
Abstract
The aim was to analyse the relationship between metabolic syndrome and type 2 diabetes mellitus risk among the aged. This was a prospective population-based study, with a 9-year follow-up. All subjects of the municipality of Lieto in Finland aged ≥64 in 1998–1999 with no type 2 diabetes mellitus at baseline (n=1117) were included. Hazard ratios for incident type 2 diabetes mellitus predicted by metabolic syndrome (defined by modified International Diabetes Federation criteria) were estimated. During the 9-year follow-up, a total of 69 participants (6.2%) developed type 2 diabetes mellitus. After multivariable adjustment (age, gender, smoking, frequency of exercise, cardiovascular disease and low-density lipoprotein-cholesterol), type 2 diabetes mellitus (hazard ratio, 95% confidence interval) (3.15, 1.89–5.25, p < 0.001) was more common in subjects with metabolic syndrome compared to subjects without it. Evaluating metabolic syndrome components individually, impaired fasting glucose (5.09, 2.64–9.82, p < 0.001) and obesity (1.71, 1.05–2.97, p = 0.034) predicted a higher incidence of type 2 diabetes mellitus. Our findings suggest that metabolic syndrome predicts onset of type 2 diabetes mellitus even in late life. Impaired fasting glucose and obesity should be targets for primary prevention of diabetes among the aged with metabolic syndrome.
Introduction
Diabetes is underestimated as a major global cause of premature mortality because only a minority of persons with diabetes mellitus (DM) die from a cause uniquely related to the condition. 1 Vascular complications of type 2 DM account for the majority of social and economic burden among patients and societies.1,2 The incidence of type 2 DM can be reduced through lifestyle changes.3–6 Therefore, it is important to identify high-risk individuals for type 2 DM.
Major risk factors for diabetes include positive family history, obesity, glucose intolerance and impaired fasting glucose. Metabolic syndrome (MetS), also including obesity and impaired fasting glucose, represents the clustering of risk factors for diabetes and vascular diseases. However, since the development of the MetS concept, there has been much controversy regarding its value to identify persons with a high risk for diabetes and cardiovascular disease. 7
Previous studies concerning MetS as a risk factor for diabetes have been conducted mostly among middle-aged populations, and elderly subjects have been involved only in some studies. According to a meta-analysis based on 16 cohorts, 8 MetS, defined by various criteria, predicted diabetes more strongly than it predicted coronary heart disease events among an adult population. The association of MetS with incident type 2 DM is less studied among the aged. According to Sattar et al., 9 MetS and its components were strongly associated with type 2 DM in two prospective studies in elderly populations.
The aim of our study was to analyse whether MetS and/or its individual components, as defined by modified criteria of the International Diabetes Federation (IDF), predicted incident type 2 DM in an aged Finnish cohort during the 9-year follow-up.
Materials and methods
This study is a part of the longitudinal epidemiological study carried out in the municipality of Lieto in south- western Finland.10,11 The longitudinal study was designed to describe the prevalence, risk factors and prognosis of cardiovascular, respiratory and other common diseases in an unselected Finnish population aged 64 years and over. All persons born in or prior to 1933 (n = 1529) were asked to participate and examinations were carried out between March 1998 and September 1999. Of those eligible, 63 died before they were examined and 273 refused or did not respond, leaving 1260 (82.4%) participants, 533 men and 727 women. 11 The sample for the current study consisted of 1117 (88.7%) persons who had neither a diagnosis of type 2 DM (International Classification of Diseases (ICD)-10 codes E10–E14) nor serum fasting glucose >7 mmol/l at baseline and who had sufficient data on MetS and confounding factors. They were followed up for 9 years in order to determine the incidence of type 2 DM, as will be described later.
Weight and height were measured and body mass index (BMI), measured as kg/m2, was calculated. Blood pressure was measured in a sitting position using the standard cuff method and a mercury sphygmomanometer. Systolic blood pressure was determined by the Korotkoff phase 1 and diastolic blood pressure by the Korotkoff phase 4 or 5. Two values were recorded with 2 mmHg accuracy 5 min apart and the mean values were used. Blood samples were drawn after an overnight fast at the Health Centre and they were analysed in the Central Laboratory of Turku University Hospital. Diabetes was defined based on a previous diagnosis (E10–E14) in the medical records and/or treatment with anti-diabetic agents (Anatomical Therapeutic Chemical (ATC) code A10) and/or fasting serum glucose level ≥7 mmol/l measured during the baseline examinations in 1998–1999. 12
Confounding factors
Gender, age, cardiovascular disease and frequency of exercise were used as confounding factors. Data on the frequency of exercise (1–7 d/week; less than once per week– not at all) were collected by interview. Cardiovascular disease at baseline consisted of ICD-10 codes I10–I15, I20–I25, I50, I60–I66, I69, I71 and I74.
Definition of MetS
To determine the subjects who had MetS, the modified definition of the IDF16,17 was used: BMI > 30 kg/m2 plus any two of the following four factors: 1. raised triglycerides (≥ 1.7 mmol/l) or specific treatment for this lipid abnormality (C10AB); 2. reduced high-density lipoprotein (HDL)-cholesterol (≤ 1.03 mmol/l for men; ≤ 1.29 mmol/l for women) or specific treatment for this lipid abnormality (C10AC); 3. raised blood pressure (systolic ≥ 130 mmHg or diastolic ≥ 85 mmHg) or treatment of previously diagnosed hypertension (C02, 03, 07–09); 4. elevated fasting plasma glucose ( ≥ 5.6 mmol/l) or previously diagnosed type 2 DM. In our study, waist circumference (WC) was not measured and therefore we used modified criteria of IDF where BMI ≥30 kg/m2 was used to assume central obesity (according to the definition by IDF, if BMI is >30 kg/m2, central obesity can be assumed and WC does not need to be measured).13,14
The incidence of type 2 DM during the follow-up period
Incidence of type 2 DM (ICD-10 codes E10–E14) was obtained from Finnish official registers using the unique personal identification numbers. Registers used between 1998 and 2008 were the Finnish Hospital Care Register provided by the National Institute for Health and Welfare, the Finnish Cause of Death Registry (Statistics Finland) and the Special Refund Entitlement Register at Social Insurance Institution in Finland (use of type 2 DM medication entitled to reimbursement payments under the Special Refund Categories).
Ethics
The study was conducted according to the guidelines of the Declaration of Helsinki. The Ethics Committee of the Hospital District of Varsinais-Suomi approved the study protocol. Participants gave their informed consent.
Statistical analyses
At baseline, differences between subjects with MetS and without MetS were assessed using the χ2 test, Fisher’s exact test or two-sample t-test. Kolmogorov–Smirnov’s test was used to test the normality of distributions. Because of the skewed distributions, triglyceride was log-transformed and glucose was square (x2)-transformed for statistical analyses.
Hazard ratios and their 95% confidence intervals (CI) for type 2 DM were calculated using Cox proportional hazard models separately for men and women. The follow-up periods were calculated from baseline measurements to the end of the follow-up period of 9 years or to the onset of type 2 DM. Analyses were adjusted for confounding factors: age; frequency of exercise; cardiovascular disease. The associations between MetS and each of its individual components and type 2 DM were analysed by adjusting confounding factors and in the analyses of individual components also by other components of MetS. P-values <0.05 were considered statistically significant. All statistical analyses were performed using SAS System for Windows, version 9.1 (SAS Institute Inc., Cary, NC, USA).
Results
Baseline characteristics
The mean age of participants (n = 1117) was 73.4 (SD 6.8) years. Subjects fulfilling the criteria of MetS (n = 177; 15.8% of the 1117 participants) exercised less frequently than those having no MetS (n = 940; Table 1). Cardiovascular disease was more common among subjects with MetS than among those without it. Low-density lipoprotein-cholesterol concentration did not significantly differ between those with MetS and those without it.
Baseline characteristics of all participants with no type 2 diabetes mellitus (n = 1117) by metabolic syndrome.
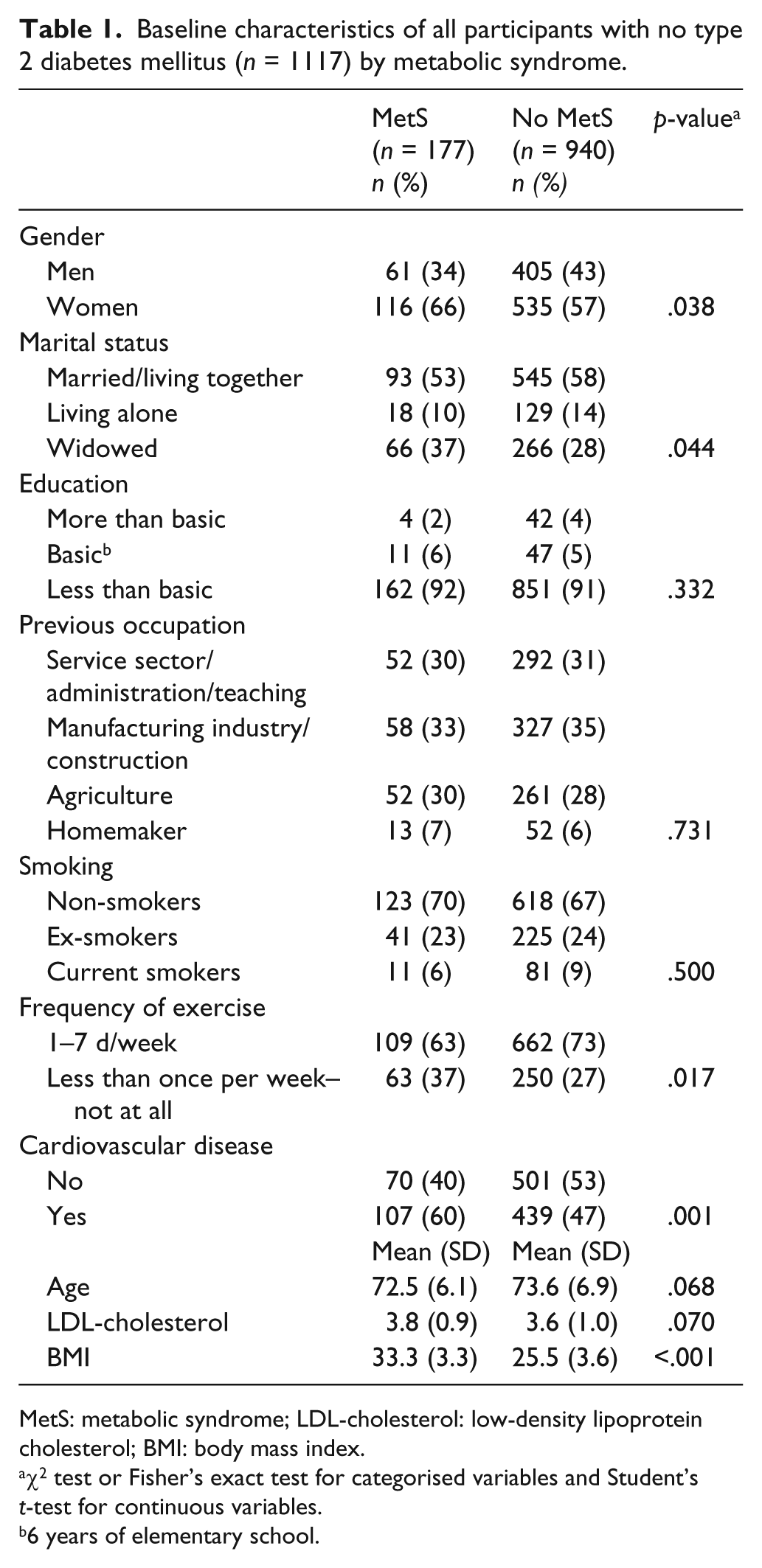
MetS: metabolic syndrome; LDL-cholesterol: low-density lipoprotein cholesterol; BMI: body mass index.
χ2 test or Fisher’s exact test for categorised variables and Student’s t-test for continuous variables.
6 years of elementary school.
MetS and incident type 2 DM
During the 9 years of follow-up, 69 subjects (6.2% of the total sample of 1117; 27 (15.3%) of those with MetS and 42 (4.5%) of those without it) were diagnosed for type 2 DM. After the multivariable adjustment (gender, age, frequency of exercise and cardiovascular disease), the incidence of type 2 DM was greater in those with MetS compared to those not having MetS (Table 2).
Hazard ratios (95% CI)of MetS and individual components of MetS defined by International Diabetes Federation for incidence type 2 DM during the 9-year follow-up (n = 1117).
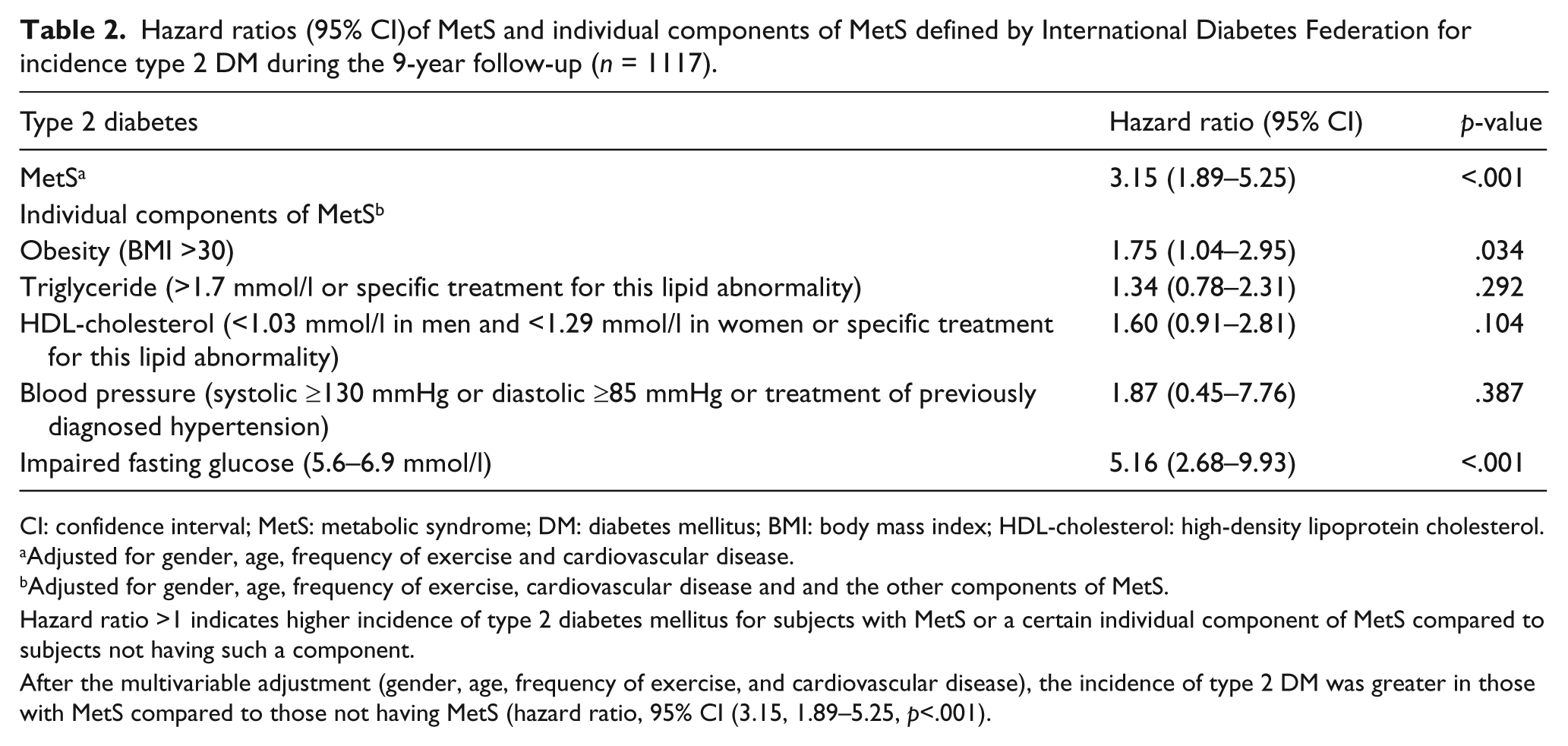
CI: confidence interval; MetS: metabolic syndrome; DM: diabetes mellitus; BMI: body mass index; HDL-cholesterol: high-density lipoprotein cholesterol.
Adjusted for gender, age, frequency of exercise and cardiovascular disease.
Adjusted for gender, age, frequency of exercise, cardiovascular disease and and the other components of MetS.
Hazard ratio >1 indicates higher incidence of type 2 diabetes mellitus for subjects with MetS or a certain individual component of MetS compared to subjects not having such a component.
After the multivariable adjustment (gender, age, frequency of exercise, and cardiovascular disease), the incidence of type 2 DM was greater in those with MetS compared to those not having MetS (hazard ratio, 95% CI (3.15, 1.89–5.25, p<.001).
Table 2 also shows adjusted hazard ratios (95% CI) for single components of MetS for the incidence of type 2 DM. Impaired fasting glucose and obesity (BMI > 30) predicted type 2 DM among the aged. In additional analyses, where subjects with impaired fasting glucose were excluded, none of the remaining components (obesity, triglycerides, HDL-cholesterol or blood pressure) of MetS did predict type 2 DM among aged subjects.
Discussion
In this population-based, 9-year follow-up study of aged Finns living in south-western Finland, MetS (defined by modified IDF criteria) predicted incident type 2 DM. Of the individual components of MetS, impaired plasma fasting glucose and obesity were independently associated with an increased risk of type 2 DM.
The results of our study are in line with the results of previous studies. According to a meta-analysis based on 16 cohorts, 8 MetS, defined by various criteria, predicted diabetes among an adult population. Sattar et al. 9 found that MetS was strongly associated with type 2 DM even in an aged population.
According to previous cohort studies conducted among adults6,15,16 and the aged, 9 all five single components of MetS (WC/BMI, blood pressure, serum HDL-cholesterol, serum triglycerides and impaired fasting glucose) predicted the occurrence of type 2 DM. In our study, of the single components of MetS, only impaired fasting glucose and obesity increased the risk of type 2 DM, which may be due to the lower number of persons with incident type 2 DM during the follow-up period compared with other studies. According to our study, impaired fasting glucose alone had a higher predictive value than MetS for the incidence of type 2 DM.
The study of Sattar et al. 9 included two cohorts of aged subjects and in both cohorts (The Prospective Study of Pravastatin in The Elderly at Risk, (PROSPER) and The British Regional Heart Study, (BRHS)), increased fasting glucose was strongly linked to the risk for incident diabetes. In PROSPER, nearly 50% of participants with fasting glucose >6.1 mmol/l progressed to develop overt diabetes. In BRHS, which included a younger-aged cohort, fasting glucose alone was similar to MetS in the prediction of diabetes. In an 8-year follow-up of the Framingham offspring middle-aged population, glucose cut-off was, by far, the best predictor of diabetes. 17
In the study of Laaksonen et al., 6 obesity was the most important predictor of type 2 DM among individuals aged 40–79 years. This is in accordance with previous cohort studies,4,5,18 which also suggest that weight control would apparently be the most effective strategy in type 2 DM prevention among an adult population. According to Biggs et al., 19 heavy weight gain in late life (after 65 years of age) is an important risk factor for diabetes. Although the risk associated with adiposity appeared to wane with age, individuals in the highest category of BMI remained at twice the risk of diabetes compared to those in the lowest category among participants 75 years of age or older. On the other hand, most epidemiological data argue in favour of beneficial or neutral, rather than detrimental, effects of a slight increase in BMI on life expectance after the age of 65 years. Furthermore, weight loss in the aged appears to hold various risks related mainly to loss of lean body mass and potential nutritional deficiencies.20–22 Thus, weight loss interventions should be cautious and individualised in older patients to limit the loss of lean body mass and to avoid nutritional deficiencies. Risk-benefit analysis is crucial in weight management in the aged and expected benefits must be assessed against potential detrimental effects of weight loss. 23
In a representative population sample of subjects aged 65–74 years, obesity and central obesity doubled the prevalence of impaired glucose tolerance (IGT) and type 2 DM. 24 The simultaneous presence of obesity, central obesity and family history of diabetes was associated with a threefold increase in the prevalence of IGT or type 2 DM. Thus, it is suggested that the MetS concept is not necessary or clinically needed to identify those at an increased risk for a new onset of type 2 DM. Simple questions (e.g. on age, family history of diabetes, ethnic origin, physical activity and diet) combined with common clinical measurements (e.g. BMI, waist and blood pressure) are sufficient. These non-laboratory measures can be used to identify high-risk individuals before any blood sample (primarily of fasting or postprandial glucose) is taken. 9 In support of this approach, simple questionnaires work well in predicting diabetes risk in several cohorts of middle-aged populations.4,25 For example, the Finnish Diabetes Risk Score (FINDRISC; including age, BMI, WC, antihypertensive drug therapy, history of high glucose level, physical activity and fruit and vegetable consumption) was used in the nationwide programme for prevention of type 2 DM in Finland during 2003 and 2010. 26 Filling in the FINDRISC may encourage a person who gets a high score to have his/her blood glucose measured. FINDRISC has also been found to identify people who are considered to be at a high risk for type 2 DM, but who currently have normal glucose levels. 25 To implement lifestyle intervention among them can be called true primary prevention of hyperglycaemia. In a screening strategy based on blood glucose measurement alone, this important group would remain unrecognised and would receive no intervention. 27
The original IDF definition of MetS was not used in our study due to the lack of WC measurement. We used BMI as the sole measure of obesity, which is a limitation of the study. Central obesity assessed by WC has been considered a pivotal and essential component of MetS in the new definition of IDF. However, if BMI is >30 kg/m2, central obesity can be assumed and it is not necessary to measure WC.13,14 Altogether, 15.8% of the subjects in our study fulfilled the criteria of MetS, having BMI >30 kg/m2 plus any two of the four other criteria. Using BMI instead of WC may have led to an underestimation of the prevalence of MetS in our study, because there may have been subjects fulfilling the criterion of central obesity (WC 94 cm in men and 80 cm in women) among those whose BMI was <30 kg/m2. The meta-analysis of 32 population-based studies showed that relative risks for diabetes were equivalent for standardised differences in BMI, WC and waist:hip ratio. 28 On the other hand, age-related physiological changes have a marked impact on body composition, including a decline in lean body mass and total body water in parallel with an increase in fat mass.29,30 Due to this, indexes of centralised fat distribution, primarily WC, appear to have a greater prognostic value than BMI for characterising obesity and associated health risks in the aged. 31 The sample size of our study was also fairly small compared to some other studies.5,9,15,18,19
The strengths of this study are the population-based design with very high participation rate and the long follow-up time. Almost the entire aged population living in Lieto participated. BMI measurements relied on clinical anthropometric assessment and information on type 2 DM was based on several registers. Incidence rates were adjusted for several confounding variables at baseline.
Da Qing IGT and Diabetes Study, 32 The Finnish Diabetes Prevention Study33,34 and Diabetes Prevention Program 35 have shown that type 2 DM can be prevented or at least delayed in high-risk subjects by lifestyle modification. Diagnosis of MetS may be useful in identifying high-risk individuals who benefit from evidence-based prevention or treatment.
In conclusion, our findings suggest that MetS predicts type 2 DM even in later life. Of individual components of MetS, impaired fasting glucose and obesity have the greatest impact predicting DM while other single components have no predictive value. Thus, the results of our study and those of earlier studies underscore the importance of treatment of risk factors in the aged, especially impaired fasting glucose and obesity.
Footnotes
Funding
This work was supported by the 19th February Fund of the Finnish Heart Association, the Turku Health Center Research Fund, the Turku University Hospital Research Fund, the Academy of Finland, the Yrjö Jahnsson Foundation and the Nordic Lions Club.
Conflicts of interest
None declared.