
Abstract
Purpose of the study:
To examine differences in the characteristics, treatment practices and in-hospital outcomes of patients with and without previously diagnosed diabetes hospitalized for non-ST segment elevation myocardial infarction.
Key methods:
The study cohort consisted of 3916 patients diagnosed with non-ST segment elevation myocardial infarction at all 11 central MA medical centres between 1999 and 2009, of whom 1475 (38%) had been previously diagnosed with diabetes.
Main results:
Diabetic patients were more likely to have received treatment with effective cardiac medications, and to have undergone coronary bypass surgery, but were less likely to have received a percutaneous coronary intervention, than non-diabetic patients. Patients with a history of diabetes were more likely to have developed cardiogenic shock, heart failure and died during their index hospitalization than non-diabetic patients.
Main conclusion:
Diabetic patients presenting with non-ST segment elevation myocardial infarction remain at high risk of developing significant clinical complications during hospitalization.
Introduction
Cardiovascular disease is the leading cause of morbidity and mortality among US adults. 1 In 2012, it was estimated that 29 million Americans had diabetes. 2 Adult men and women with diabetes are two to four times more likely to develop cardiovascular disease than adults without diabetes, and approximately two-thirds of adults with diabetes die from cardiovascular-related causes. 3
Multiple studies have documented a poorer prognosis associated with diabetes among persons who develop an acute myocardial infarction (AMI), but it is still unclear whether the negative effects associated with diabetes differentially affect the various manifestations of AMI including non-ST segment elevation AMI (NSTEMI) and ST-segment elevation AMI (STEMI). The importance of studying patients with NSTEMI has been highlighted by updated clinical management guidelines released in 2011. 4 Although, in general, the indications for treatment of patients with NSTEMI or unstable angina are similar to those for stable angina,5–8 patients with diabetes were recommended for more aggressive and timely management. 4 Moreover, despite improvements in the medical management of patients presenting with NSTEMI over time, 9 this condition remains associated with a poor prognosis, especially among persons with previously diagnosed diabetes.10–12
The objectives of this observational study in residents of a large central MA metropolitan area were to examine differences, and decade-long trends, in the characteristics, treatment practices and short-term outcomes of patients with and without a history of diabetes hospitalized for NSTEMI at all 11 medical centres in the Worcester, MA, metropolitan area. Data from the Worcester Heart Attack Study were utilized for this investigation.13–15
Methods
This study utilized data from the Worcester Heart Attack Study. This is an ongoing population-based observational study describing long-term trends in the incidence, hospital and post-discharge case-fatality rates (CFRs) of AMI among residents of the Worcester metropolitan area (2000 census estimate = 478,000) hospitalized at all 11 central MA medical centres. The details of this study have been previously described.13–15 In brief, the medical records of patients from this large metropolitan area hospitalized for possible AMI were individually reviewed and a diagnosis of AMI was validated according to predefined criteria. 13 Patients who developed AMI secondary to an interventional procedure or surgery were excluded from the study sample. This study was approved by the Institutional Review Board at the University of Massachusetts Medical School.
In this investigation, we only included patients with NSTEMI which was defined by the absence of a new ST-segment elevation at the J point in electrocardiography (ECG) leads. We further classified patients as having a history of diabetes, or the absence thereof, based on the review of data available in hospital medical records. 16
Demographic, medical history and clinical data were abstracted from the hospital medical records of patients with confirmed AMI by trained study physicians and nurses. Information was collected about patient’s age, sex, race, medical history, AMI order (initial vs prior), physiologic factors, laboratory test results, length of hospital stay and hospital discharge status.13–15 Information about the hospital use of cardiac medications and receipt of coronary angiography, percutaneous coronary intervention (PCI) and coronary artery bypass graft (CABG) surgery was collected. Development of several significant clinical complications (e.g. atrial fibrillation, cardiogenic shock, stroke, heart failure) during the patient’s index hospitalization was defined according to standardized criteria.17–20
Data analysis
We examined differences in the demographic and clinical characteristics, treatment practices and hospital outcomes between diabetic as compared with non-diabetic patients hospitalized with NSTEMI through the use of chi-square and t-tests for discrete and continuous variables, respectively.
In-hospital CFRs and the proportion of patients developing various in-hospital clinical complications were calculated in a standard manner. Kaplan–Meier curves were constructed and log-rank tests were performed to examine differences in post-discharge all-cause mortality between diabetic as compared with non-diabetic patients with NSTEMI. A series of multivariable-adjusted logistic regression analyses were carried out to assess the overall impact of diabetes, and the significance of changing trends between 1999 and 2009, in the odds of developing atrial fibrillation, stroke, heart failure, cardiogenic shock and dying during the acute hospitalization while controlling for several potentially confounding demographic, medical history and clinical factors that have been shown to affect these outcomes. Potential confounders included in these analyses were age, sex and history of other coexisting disorders (e.g. coronary heart disease, heart failure, hypertension, stroke, cancer, liver and renal disease). Due to the observational nature of the study, and the difficulty in interpretation of any observed associations, we did not control for the hospital receipt of various cardiac medications or coronary interventional procedures in examining the association between previously diagnosed diabetes and our principal hospital outcomes.
Results
Study population characteristics
The study sample consisted of 3916 patients diagnosed with NSTEMI at all hospitals in central MA on a biennial basis between 1999 and 2009. The average age of these patients was 73 years, 54% were male and 38% had a history of diabetes based on the review of information contained in hospital medical records.
Patients with a history of diabetes were more likely to be women, have a higher average body mass index (BMI) and a greater prevalence of comorbid conditions as compared with non-diabetic patients (Table 1). Patients with previously diagnosed diabetes were less likely to have presented with classical anginal symptoms, including chest or left arm pain, but were more likely to have presented with dyspnoea.
Characteristics of diabetic and non-diabetic patients hospitalized with NSTEMI.
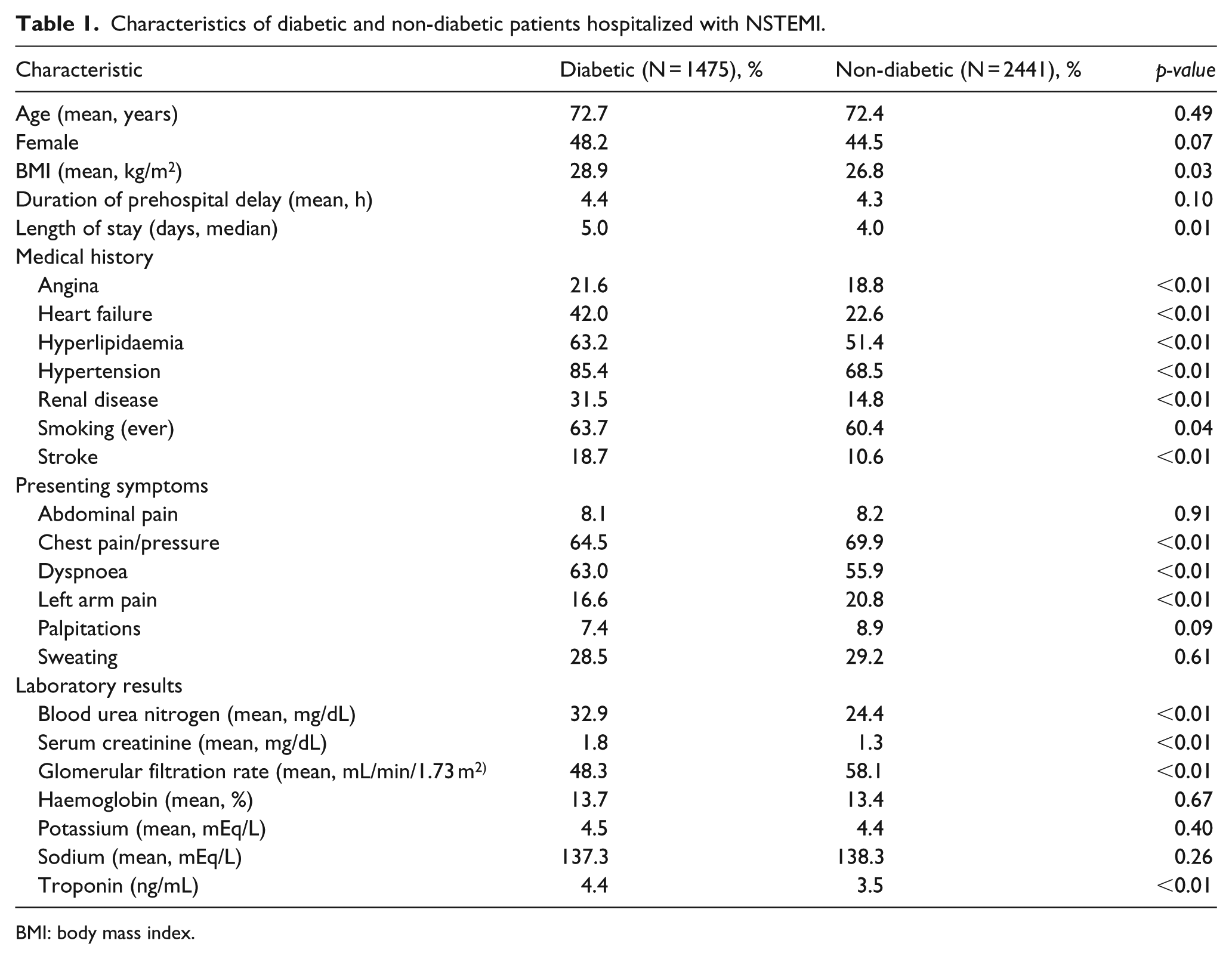
BMI: body mass index.
In terms of baseline laboratory findings, patients with a history of diabetes were significantly more likely to have presented with higher peak troponin, blood urea nitrogen and serum creatinine levels, but were more likely to have a lower glomerular filtration rate (GFR) as compared with non-diabetic patients (Table 1).
Hospital treatment practices
During the years under study, there were significant increases over time in the utilization of recommended cardiac medications during hospitalization, including angiotensin-converting enzyme (ACE) inhibitors/angiotensin receptor blockers (ARBs), aspirin, β-blockers and statins in both diabetic and non-diabetic patients presenting with NSTEMI (Figure 1). In patients with a history of diabetes, marked increases were observed in the rates of prescribing ACE inhibitors/ARBs (from 58.9% to 69.0%), β-blockers (from 76.7% to 95.1%) and lipid-lowering drugs (from 45.8% to 92.9%) between 1999 and 2009, respectively. Overall, diabetic patients were more likely to have received ACE inhibitors/ARBs, calcium channel blockers, diuretics and lipid-lowering drugs during their acute hospitalization as compared with non-diabetic patients (Table 2). Diabetic patients had a significantly longer hospital stay (median 5.0 vs 4.0 days) than patients without previously diagnosed diabetes (p < 0.05).
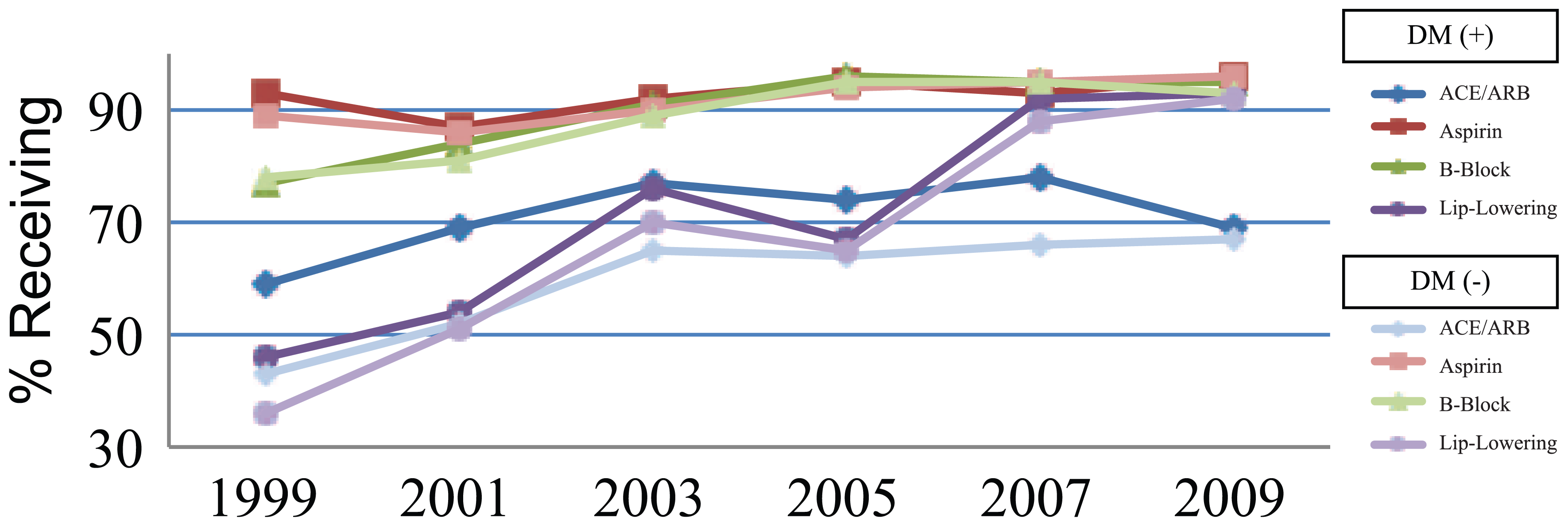
Trends in receipt of in-hospital medications in diabetic and non-diabetic patients hospitalized with NSTEMI.
Hospital management practices in diabetic and non-diabetic patients hospitalized with NSTEMI.
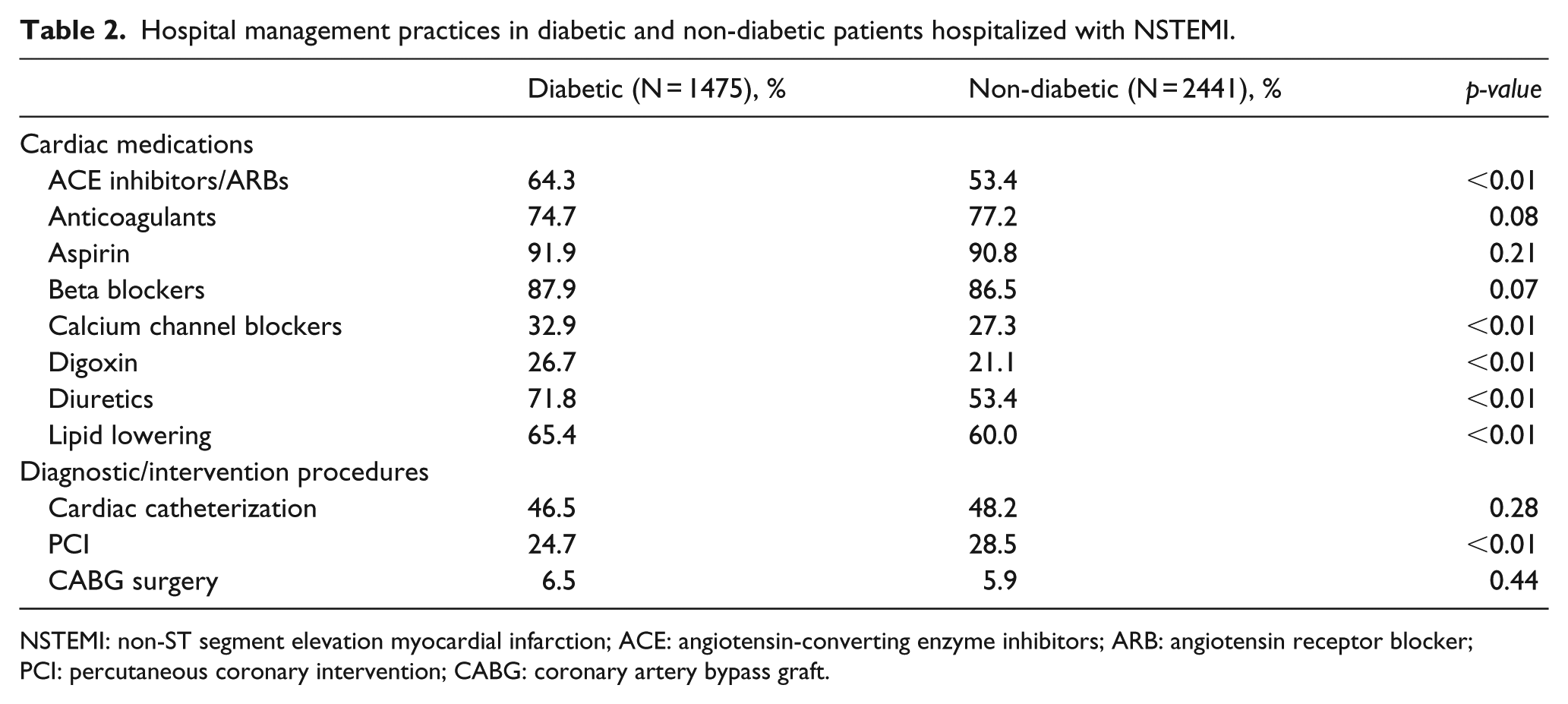
NSTEMI: non-ST segment elevation myocardial infarction; ACE: angiotensin-converting enzyme inhibitors; ARB: angiotensin receptor blocker; PCI: percutaneous coronary intervention; CABG: coronary artery bypass graft.
Although there were marked increases over time in the proportion of patients with and without diabetes undergoing cardiac catheterization and PCI during their index hospitalization (Figure 2), patients with diabetes were slightly less likely to have undergone cardiac catheterization (46.5% vs 48.2%) or a PCI (24.7% vs 28.5%), but slightly more likely to have undergone CABG surgery (6.5% vs 5.9%) than patients without a history of diabetes (Table 2).
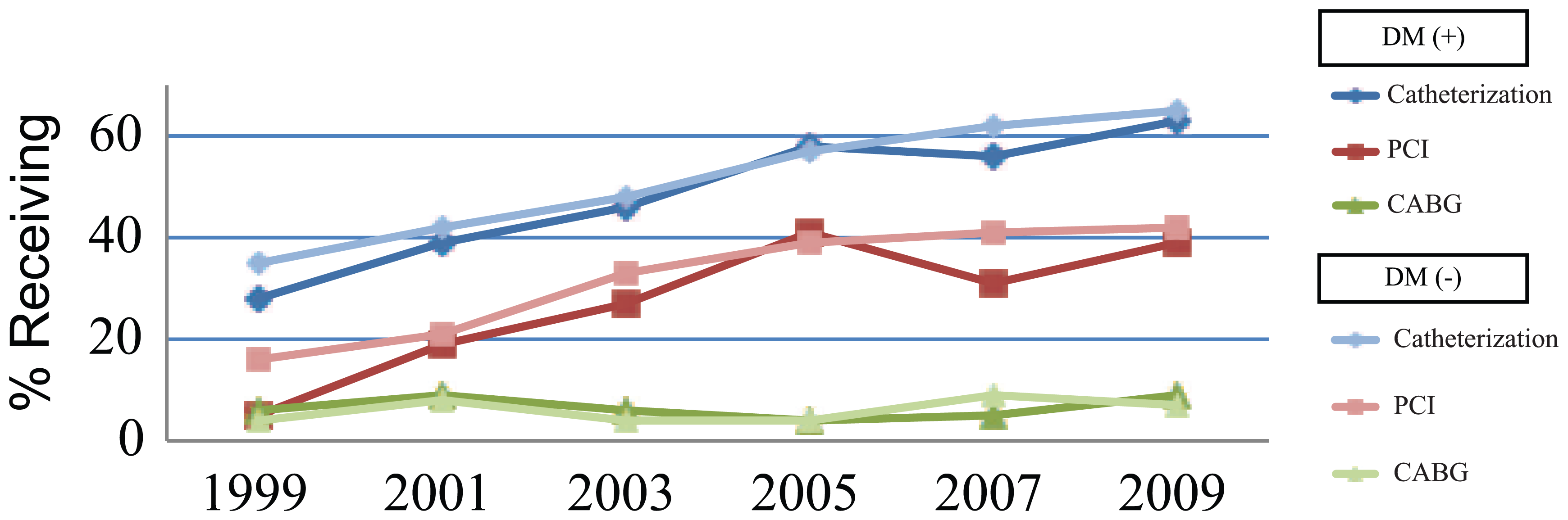
Trends in receipt of in-hospital procedures in diabetic and non-diabetic patients hospitalized with NSTEMI.
In-hospital outcomes
Diabetic patients were more likely to have developed important in-hospital complications including heart failure and cardiogenic shock compared to those without a history of previously diagnosed diabetes (Table 3). Patients with a history of diabetes also experienced significantly higher in-hospital death rates as compared to those without diabetes (11.4% vs 9.5%, p = 0.02). There were no significant changes in the frequency of these clinical complications during the decade-long period under study for patients with or without previously diagnosed diabetes (Figure 3).
Risk of developing selected in-hospital complications in diabetic compared with non-diabetic patients.
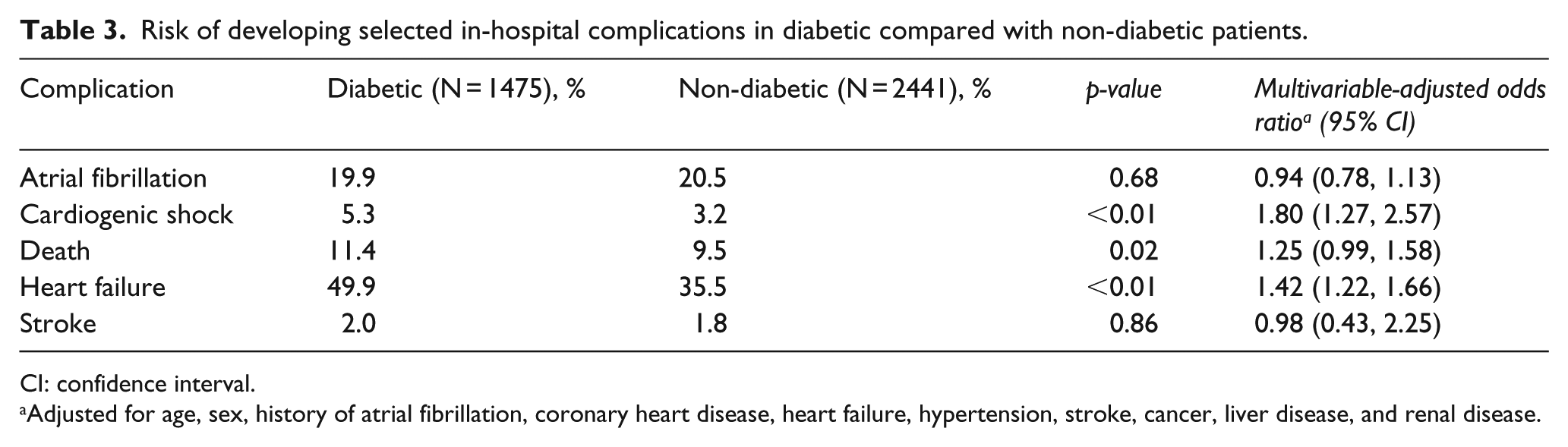
CI: confidence interval.
Adjusted for age, sex, history of atrial fibrillation, coronary heart disease, heart failure, hypertension, stroke, cancer, liver disease, and renal disease.
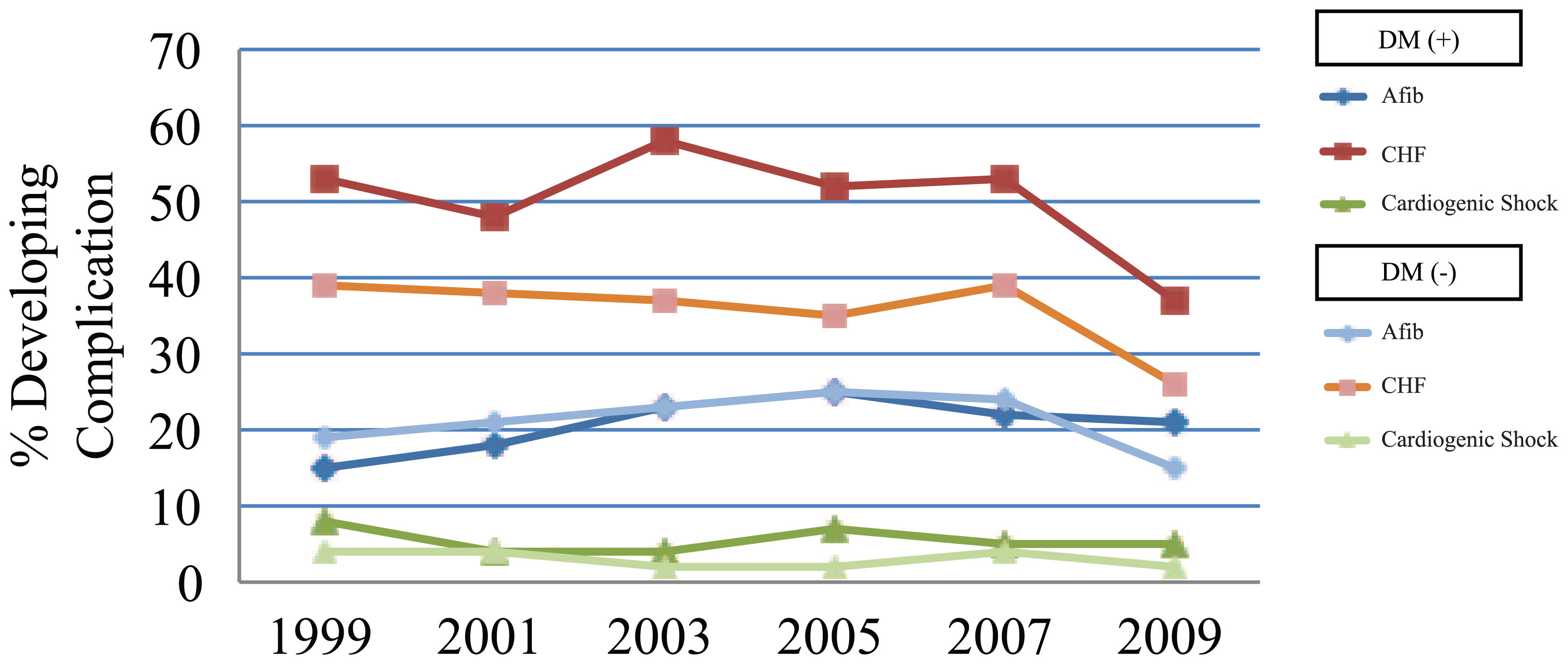
Trends of in-hospital cardiac complications in diabetic and non-diabetic patients hospitalized with NSTEMI.
We examined the risks of developing important in-hospital complications as well as dying in patients with and without diabetes after adjusting for several confounding factors of prognostic importance. Our multivariable-adjusted results showed that diabetic patients were significantly more likely to have developed heart failure or cardiogenic shock during their acute hospitalization than patients without previously diagnosed diabetes (Table 3). Diabetic patients had a borderline significant 25% higher multivariable-adjusted odds of dying during hospitalization when compared with patients without a history of diabetes. Kaplan–Meier curves showed that the overall survival was significantly poorer in patients with diabetes as compared to those without previously diagnosed diabetes (log-rank test, p < 0.01) (Figure 4). A significant decline in in-hospital crude death rates was observed in both diabetic (14.3%–8.9%) and non-diabetic patients (12.2%–4.1%) between 1999 and 2009.
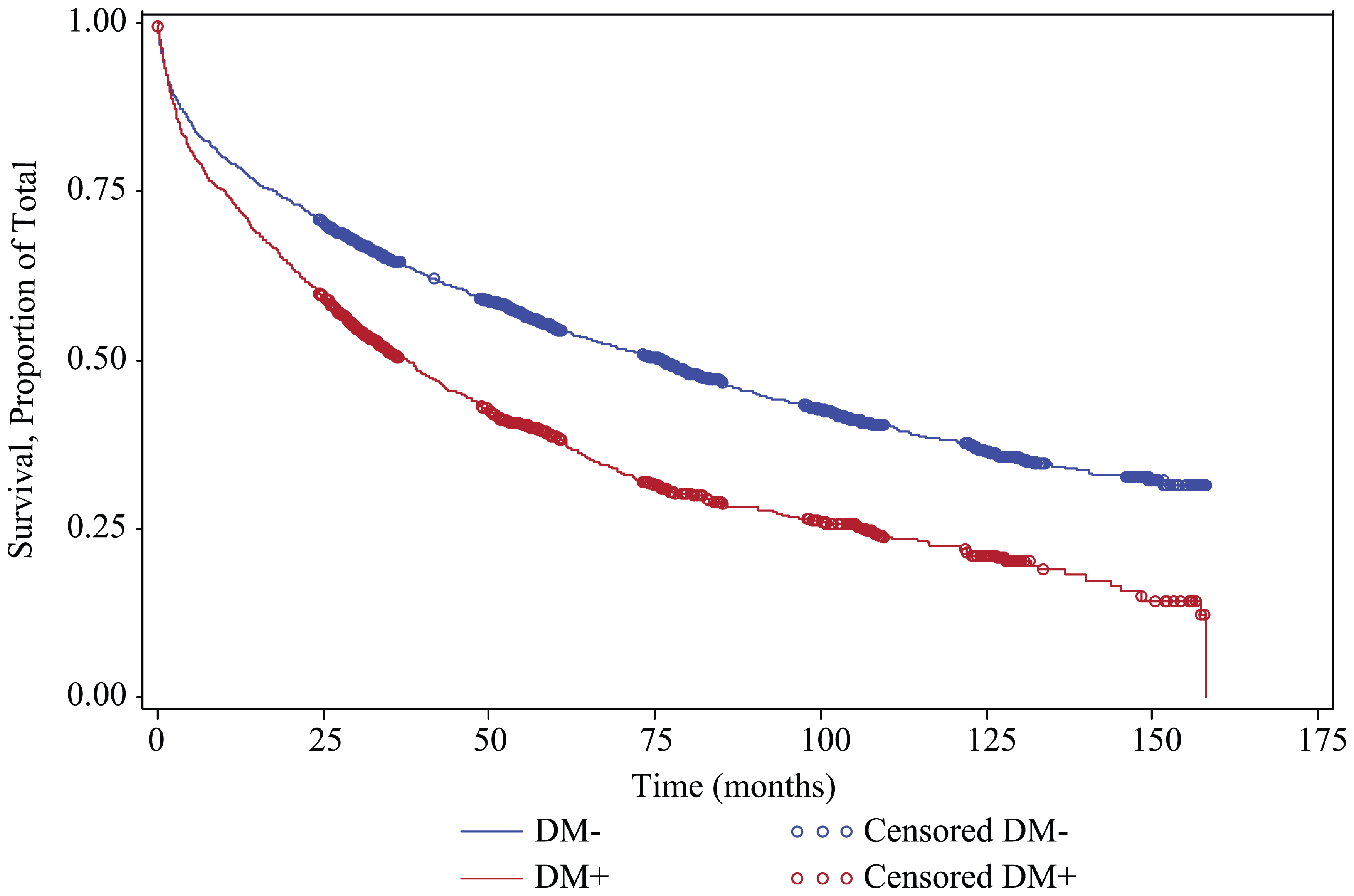
Kaplan–Meier curves for total mortality among diabetic and non-diabetic patients hospitalized with NSTEMI (1999–2009).
Discussion
The results of this study suggest that patients with an NSTEMI and a history of diabetes present with a greater prevalence of cardiovascular risk factors than non-diabetic patients. Despite encouraging trends in the use of guideline-directed medical and invasive treatments in diabetic patients over the study period, these individuals remained at higher risk than non-diabetics for developing important in-hospital complications.
Study population characteristics
Our findings are similar to those of prior studies which have shown that a considerable proportion of patients hospitalized with an NSTEMI have been previously diagnosed with diabetes. Our observed prevalence rate of previously diagnosed diabetes in this population of 38% compares with prevalence estimates of 35% in the National Cardiovascular Data Registry (NCDR) 21 and 30% in the Organization to Assess Strategies in Acute Ischemic Syndromes (Oasis) trial. 22
Diabetic patients hospitalized with NSTEMI are more often female with a higher BMI and are more likely to present with cardiac as well as other comorbidities which increase their overall risk of developing adverse outcomes. 21 The higher prevalence of comorbidities among patients with a history of diabetes might be explained by a higher prevalence of macro- or microvascular disease, chronic kidney disease, unfavourable serum lipid levels or perhaps related to preexisting diabetic cardiomyopathy. Our study also supports findings from previous investigations which have shown that diabetic patients are less likely to present with classical anginal symptoms than patients without previously diagnosed diabetes.23,24 In a recently published study from the NCDR Acute Coronary Treatment and Intervention Outcomes Network–Get with the Guidelines (ACTION Registry-GWTG), that examined differences between diabetic and non-diabetic patients with AMI from 462 US sites, patients with diabetes were more likely to be women, have a higher BMI and tended to have more cardiac risk factors than patients without diabetes. 21
While there were no significant differences in serum haemoglobin or various electrolyte levels between diabetic and non-diabetic patients, patients with previously diagnosed diabetes had significantly higher serum levels of creatinine and blood urea nitrogen, and a lower GFR, suggestive of poorer renal function in these patients. A decreased GFR has been associated with an increase in mortality in healthy as well as in high-risk, diseased patient populations.25,26 In addition, higher peak troponin levels in patients with previous history of diabetes have been shown to be associated with unfavourable short- and long-term outcomes in patients with NSTEMI.27,28
Hospital management practices
Encouraging trends were observed in the prescribing rates of evidence-based in-hospital cardiac medications during the years under study in diabetic as well as non-diabetic patients. Overall, patients with diabetes were significantly more likely to have received ACE inhibitors/ARBs than non-diabetic patients. Similar prescribing patterns were observed in the ACTION Registry-GWTG when comparing NSTEMI patients with and without diabetes, 21 as well as in the National Registry of Myocardial Infarction that studied patients presenting with AMI between 1994 and 2006. 29 Despite findings that have shown β-blockers to benefit patients with diabetes to a greater extent than those without diabetes in the immediate post-myocardial infarction period,30,31 no differences in the prescribing rates (almost 90% in both groups) of this medication were observed in the present study.
While the proportion of patients with previously diagnosed diabetes who underwent cardiac catheterization was essentially similar to patients without diabetes, diabetic patients were less likely to have undergone a PCI compared with non-diabetics but were slightly more likely to have undergone CABG surgery during their index hospitalization. Similar findings were reported from the ACTION Registry-GWTG, the GRACE study and the National Registry of Myocardial Infarction.22,32,33 The reasons why patients with previously diagnosed diabetes are more likely to undergo CABG surgery in the setting of an acute coronary event is likely explained by this metabolic disorder promoting atherogenesis and endothelial dysfunction, leading to more advanced underlying atherosclerosis. 29 While most previous studies that compared different revascularization procedures in patients with diabetes and underlying coronary heart disease, especially those with multi-vessel disease, suggest that these patients benefit more from undergoing CABG surgery than PCI,32,34 some recent studies suggest that modern PCI techniques with optimal medical treatment might not be inferior to undergoing CABG surgery. 34
Since diabetic patients presenting with NSTEMI represent a high-risk group, recent updates in practice guidelines have recommended a more aggressive early invasive strategy in their acute management. 4 Indeed, the proportion of NSTEMI patients with diabetes who underwent coronary revascularization more than doubled in our study between 1999 and 2009. Despite multiple studies showing encouraging increases in the proportion of NSTEMI patients with diabetes treated with invasive coronary strategies, diabetic patients remain no more likely than non-diabetics to undergo coronary revascularization, and there remains an underuse of these more aggressive treatment approaches for this high-risk population.33,35 In a recent study using data from the nationwide ACTION Registry-GWTG, NSTEMI patients with a history of diabetes were less likely to have undergone a cardiac catheterization or PCI than persons without diabetes, while they were more likely to have undergone CABG surgery, between 2007 and 2011. 21 A number of international studies have shown similar results. For example, in an analysis of 847 patients with a recently diagnosed NSTEMI hospitalized at a single medical centre in Zwolle, Netherlands, between 2005 and 2009, while cardiac catheterization was performed equally in patients with and without diabetes, PCI was performed significantly less often in patients with diabetes, and CABG surgery was performed at a similar rate in patients with and without diabetes. 12
In-hospital outcomes
After controlling for several important potentially confounding factors of prognostic importance, persons with diabetes were at increased odds for developing heart failure, cardiogenic shock and dying during their acute hospitalization compared to those without a history of previously diagnosed diabetes. Similar to our findings, NSTEMI patients with diabetes in the ACTION Registry-GWTG were more likely to have developed cardiogenic shock, and have died during hospitalization compared to patients without diabetes. 21 In the GRACE study, NSTEMI patients with diabetes had a significantly higher risk for developing heart and renal failure compared to patients without diabetes during their acute hospitalization. 33 While we observed a decline in in-hospital death rates for both diabetic and non-diabetic patients during the years under study, overall, and during the most recent year under study, diabetic patients remained at increased risk for dying. These findings highlight the need for wider adoption of recent guidelines for the management of high-risk NSTEMI patients, including persons with diabetes, and for the continued examination of trends in short-term CFRs according to diabetes status in patients hospitalized with AMI.
There are several reasons that may explain the worse hospital outcomes observed in patients with previously diagnosed diabetes. Coronary revascularization through the utilization of PCI was performed significantly less often in patients with as compared to those without diabetes. Patients with diabetes may have more diffuse or distal underlying coronary artery disease resulting in a coronary anatomy less suitable for successful revascularization or to a higher prevalence of renal disease discouraging the use of the extra contrast media used in performing a PCI.
A multiplicity of additional factors may also result in a higher risk for adverse outcomes in persons with diabetes. These include diabetic cardiomyopathy, small vessel disease, alterations in platelet activity and fibrinolysis and poorer kidney function as reflected by higher blood urea nitrogen and serum creatinine levels, and a lower estimated GFR. It is also possible that NSTEMI patients with previously diagnosed diabetes may have been treated with less than optimal ‘therapeutic doses’ of effective medications during their acute hospitalization or may have developed a more severe AMI.10,32,33,35 The high prevalence of vascular risk factors among diabetic patient presenting with NSTEMI highlight the importance of developing multifactorial interventions aimed at the tight control of these risk factors to reduce the risk of microvascular and macrovascular complications and improve patient outcomes.
Study strengths and limitations
The strengths of our study include the large community-based sample of patients with confirmed NSTEMI from a large central New England metropolitan area whose demographic and socio-economic characteristics reflect those of the US population as a whole. We were also able to examine decade-long trends in a variety of NSTEMI associated clinical characteristics and important hospital clinical outcomes. However, this study has several limitations that need to be considered in the interpretation of our results. The diagnosis of diabetes was based on data from hospital medical records and not according to predefined measurements or a standardized study protocol. Additionally, due to the observational nature of the study that was carried out at 11 hospitals over varying time periods, we did not have access to systematically collected haemoglobin A1c or fasting glucose levels, glucose tolerance test results, type of outpatient treatments that patients may have received, duration of time that patients were known to be diabetic or other information to further characterize patient’s chronic glycometabolic status.
Conclusion
The results of this community-wide study provide insights into the characteristics, short-term management and in-hospital outcomes of diabetic as compared with non-diabetic patients presenting with NSTEMI. Despite encouraging trends in both the medical and invasive treatment of patients with NSTEMI, diabetic patients remained at increased risk of several adverse in-hospital outcomes as compared with non-diabetic patients. These findings indicate the need for the enhanced awareness of the increased risk of NSTEMI patients presenting with diabetes as well as the more optimal use of proven cardiac treatments in the management of these complex, high-risk patients.
Footnotes
Acknowledgements
We wish to acknowledge all persons involved in the review of data for this project as well as our collaborators at all greater Worcester hospitals. All authors had access to the data and had a role in writing this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This research was made possible by the cooperation of participating hospitals in the Worcester metropolitan area. Funding support was provided by the National Institutes of Health (RO1 HL35434). Partial salary support for Drs Gore, McManus, and Goldberg was provided for by National Institutes of Health grant 1U01HL105268-01 and to Dr McManus by National Institutes of Health Grant KL2RR031981.