
Abstract
Objective:
To assess the impact of intermediate-term treatment with rosiglitazone on high-sensitivity cardiac troponin T levels among patients with type 2 diabetes mellitus with or at high risk of coronary artery disease.
Methods:
High-sensitivity cardiac troponin T level was measured at baseline and after 6 months of study treatment in a randomized trial comparing rosiglitazone versus placebo in patients with type 2 diabetes and prevalent cardiovascular disease or multiple cardiovascular disease risk factors. Univariable and multivariable linear regression analyses were performed to assess the effect of rosiglitazone versus placebo on high-sensitivity cardiac troponin T levels.
Results:
The study included 150 randomized participants, of whom 106 had paired baseline and end-of-study blood samples for analysis (mean age: 56 ± 8 years, 42% women; 8.8 years average type 2 diabetes duration; mean haemoglobin A1c of 7.5). Almost all study participants (93%) had detectable high-sensitivity cardiac troponin T (⩾3 ng/L) at baseline, including 23% with high-sensitivity cardiac troponin T levels exceeding the threshold commonly used to diagnose myocardial infarction (⩾14 ng/L). Change in high-sensitivity cardiac troponin T levels from baseline to follow-up was not significantly different between rosiglitazone and placebo groups (p = 0.316).
Conclusion:
Rosiglitazone did not impact high-sensitivity cardiac troponin T levels, adding to the growing body of literature suggesting that the incremental heart failure risk associated with rosiglitazone is not mediated by direct myocardial injury.
Introduction
The peroxisome proliferator-activated receptor gamma agonists, rosiglitazone and pioglitazone, used for the treatment of type 2 diabetes, are associated with an increased risk of incident or worsening heart failure (HF). US product labels provide cautions for both medications in patients with any HF and contraindications for initiation in patients with Class III or IV HF. 1 While uncertainty remains regarding the mechanism underpinning the HF effects, most data suggest plasma volume expansion caused by these medications, without evidence of adverse effects on cardiac structure or function.2–4
The development of high sensitive assays for measurement of high-sensitivity cardiac troponin T (hscTnT) and I, and demonstration in numerous studies of the association between small elevations in troponin and subsequent cardiovascular (CV) events, specifically incident or worsening HF, provides a powerful new tool for screening for subclinical cardiac injury.5,6 On this backdrop, we assessed the prevalence of detectable circulating hscTnT in patients with type 2 diabetes with or at high risk of atherosclerotic vascular disease and the impact of 6 months of rosiglitazone versus placebo on hscTnT levels.
Methods
Study design and population
Data and blood samples were analysed from a single-centre, prospective, double-blind, randomized, parallel group, placebo-controlled trial designed primarily to assess the effects of rosiglitazone on integrated CV performance and cardiac structure and function among patients with type 2 diabetes and cardiovascular disease (CVD) or at increased risk of CVD, with the trial design and primary results previously published.3,7 Inclusion criteria included participants with medically treated type 2 diabetes with either prevalent atherosclerotic CVD or at least one additional CVD risk factor: smoking, hypertension, hypercholesterolaemia, albuminuria, family history of premature coronary disease or documented C-reactive protein >3 mg/L. Exclusion criteria included prior thiazolidinedione (TZD) treatment, prior HF or liver function test >3× upper limit of normal. All participants provided written informed consent to a protocol approved by University of Texas Southwestern Medical Center institutional review board.
Participants were randomized 1:1 to 6 months of blinded treatment with rosiglitazone or placebo added to existing glucose-lowering therapy, initiated at 4 mg daily of rosiglitazone or matching placebo, and titrated at 1 month to rosiglitazone 8 mg daily or matching placebo for the remainder of the study. Glycosylated haemoglobin A1c (HbA1c) was measured at baseline, monthly for the first 3 months, and at the final study visit at 6 months. Open-label non-TZD glucose-lowering treatment was titrated targeting A1c < 7.0% in both arms throughout the trial, in accordance with contemporaneous American Diabetes Association guidelines. 8
All participants underwent cardiopulmonary exercise testing at baseline and after 6 months of study treatment with peak measured oxygen consumption scaled to fat-free mass (FFM; VO2peak; mL/kg-FFM/min). In addition, a subgroup of participants (n = 75) volunteered to participate in a cardiac magnetic resonance imaging (cMRI) substudy, 66 of whom had complete cMRI and hscTnT data for analyses. The exercise testing and cMRI protocols have been described previously.3,7
Measurements of biomarkers
At baseline and at the final study visit completing 6 months of study treatment, venous blood samples were collected into ethylenediaminetetraacetic acid (EDTA) tubes, stored immediately on ice, centrifuged within 4 h at 1430g for 15 min at 40°C, with plasma immediately stored at −70°C. HscTnT levels were measured on all samples following study completion using a highly sensitive automated immunoassay (Elecsys-2010 Troponin T hs STAT, Roche Diagnostics, Indianapolis, IN), with a limit of blank (LOB) of 3 ng/L, a limit of detection of 5 ng/L and a reported 99th percentile value in apparently healthy individuals of 14 ng/L. For purposes of these analyses, all hscTnT levels ⩾ LOB of 3 ng/L were considered detectable.
Statistical analysis
For primary analyses, all trial participants were stratified into two groups based on their baseline hscTnT levels, with secondary analyses further stratifying those with detectable hscTnT into those with or without levels ⩾14 ng/L, the value established for diagnosis of myocardial infarction (MI) for patients with acute coronary syndromes, using univariable and multivariable logistic regression. Results are presented as the mean ± standard deviation (SD) for continuous normally distributed variables, median (interquartile range) for non-normally distributed data and proportions for categorical data. Continuous data were analysed using Student’s t-test or the Wilcoxon rank-sum test as appropriate. Categorical data were analysed across groups using Pearson’s chi-squared test. Primary outcome of the study was continuous change in hscTnT from baseline to end of study, which was compared within and across the two treatment groups using the Wilcoxon rank-sum test. A two-sided p < 0.05 was considered statistically significant, with no adjustment made for multiple comparisons. Statistical analyses were performed using SAS software, version 9.2 (SAS Institute; Cary, NC).
Step-wise logistic regression with backward selection was used to identify participant characteristics independently associated with a significantly elevated hscTnT level (⩾14 ng/L) at baseline as well as to identify predictors of increase in troponin (>0 ng/L) over the 6-month study period. Candidate variables analysed for hscTnT ⩾ 14 ng/L at baseline included age, sex, body mass index, prevalent CVD, duration of type 2 diabetes, renal function assessed as estimated glomerular filtration rate, hypertension, insulin use, treatment arm (rosiglitazone vs placebo), A1c, baseline peak oxygen consumption (VO2peak) and N-terminal pro-brain natriuretic protein (NT-proBNP). Furthermore, measures of left ventricular (LV) structure and function (ejection fraction and LV mass) were included as additional covariables in the aforementioned logistic regression analyses, restricted to the subgroup of participants who underwent cardiac MRI.
Results
The study included 150 participants, of whom 106 had paired baseline and end-of-study blood samples for analysis (53 placebo, 53 rosiglitazone, mean age: 56 ± 8 years, 42% women; 8.8 years average type 2 diabetes duration; 42% insulin treated). In all, 93% of study participants had detectable hscTnT levels (⩾3 ng/L) at baseline, of which 23% had levels ⩾14 ng/L. We observed significant differences in the demographic and clinical characteristics of the study participants with versus without detectable troponin levels at baseline (Table 1). Compared with participants without detectable hscTnT (<3 ng/L), those with detectable troponin levels were more likely to be men, had more prevalent comorbidities including CV risk factors and lower fitness levels (Table 1). Use of medications such as statins and hypoglycaemic agents (insulin, sulfonylureas) was higher in participants with detectable hscTnT levels. These differences were more pronounced among the subgroup of participants with hscTnT levels beyond the 99th percentile cut-off for MI (⩾14 ng/L).
Demographic and cardiometabolic characteristics of study population.
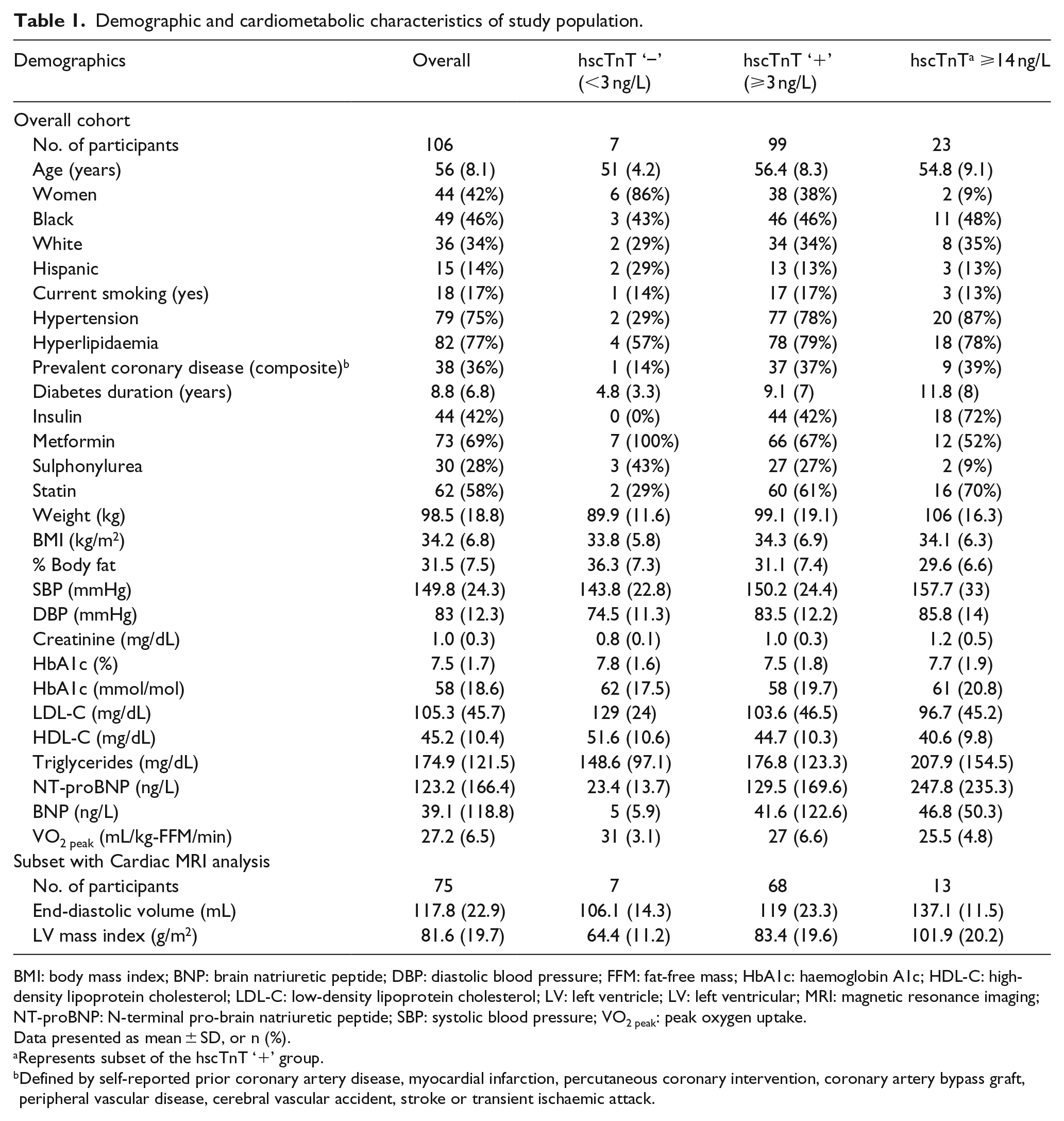
BMI: body mass index; BNP: brain natriuretic peptide; DBP: diastolic blood pressure; FFM: fat-free mass; HbA1c: haemoglobin A1c; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; LV: left ventricle; LV: left ventricular; MRI: magnetic resonance imaging; NT-proBNP: N-terminal pro-brain natriuretic peptide; SBP: systolic blood pressure; VO2 peak: peak oxygen uptake.
Data presented as mean ± SD, or n (%).
Represents subset of the hscTnT ‘+’ group.
Defined by self-reported prior coronary artery disease, myocardial infarction, percutaneous coronary intervention, coronary artery bypass graft, peripheral vascular disease, cerebral vascular accident, stroke or transient ischaemic attack.
There were statistically significant increases in median hscTnT levels from baseline to end-of-study in both the placebo (8.1–9.0 ng/L; p < 0.0001) and in the rosiglitazone groups (9.9 vs 10.4 ng/L; p = 0.003; Figure 1). However, the change in hscTnT levels from baseline to follow-up was not significantly different between the two groups (p = 0.316). Similarly, the proportion of participants who increased their troponin levels (>0 ng/L) was not statistically different between controls versus rosiglitazone groups (75% vs 64%; p = 0.20).
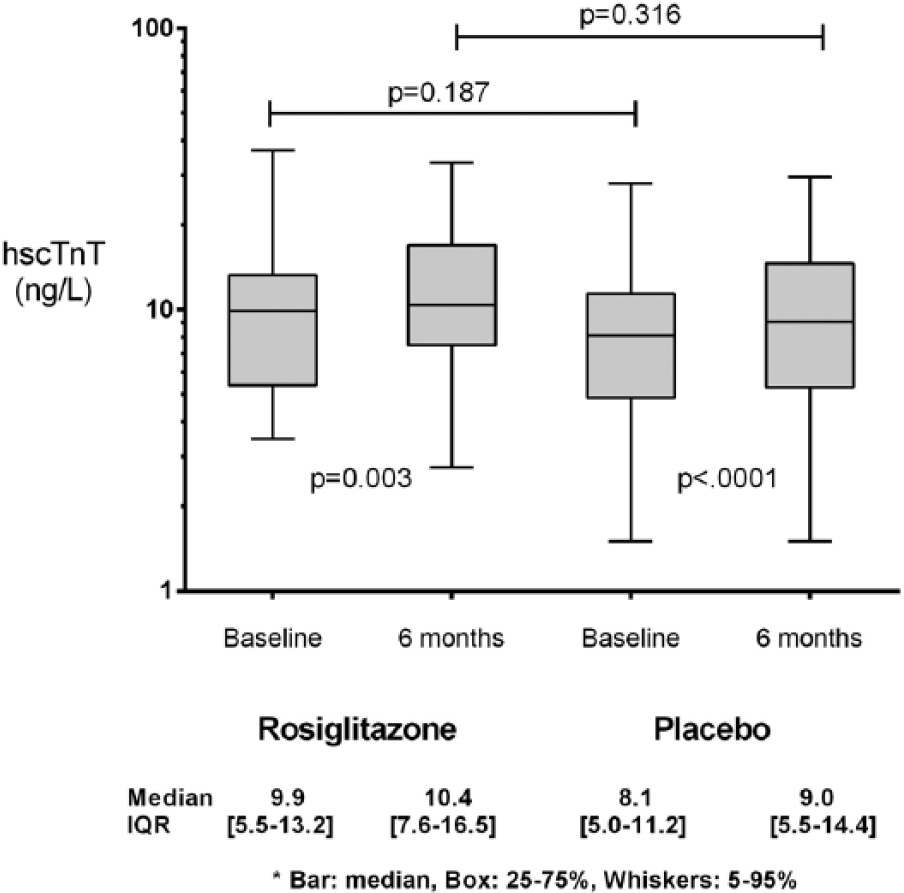
High-sensitive cardiac troponin T levels at baseline and follow-up among the rosiglitazone and placebo groups.
In multivariable adjusted logistic regression analyses, we identified male sex (p = 0.006), NT-proBNP (p = 0.008), LV mass (p = 0.002) and insulin use (p = 0.02) as independent predictors of significantly elevated baseline hscTnT levels (⩾14 ng/L). Furthermore, prevalent CVD (p = 0.04) and baseline A1c (p = 0.03) were independently associated with increase in hscTnT over the 6-month study follow-up (Table 2). In multivariable analyses, rosiglitazone use was not associated with end-of-study hscTnT levels or change in hscTnT from baseline to 6-month follow-up.
Multivariable adjusted logistic regression analysis to determine predictors of baseline high troponin and increase in troponin from baseline to follow-up.
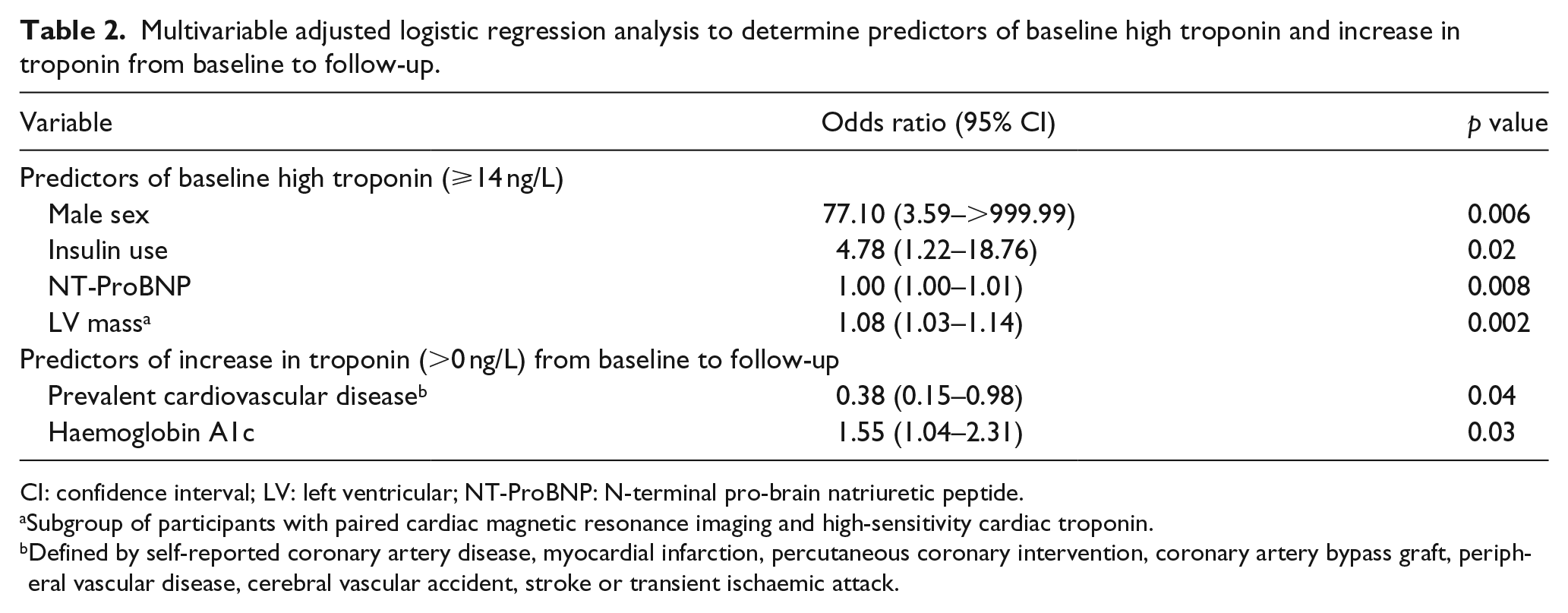
CI: confidence interval; LV: left ventricular; NT-ProBNP: N-terminal pro-brain natriuretic peptide.
Subgroup of participants with paired cardiac magnetic resonance imaging and high-sensitivity cardiac troponin.
Defined by self-reported coronary artery disease, myocardial infarction, percutaneous coronary intervention, coronary artery bypass graft, peripheral vascular disease, cerebral vascular accident, stroke or transient ischaemic attack.
Discussion
We observed two important findings in this study. First, an extremely high proportion of patients with type 2 diabetes had hscTnT levels ⩾ LOB (3 ng/L) with a significant percentage having hscTnT levels exceeding the 99th percentile of normal controls, a threshold used in the clinical setting of acute coronary syndromes to diagnose MI. Second, rosiglitazone compared with placebo is not associated with higher hscTnT levels after 6 months of study treatment.
The proportion of our study cohort of stable ambulatory patients with type 2 diabetes who had hscTnT ⩾ LOB was significantly greater than that reported in previous population-based studies, most likely attributable to the enrichment criteria for this study requiring prevalent CVD or clustered CVD risk factors, relatively advanced age of this clinical cohort and long duration of diabetes on average.9–12 These findings represent a high burden of chronic subclinical myocardial injury and greater risk of adverse CV outcomes among patients with diabetes and risk factors for CVD.10,11,13 Furthermore, the proportion of patients with hscTnT levels above the 99th percentile cut-off for MI was also notably high in this study, of clinical importance as this could confound diagnosis of MI in up to one-quarter of such patients if the hscTnT assay is used.14,15
TZDs have been associated with adverse outcomes such as an increased risk of new or worsening peripheral oedema with incidence ranging 2.5%–16.3% and based on published meta-analysis, 1.3- to 2.2-fold increased risk of incident HF with pioglitazone and rosiglitazone, respectively.1,16–20 Furthermore, evidence from at least one animal model suggests accelerated apoptosis and cardiac toxicity with rosiglitazone, proposed to be mediated by reactive oxygen species. 21 As a result, the risk of incident or worsening HF with rosiglitazone has been a matter of significant concern and debate.1,22,23 In 2010, adjudicated results of the Rosiglitazone Evaluated for Cardiac Outcomes and Regulation of Glycaemia in Diabetes (RECORD) study, a randomized controlled trial comparing rosiglitazone to placebo in over 4500 participants with a median follow-up of 5.5 years, showed an increased risk of HF events (hazard ratio, HR (95% confidence interval, CI): 2.1 (1.35–3.27)) in the rosiglitazone arm. 24 However, other randomized control trials with intermediate-term follow-up (up to 1 year) have failed to demonstrate a significant deterioration in systolic or diastolic LV function with use of rosiglitazone as compared to placebo,25,26 including the previously published results from the MRI substudy of the present trial with no significant change in cardiac function or integrated cardiopulmonary performance. 3 However, it is plausible that rosiglitazone could cause subclinical myocardial injury which may not be detectable with imaging studies but may manifest as clinical HF on long-term follow-up. Importantly, however, no such signal was detected in this study, the first randomized trial to evaluate the effect of rosiglitazone on a sensitive marker of myocardial injury.
With the emergence of high-sensitive cardiac troponin assays, very low concentrations of troponin previously below the threshold of detection by conventional assay are now measurable. The hscTnT assay has been established as a useful tool in evaluating risk of incident HF or adverse CV outcomes. HscTnT and hscTnI have been evaluated in retrospective studies and found useful in surveillance of cardiac sarcoidosis activity and a biomarker for ruling out acute rejection in cardiac transplant recipients.27,28 In this study, we used hscTnT as a biomarker for subclinical myocardial injury to determine whether 6 months of treatment with rosiglitazone causes an increase in levels when compared to a placebo. We observed that despite an increase in hscTnT levels from baseline to follow-up, there was no difference between the rosiglitazone and placebo group, suggesting that use of rosiglitazone is not associated with any significant increase in myocardial injury.
There are a number of potential limitations. First, the sample size of our study is relatively small and the possibility of type 2 error cannot be ruled out. Nevertheless, we had ⩾80% power to detect a difference in 6-month hscTnT levels as small as 5.2 ng/L between groups. Second, the endpoint assessed was not part of the a priori hypothesis of the clinical trial. However, measurement of hscTnT was blinded to treatment assignment and outcomes assessment. Third, the study duration of 6 months precludes any long-term effects of rosiglitazone on hscTnT. Finally, interpretation of data is restricted to rosiglitazone and hence cannot be generalized to other TZD CV outcomes.
In conclusion, intermediate-term use of rosiglitazone in patients with diabetes mellitus and risk factors for CVD is not associated with an increase in hscTnT, a marker of subclinical myocardial injury.
Footnotes
Acknowledgements
We thank all the participants of the study as well as all staff member who collected the data.
Author contributions
U.I.S. and D.K.M. conceived and designed the study; helped to acquire, analyse and interpret the data; helped to draft the manuscript and revise the manuscript for important intellectual content; and approved the final version of the manuscript submitted. A.P. helped with data interpretation, manuscript preparation and important intellectual content. C.R.A. analysed the data and helped with data representation. R.S., I.J.N., O.G., B.G., S.M.A., A.K. and J.A.dL. helped to draft the manuscript and revise the manuscript for important intellectual content, and approved the final version of the manuscript submitted. D.K.M. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Declaration of conflicting interests
D.K.M. reports research grant from Novo Nordisk, AstraZeneca, Boehringer Ingelheim, Lexicon, GlaxoSmithKline, Takeda, Janssen, Eli Lilly, and Bristol Myers Squibb and consultancy fees from Takeda, Novo Nordisk, Janseen, Boehringer Ingelheim, Regeneron and Merck. J.A.dL. reports receiving research grants from Roche Diagnostics and Abbott diagnostics and consulting income from Abbott Diagnostics. All other authors have no financial relationships.
Funding
This work was supported by research grants from Glaxo Smith Kline, Roche Diagnostics, Inc., the Donald W. Reynolds Foundation and the National Center for Advancing Translational Sciences of the National Institutes of Health under award number UL1TR001105.