table 2).
Associations of AGEs with diastolic function
After adjustment for the variables of model 2, higher levels of the Z-score of serum CML were, in NGM, associated with worse diastolic function. The regression coefficients [beta (95% confidence interval (CI))] for LA volume index and the LA volume × LVMI product term were −0.053 (−0.095; −0.011) and −0.064 (−0.126; −0.002), respectively. In IGM and T2DM, no significant associations were observed with both indices of diastolic function. The p-values for interaction between GMS and the Z-score of CML were 0.011 and 0.035 for the LA volume index and the LA volume × LVMI product term, respectively.
After adjustment for the variables of model 2, higher levels of the Z-score of serum pentosidine were, in NGM, associated with worse diastolic function in both indices (i.e. LA volume index and the LA volume × LVMI product term): −0.056 (−0.099; −0.013) and −0.084 (−0.417; −0.021), respectively. In IGM, lower levels of the Z-score of pentosidine were associated with lower levels of the LA volume × LVMI product term only: −0.080 (−0.164; 0.003). In T2DM, no significant associations could be observed between the Z-score of pentosidine and diastolic function. The p-values for interaction between GMS and Z-score of pentosidine were 0.040 and 0.085 for the LA volume index and the LA volume × LVMI product term, respectively.
Neither in NGM nor in IGM or in T2DM was the Z-score of serum CEL associated with diastolic function. The p-values for interaction between GMS and Z-score of CEL were 0.320 and 0.390 for the LA volume index and the LA volume × LVMI product term, respectively. (Table 3, Supplemental Figure 1(a)).
Associations of Z-score of serum AGEs with diastolic function (n = 672) and systolic function (n = 649) according to glucose metabolism status.
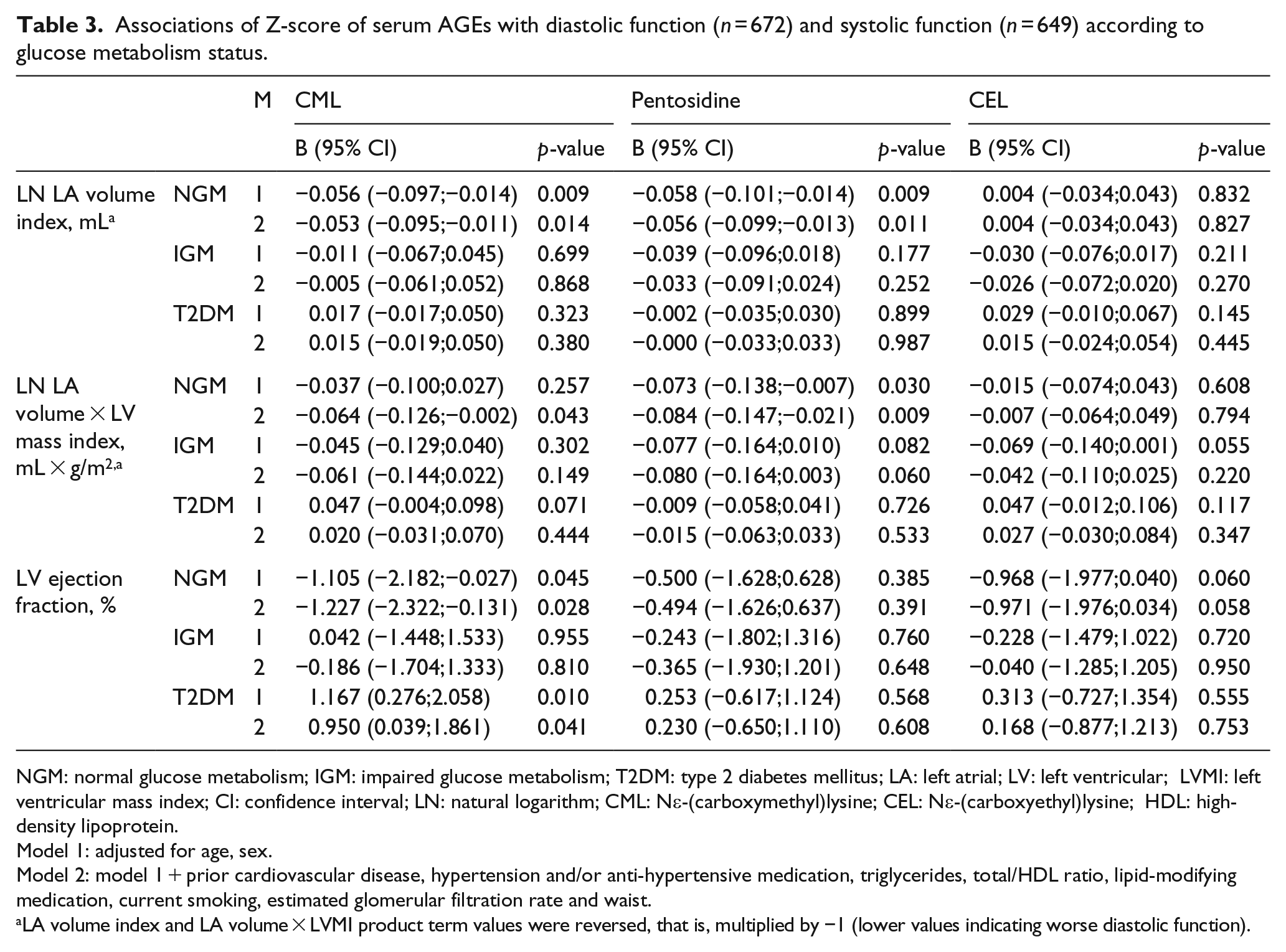
NGM: normal glucose metabolism; IGM: impaired glucose metabolism; T2DM: type 2 diabetes mellitus; LA: left atrial; LV: left ventricular; LVMI: left ventricular mass index; CI: confidence interval; LN: natural logarithm; CML: Nε-(carboxymethyl)lysine; CEL: Nε-(carboxyethyl)lysine; HDL: high-density lipoprotein.
Model 1: adjusted for age, sex.
Model 2: model 1 + prior cardiovascular disease, hypertension and/or anti-hypertensive medication, triglycerides, total/HDL ratio, lipid-modifying medication, current smoking, estimated glomerular filtration rate and waist.
LA volume index and LA volume × LVMI product term values were reversed, that is, multiplied by −1 (lower values indicating worse diastolic function).
Associations of AGEs with systolic function
After adjustment for the variables of model 2, higher levels of the Z-score of serum CML were, in NGM, associated with lower LV ejection fraction [−1.227 (−2.322; −0.131)]. In IGM, no significant association could be observed; whereas in T2DM, higher levels of the Z-score of CML were associated with higher LV ejection fraction [0.950 (0.039; 1.861)]. The p-value for interaction between GMS and Z-score of CML for LV ejection fraction was 0.002. Neither in NGM nor in IGM or in T2DM was the Z-score of serum pentosidine associated with LV ejection fraction. The p-value for interaction between GMS and Z-score of pentosidine for LV ejection fraction was 0.316.
Higher levels of Z-score of serum CEL were associated with lower LV ejection fraction [−0.971 (−1.976; 0.034)] in NGM only. The p-value for interaction between GMS and Z-score of CEL for LV ejection fraction was 0.218 (Table 3 and Supplemental Figure 1(b)).
Associations of AGEs with LV structure
None of the serum Z-scores of the individual AGEs were associated with any of the individual indices of LV structure (Supplemental Table 1). No significant interaction between GMS and individual Z-scores of AGEs for the individual indices of LV structure were observed (data not shown).
Additional analyses
When the statistical analyses were repeated on those with full echocardiographic data (n = 644), the results did not materially change (data not shown). If we replaced waist circumference by either waist-to-hip ratio or body mass index, the results did not materially change (data not shown). Additional adjustments for insulin resistance, insulin therapy, RAAS-modifying agents or ACE inhibitors specifically did not materially change the results (data not shown).
Discussion
This study is the first large population-based cohort study, stratified according to GMS, that investigated the association between the protein-bound serum AGEs, CML, pentosidine and CEL on the one hand and LV function and structure as determined by echocardiography on the other.
The results showed that, in NGM only, higher levels of CML and pentosidine were associated with worse diastolic function. In IGM, higher levels of pentosidine were borderline and significantly associated with worse diastolic function; whereas in T2DM, none of the serum AGEs were associated with diastolic function. With regard to systolic function, in NGM, higher levels of CML and CEL were associated with worse systolic function. In IGM, no associations were observed; whereas in T2DM, higher levels of CML were associated with better systolic function. Finally, none of the serum AGEs were individually related to any of the individual indices of LV structure.
The results of this study extend previous knowledge by adding population-based data and by showing that serum AGEs are indeed associated with both impaired diastolic and systolic LV function in individuals with NGM, and thus may contribute to the pathobiology of heart failure. Such associations were, however, not observed, quite unexpectedly, in individuals with IGM or T2DM.
Interestingly, similar observations were made by Campbell et al. 7 in patients undergoing coronary bypass surgery and by Berg et al. 8 in individuals with type 1 diabetes. In the former study, the association between higher levels of circulating CML and diastolic dysfunction became stronger after exclusion of individuals with diabetes; 7 whereas in the latter, higher levels of circulating CML were associated with better systolic function in individuals with diabetes. 8
The above suggests that the associations between circulating AGEs and LV function and structure are not straightforward. Studies conducted on human7,26–32 or animal33–38 cardiac tissue have shown that AGEs accumulate within the myocardium,7,26–34 even more so in T2DM26–31,34 or IGM. 33 In addition, these studies showed that the myocardial accumulation of AGEs was associated with impaired diastolic function30,33–36 and/or impaired systolic function.36–38 The contrasting results of our study, where we measured circulating AGEs is the observation that they were not associated with LV function with deteriorating GMS and thereby calls into question whether circulating AGEs in IGM and T2DM may be representative of the accumulation of AGEs within the myocardium.
For example, it has been shown that, with increasing levels of obesity, CML becomes increasingly trapped in visceral adipose tissue, which was accompanied by lower levels of circulating CML and greater insulin resistance. 25 In the present study, however, adjustment for measures of obesity did not affect the results. Alternatively, it has been suggested that collagen, due to cross-linkage by AGEs, is less vulnerable to enzymatic degradation, and thereby traps AGEs in the extracellular matrix. 39 In addition, we cannot fully exclude the possibility that survival bias might have influenced our results to such an extent that the reported associations between circulating AGEs and LV function are underestimated, in particular, in individuals with IGM or T2DM, because of their increased cardiovascular mortality risk. In sum, a straightforward pathobiological explanation for the results of the present study and the studies by Campbell et al. 7 and Berg et al. 8 with respect to IGM and T2DM is not readily at hand, and this issue requires further study.
Nevertheless and regardless of how circulating AGEs may be (pathobiologically) handled with deteriorating GMS, an important role for AGEs in the pathobiology of heart failure can still be deducted from the fact that in ageing individuals with NGM, the risk of heart failure parallels the accumulation of AGEs.2,40,41
Other limitations of this study may be its cross-sectional design, which does not allow strong causal inferences. In addition, the criteria to define diastolic function have changed considerably over the years. Nevertheless, LA volume index and the LA volume × LVMI product term have been shown to be reliable proxy measurements for chronic diastolic function.19,20
In conclusion, in this population-based cohort study, in NGM, both higher levels of serum CML and pentosidine were associated with worse diastolic function, and higher levels of CML and CEL were associated with worse systolic function. In IGM, a similar pattern emerged, though less consistent; whereas in T2DM, these associations were either non-existent or even reversed. The results of this study thereby suggests that serum AGEs are associated with impaired LV function in individuals with NGM but that in individuals with deteriorating GMS serum AGEs may not mirror heart failure risk.
Footnotes
Declaration of conflicting interests
P. Linssen, C. Schalkwijk, J. Dekker, G. Nijpels and C. Stehouwer have nothing to disclose. R. Henry reports grants and personal fees from Sanofi, outside the submitted work. HP. Brunner-La Rocca reports grants and personal fees from Roche Diagnostics, grants from AstraZeneca, grants from GSK and personal fees from Novartis, outside the submitted work.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.