
Abstract
Blood pressure variability is associated with macrovascular complications and stroke, but its association with the microcirculation in type II diabetes has not been assessed. This study aimed to determine the relationship between blood pressure variability indices and retinal arteriolar diameter in non-diabetic and type II diabetes participants. Digitized retinal images were analysed to quantify arteriolar diameters in 35 non-diabetic (aged 52 ± 11 years; 49% male) and 28 type II diabetes (aged 61 ± 9 years; 50% male) participants. Blood pressure variability was derived from 24-h ambulatory blood pressure. Arteriolar diameter was positively associated with daytime rate of systolic blood pressure variation (p = 0.04) among type II diabetes participants and negatively among non-diabetics (p = 0.008; interaction p = 0.001). This finding was maintained after adjusting for age, sex, body mass index and mean daytime systolic blood pressure. These findings suggest that the blood pressure variability–related mechanisms underlying retinal vascular disease may differ between people with and without type II diabetes.
Introduction
Quantitative measures of retinal vascular structure, such as vessel diameters, may provide prognostic information regarding microvascular complications and risk related to vascular diseases such as type II diabetes (T2DM). Retinal microvascular changes have been related to hypertension, 1 while changes in retinal arteriolar diameters could be an early pathophysiological indicator in T2DM. 2 Although narrower retinal arteriolar diameters have been found to be associated with high blood pressure (BP), 3 possibly indicating vasoconstriction or inward remodelling in response to elevated BP, wider retinal arteriolar diameters were found to be associated with T2DM, 4 suggesting impaired arteriolar autoregulation 5 due to compromised myogenic responses. Negative correlations between BP and arteriolar diameters have also been observed in T2DM, 6 but evidence suggests that these relationships may be weaker than in non-diabetic individuals. 7
On the other hand, blood pressure variability (BPV) indices, such as the rate of BP variation over time (a measure of the speed of BP change), is thought to be an indication of the alterations in cardiovascular regulatory mechanisms that could lead to vascular complications irrespective of the mean (average) BP level. 8 At the same time, increased arterial stiffness and autonomic dysregulation, which could both lead to increased BPV, are common complications in T2DM.9,10 Nevertheless, the relevance of BPV or mean BP level to retinal arteriolar diameters as derived from 24-h ambulatory BP has never been investigated in individuals with T2DM. The aim of this study was to examine the relationship between mean BP levels and BPV with arteriolar diameters, in individuals with T2DM. We hypothesized that BPV indices may play a role in retinal vascular structure, as assessed by the quantification of arteriolar diameter, in patients with T2DM.
Methods
Data from this study were derived from a previously published investigation among 80 consecutive participants with (n = 40) and without T2DM (n = 40) recruited from the local community. 11 This current post-hoc, hypothesis-generating analysis was from the 35 non-diabetic and 28 T2DM participants where both retinal imaging and 24-h ambulatory BP measurements were available. Exclusion criteria included pregnancy, arrhythmia or a clinical history of cardiovascular disease (including coronary artery disease, myocardial infarction, heart failure or stroke) or severe pulmonary disease. T2DM was self-reported after diagnosis by a doctor. The Human Research Ethics Committee of the University of Tasmania approved the study and written informed consent was provided by all participants.
Retinal imaging
Retinal images were recorded using a non-mydriatic retinal camera (Canon, CR-DGi-45NM) and digitized to a resolution of 2800–2400 pixels using a LS100 slide scanner (Nikon, Tokyo, Japan). Microvascular parameters were measured using a custom written MATLAB program, as described previously. 12 Good reproducibility of this technique has been previously reported. 12 The analysis was performed on a series of complete vascular branches, either from one eye or from both eyes in order to obtain the required number of vessel segments (8, range: 7–18) and bifurcations (6, range: 3–15). Arteriolar diameter was measured in a series of intensity cross-sections normal to the vessel at two-pixel intervals along the entire length of the vessel segment. At each cross-section, arteriolar diameter was measured to subpixel accuracy using a sliding linear regression filter technique as described previously 12 and the average was calculated for each vessel.
24-h ambulatory BP and BPV indices
The 24-h ambulatory BP was measured every 20 min during the daytime and every 30 min during the night-time (TM-2430; A&D Medical, Sydney, Australia). Participants were asked to continue their usual daily activities but to avoid any strenuous activities. Individual measurements with an error code or those with a pulse pressure of less than 20 mmHg were excluded from the analysis. BPV was expressed separately for the periods of daytime, night-time and 24-h as the rate of BP variation and was calculated based on a modified method described by Zakopoulos et al. 13 Rate of BP variation was further adjusted for the corresponding mean BP levels [(rate of BP variation/mean BP) × 100]. Calculations involved plotting the slope for the change between systolic blood pressure (SBP) and diastolic blood pressure (DBP) readings against time. Daytime was defined as the period between 08:00 and 20:00 and night-time as the period between 22:00 and 06:00. The periods from 20:00 to 22:00 and 06:00 to 08:00 were excluded as they represent the steepest diurnal fall and rise in BP, respectively, and, therefore may contribute to BPV measures. BPV was also quantified using the coefficient of variation (CV) of the corresponding mean BP level [(standard deviation/mean BP) × 100].
Blood biochemistry
Venous blood samples were drawn from the antecubital fossa, and analytical biochemistry was performed by the Royal Hobart Hospital pathology department using accredited laboratory techniques.
Statistical analysis
Student’s t tests were used to compare retinal and haemodynamic variables between diabetic and non-diabetic participants. Linear regression analysis was performed to assess the relationship between arteriolar diameter and BP measures, further statistical adjustment for possible confounders: age, sex, body mass index (BMI; and mean SBP for BPV) was performed by multivariable linear regression. Statistical interactions between diabetes status and BP variables were assessed by testing the statistical significance of the coefficient of a product term after adjusting for age, BMI, sex, and mean daytime SBP (diabetes status × BP variable). A p value of <0.05 was considered statistically significant. All data were analysed using Stata 12.1 (StataCorp, College Station, TX, USA).
Results
Participants with T2DM were older, had higher BMI, and most were on antihypertensive therapy or treatment with statins in comparison with non-diabetic participants (Supplementary Table 1). The 24-h ambulatory mean BP and BPV indices were similar between the groups (Supplementary Table 1) and there were no differences in arteriolar diameters [non-diabetics; 25.54(2.74) pixels vs T2DM; 25.58(2.71) pixels, p = 0.96].
In univariate regression analysis, arteriolar diameter was associated positively with daytime rate of SBP variation among participants with T2DM (β = 0.007; p = 0.04; R2 = 0.12) and negatively among non-diabetics (β = −0.010; p = 0.008; R2 = 0.17). Additionally, mean daytime SBP was negatively associated with arteriolar diameter among participants with T2DM (β = −0.003; p = 0.03, R2 = 0.16) but not among non-diabetics (β = 0.0003; p = 0.80). A significant interaction between diabetes status and daytime rate of SBP variation was observed and remained significant after adjusting for age, sex, BMI, and mean daytime SBP (β = 0.02; p = 0.001; Figure 1). Similar associations were observed when BPV was quantified as the CV (interaction p = 0.038).
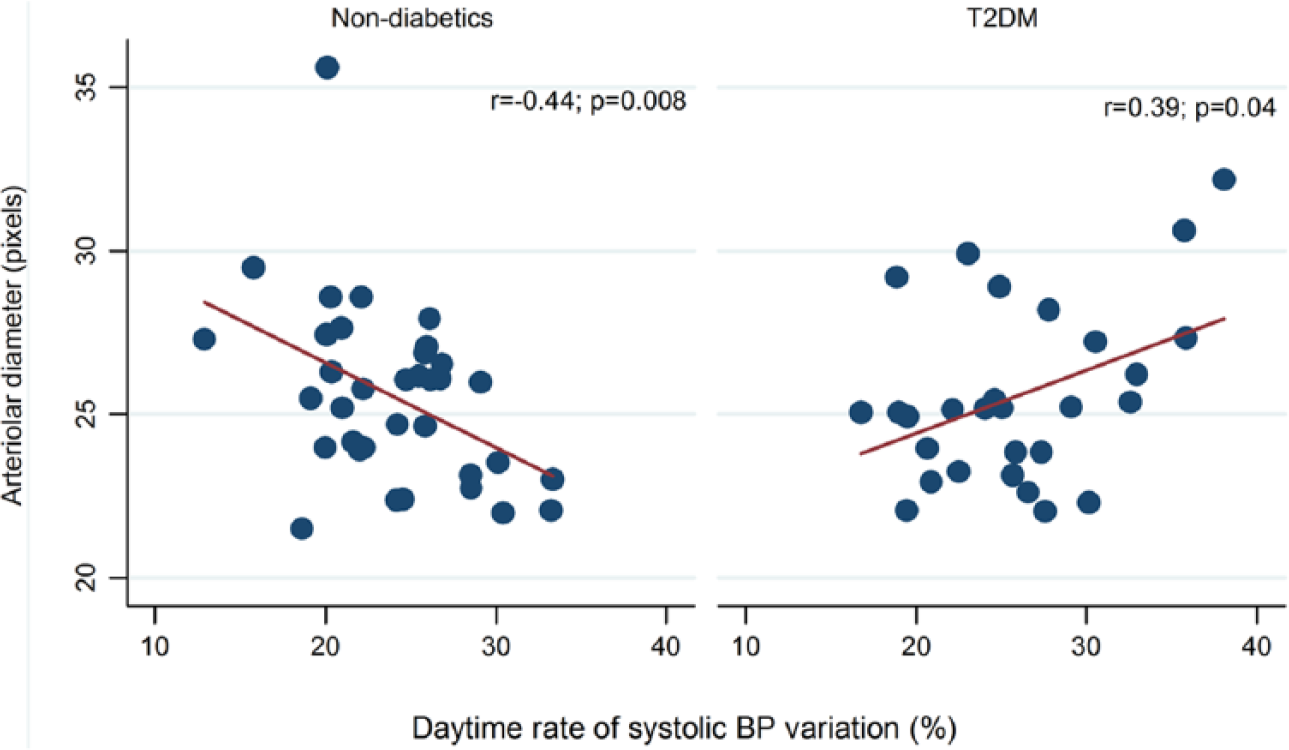
Scatter plots and fitted regression lines of the relationship between arteriolar diameter and daytime rate of systolic BP variation among non-diabetics and participants with T2DM.
Discussion
The main finding of this study was that there were significantly different associations between retinal arteriolar diameter and BPV indices among healthy individuals and participants with T2DM. Retinal arteriolar diameter was positively associated with daytime SBP variation among participants with T2DM but negatively among non-diabetic individuals.
These findings may suggest different pathophysiological contributions of BPV to adverse retinal arteriolar outcomes among people with T2DM compared with non-diabetic controls.
BPV could play a role in large artery damage and remodelling over and above mean BP levels; however, despite its importance in cardiovascular disease and stroke in particular, 8 the role of BPV in microvascular disease is still unclear. This is the first study to assess the relationship between BPV and retinal arteriolar diameter and the impact of T2DM on that relationship.
Our findings of a positive relationship between BPV and retinal arteriolar diameter in participants with T2DM could be relevant to the mechanism or consequences of increased BPV. Arteriolar dilatation in association with higher BPV in T2DM could be an early sign of impaired vascular autoregulation 5 or early autonomic neuropathy. 10 Both are associated with increased risk of retinal microvascular damage that could result from exaggerated fluctuation in transmitted pressure or flow to the microcirculation. However, these results should be seen in the context of the limitations of this study; the small sample size and the cross-sectional design which limit the interpretation of the findings.
In conclusion, the findings suggest that increased BP fluctuations may be associated with different arteriolar responses in comparison with elevated mean BP levels, with BPV possibly playing a role in the pathophysiology of retinal microvasculature in T2DM. Although the mechanisms underlying the relationship between BPV and retinal arteriolar in T2DM remain unclear, our findings support the need for further investigation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.