
Abstract
Background:
The aim was to evaluate the effect of comprehensive intensive therapy on the carotid and femoral arteries of intima-media thickness in patients with type 2 diabetes mellitus after 4-year follow-up.
Methods:
In this prospective 4-year study, patients (N = 210) with newly diagnosed type 2 diabetes received either comprehensive intensive therapy (n = 110) or conventional therapy (n = 100). Blood pressure, blood glucose and lipid levels were monitored every 3–6 months, and carotid and femoral arteries of intima-media thickness were monitored with ultrasonography. For the literature review, various databases were searched until 20 December 2014 for studies that evaluated effects of intensive multi-factorial therapies on comprehensive intensive therapy in type 2 diabetes mellitus patients.
Results:
The comprehensive intensive therapy group had a smaller rate of carotid intima-media thickness increase than the conventional therapy (control) group (p < 0.05). The carotid intima-media thickness in comprehensive intensive therapy group remained stable while the adjusted rate of carotid intima-media thickness increase was 12.55% in the control group. The femoral intima-media thickness change was also smaller in comprehensive intensive therapy group but the difference over time did not reach significance.
Conclusion:
The carotid intima-media thickness remained stable in type 2 diabetes mellitus patients who received comprehensive intensive therapy, suggesting that multi-factorial intensive therapies might have potential in reducing macro-vascular events in these patients.
Keywords
Introduction
The prevalence of type 2 diabetes mellitus (DM) is increasing worldwide,1,2 and China has the largest population of people with type 2 DM with a prevalence of 10.5% in its population aged 20–70 years. 1 Macro-vascular complications of type 2 diabetes are frequent causes of morbidity and mortality and are responsible for significant reduction in quality of life. The chance of developing macro-vascular diseases was estimated to be nearly 50% in subjects with early onset type 2 DM, 3 and the risk of dying from cardiovascular causes in patients with type 2 DM is two-fold higher than those without the disease.4,5
There have been different views in the ability of intensive blood glucose control alone to reduce the chance of developing macro-vascular events.6–8 Although the primary goals for managing type 2 DM have always been to control blood glucose levels using lifestyle changes and medications, it is becoming apparent that other risk factors of cardiovascular diseases, such as hypertension and dyslipidaemia, also play important roles in diabetes-associated complications. 9 The value of targeting multiple risk factors of macro-vascular events in patients with type 2 diabetes was demonstrated in the Steno-2 study which showed that long-term intensive multi-factorial intervention aiming at managing multiple risk factors successfully reduced rates of cardiovascular and micro-vascular events by about 50%.10,11 But besides the Steno-2 study, only a small number of other studies have investigated how different risk factors contribute to macro-vascular events in patients with type 2 DM,1,12–16 and most of these studies have been relatively short in the follow-up duration (⩽2 years).12–14,16
Although not without controversy, increased carotid intima-media thickness (cIMT) has been used to predict early coronary atherosclerosis, heart diseases and stroke. 17 Measurements of the cIMT can be performed non-invasively using high-resolution ultrasound and can be an effective way of identifying early development of cardio- and cerebrovascular complications.18,19
Our study was a continuation of Zhao et al. 14 which was a 2-year prospective study which found significantly lower values in the intensive multi-factorial therapy group compared with the conventional therapy group in total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), blood pressure [both systolic blood pressure (SBP) and diastolic blood pressure (DBP)], as well as cIMT, following 2 years of therapy. We concluded that early comprehensive (multi-factorial) and intensive treatment of type 2 DM can delay or even reverse the increase in intima-media thickness (IMT) of large arteries. 14 The purpose of this study was to evaluate the efficacy of comprehensive intensive therapy (CIT) in reducing cIMT and femoral intima-media thickness (fIMT) in patients with newly diagnosed type 2 DM after 4 years of follow-up. We also performed a systematic review on published studies in this field to allow for comparison of our findings with other reported data.
Subjects, materials and methods
Clinical study
This was a 4-year prospective study that enrolled subjects from Zhejiang University School of Medicine’s First Affiliated Hospital from July 2008 to December 2008. The study was performed according to the Declaration of Helsinki and the protocol was approved by the hospital’s institutional review board. All subjects gave their written informed consent. The study was registered on the Huaxi Hospital of Sichuan University’s evidence-based medical research website, with the following government-issued registry code: ChiCTR-TRC-00000234 Chinese Diabetes Complications Prevention Study (CDCPS).
Patients’ population
Patients with newly diagnosed type 2 DM were recruited from our department from July 2008 to December 2008. Type 2 DM was diagnosed according to the diagnostic criteria developed by the World Health Organization (WHO) in 1999.
Subjects (⩾70 years of age) with cardiovascular events or diseases that might impact their ability to participate in the study or interpretation of results were excluded. Also excluded from the study were subjects with cancers, acute or chronic liver or kidney dysfunction [blood creatinine >1.2 times of upper limit of normal; alanine aminotransferase (ALT) >2 times of upper limit of normal], bleeding tendencies and stress-related conditions such as ketoacidosis and hyperosmotic coma within 6 months after beginning this study. Patients who abused alcohol or drugs were also excluded. Patients who participated in another study within 4 weeks of the study’s start, had poor compliance or were lost to follow-up were also not included. Poor compliance was defined as the inability to adhere to treatment protocols such as taking medicine regularly and returning for scheduled follow-up visits every 3–6 months.
Study design
The following demographic information and patient disease characteristics were collected at baseline: history of smoking, drinking or diseases, occupation, physical activity, current medication and family history of type 2 DM (involving family members within three generations). Other variables assessed at baseline included body mass index (BMI), waist-to-hip ratio (WHR), fasting serum blood glucose levels, blood pressure, serum lipid levels (i.e. triglycerides, TC, LDL), and liver and kidney function.
Patients were assigned by personnel blind to patient allocation to either receive CIT or conventional therapy. Hypertension was diagnosed according to the guideline for the diagnosis and therapy of hypertension developed by WHO/International Society of Hypertension in 1999. Hyperlipidaemia was diagnosed according to the diagnostic criteria for hyperlipidaemia in the Third Report of the National Cholesterol Educational Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults [Adult Treatment Panel (ATP III)] in 2001.
The following parameters were used as the therapeutic goals for CIT: fasting blood glucose (FBG): ⩽7.0 mmol/L; glycosylated haemoglobin (HbA1c): ⩽7.0%; SBP: ⩽130 mmHg; DBP: ⩽85 mmHg; triglycerides: ⩽1.69 mmol/L; TC: ⩽4.68 mmol/L; LDL-C: ⩽2.6 mmol/L.
The CIT group’s therapies include intensive management and education aiming to bring changes in lifestyle, such as healthy diet, regular exercise and avoiding working at night. They also had their blood pressures, serum glucose and lipid levels monitored every 3 months, with the therapeutic regimen adjusted if necessary, during the follow-up period. Therapies also included pharmacotherapy to control and keep blood pressure, serum glucose and lipid levels within predesigned therapeutic goals.
The medications used in the CIT therapy group to control serum glucose include metformin (twice a day to the maximal dose of 1000 mg), long acting sulfonylureas, alpha-glucosidase inhibitors (twice/thrice a day), the glitazones (once/twice per day) and insulin injection, if oral agents failed to control. Anti-hypertensive medication includes calcium-channel blockers (once per day), angiotensin-converting enzyme inhibitors (ACEI) or angiotensin-receptor blockers (ARB) (once per day) and beta adrenergic receptor antagonist (usually given once per day). Statins (once per day at bedtime) were used to lower serum lipids. In the CIT group, all patients were required to take statins and aspirin, and there was no cost of the medications to the patient.
Subjects in the conventional therapy group received routine outpatient diabetic management and general health education and had blood glucose, lipid levels and blood pressure monitored every 6 months, but they were not given medications freely and no therapeutic goals were set for them. In the conventional treatment group, approximately 30% of patients were taking aspirin and about 40% were using statins. Patients with cardiovascular event were treated with aspirin but not any statins.
For both groups, the cIMT and fIMT were measured and recorded annually. The cIMT and fIMT were measured via ultrasound colour-flow Doppler (Sequoia 512; Siemens Medical Solutions USA Inc, Mountain View, CA, USA) with a 9–14 MHz probe. The measurements were made at 1.0 cm proximal to the carotid and femoral bifurcations, from their posterior arterial walls. For all patients, the ultrasound was performed by a single experienced technician who was blinded to patient treatment assignments.
During each visit for the CIT group, physicians would provide additional instructions regarding therapy and lifestyle or would adjust medication or discuss lifestyle modifications, but no such instruction, adjustment or discussion was provided for the conventional therapy group. Anti-hypertensive medication was given based on a patient’s blood pressure measurements with the purpose of maintaining the blood pressure within the normal range. Other laboratory values that might also affect the dosing of anti-hypertensive medications such as serum creatinine levels were monitored as well for the CIT group.
If chest tightness, chest pain or intermittent claudication occurred during the study period, the subject would receive an electrocardiogram, treadmill exercise test, ultrasonography of blood vessels of the lower limbs, computed tomography angiography (CTA) of coronary artery or angiography when needed to evaluate for the presence of any macro-vascular event. If a macro-vascular complication was confirmed, the subject was discontinued from the study.
Statistical analysis
For basic characteristics of subject, continuous variables were presented as means with standard deviations (SDs) and with independent t-tests for group comparison; categorical variables were presented as counts and percentages, with chi-square tests for group comparison.
The rates of IMT change in the carotid and femoral arteries were presented as medians and interquartile ranges (IQRs). The mixed-effect models were performed to detect the effects of follow-up times (denoted as time effect), groups (denoted as group effect) and their interaction (denoted as time × group effect) for the rates of IMT change in carotid and femoral arteries and the clinical factors associated with diabetes. If the main effect or interaction was shown to be significant, the post hoc multiple comparisons were conducted using Bonferroni correction to control overall type-I error rates. The adjusted mean rates of IMT change in the carotid and femoral arteries were determined if the rates of change were significant. Two-tailed p < 0.05 indicates statistical significance. The statistical analyses were performed with SAS software version 9.2 (SAS Institute Inc., Cary, NC, USA).
Literature review
Search strategy
The review was performed in accordance to the PRISMA guidelines. MEDLINE, Cochrane, EMBASE and Google Scholar databases were searched until 5 August 2014 for studies that evaluated the effects of multi-disciplinary intensive therapies in treating type 2 DM. The following search terms were used: diabetes, cIMT, multi-factorial therapy, multi-disciplinary therapy and CIT. Included studies were those that evaluated cIMT in subjects who had a confirmed diagnosis of type 2 DM. In included studies, the subjects must have received intervention (either medication or lifestyle change) to control the following parameters: serum glucose, serum lipids or blood pressure. Letters, editorials, comments and case reports were excluded from the systematic review. Studies were identified and manually searched by at least two independent reviewers. When there was uncertainty regarding eligibility, a third reviewer was consulted.
Data extraction
The following information and data were extracted from included studies: the name of the first author, year of publication, study design, number of participants in each study group, participants’ age and gender, details and types of intervention for each group, and the outcomes (cIMT and/or fIMT). Two reviewers extracted the data, with a third reviewer available to adjudicate any discrepancy.
Results
Clinical study
Baseline demographics and disease characteristics
The baseline demographics and disease characteristics refer to Zhao et al. 14 (Table 1). Briefly, a total of 210 patients newly diagnosed with type 2 DM were initially enrolled in the study. There were 116 males and 94 females, and the median age was 57.4 years (range: 35–70 years). In addition, concomitant hypertension was found in at least 107 patients and concomitant hyperlipidaemia was found in 82 patients. As patients were assigned into either CIT or conventional therapy group, there was no significant difference at baseline in the cIMTs and fIMTs between CIT and conventional therapy (control) group. There was also no difference between groups in the baseline values of other metabolic parameters.
Basic characteristics of study subjects.
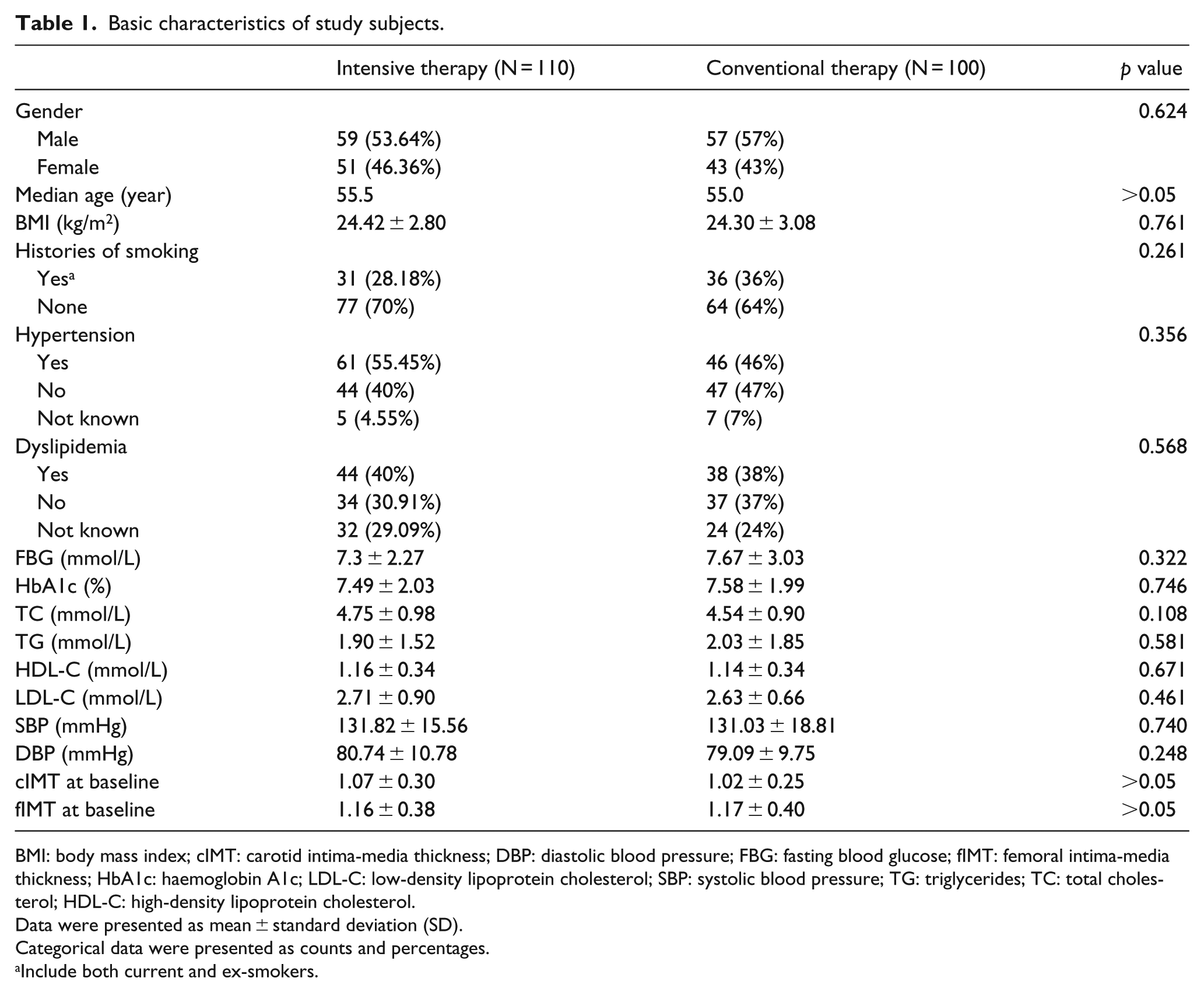
BMI: body mass index; cIMT: carotid intima-media thickness; DBP: diastolic blood pressure; FBG: fasting blood glucose; fIMT: femoral intima-media thickness; HbA1c: haemoglobin A1c; LDL-C: low-density lipoprotein cholesterol; SBP: systolic blood pressure; TG: triglycerides; TC: total cholesterol; HDL-C: high-density lipoprotein cholesterol.
Data were presented as mean ± standard deviation (SD).
Categorical data were presented as counts and percentages.
Include both current and ex-smokers.
Effects of therapy on IMT of the carotid artery (cIMT)
In the CIT group, the rate of change in cIMT shows significant difference in group effect, as well as in the interaction of group and time between two different therapy groups (p ⩽ 0.003), indicating the presence of difference between therapeutic groups in rates of cIMT change. But there was no significant time effect within the same treatment group (Table 2). Bonferroni post hoc comparison found that the conventional therapy group had significantly greater per cent increase in the cIMT than the CIT group (p < 0.001) in the fourth year. The adjusted rate of change of cIMT decreased at all time points in the CIT group, whereas the adjusted rate of change in the control group increased at all time points (Table 2).
Change rates of cIMT for the two intervention groups.
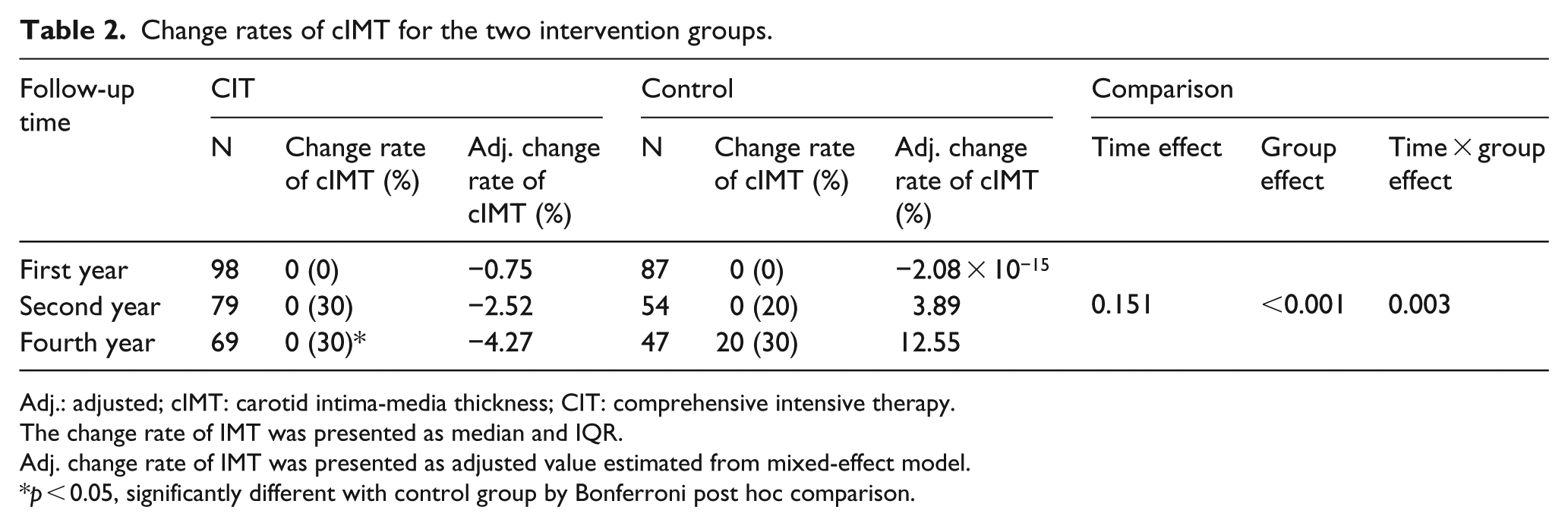
Adj.: adjusted; cIMT: carotid intima-media thickness; CIT: comprehensive intensive therapy.
The change rate of IMT was presented as median and IQR.
Adj. change rate of IMT was presented as adjusted value estimated from mixed-effect model.
p < 0.05, significantly different with control group by Bonferroni post hoc comparison.
Effects of therapy on IMT of the femoral artery (fIMT)
The change rate of fIMT was significantly different in group effect (p = 0.008), which means there was a difference between two different groups, but was not significantly different in time effect for the same treatment group or in the effect of time between control and CIT groups. According to Bonferroni post hoc multiple comparisons, the change rate of fIMT was significantly lower in CIT group than control groups in the second year (p values ⩽0.01) (Table 3). The adjusted fIMT change rates decreased at all time points in the CIT group, whereas the adjusted fIMT change rates increased at all time points in the control group (Table 3).
Change rate of fIMTs for the two intervention groups.
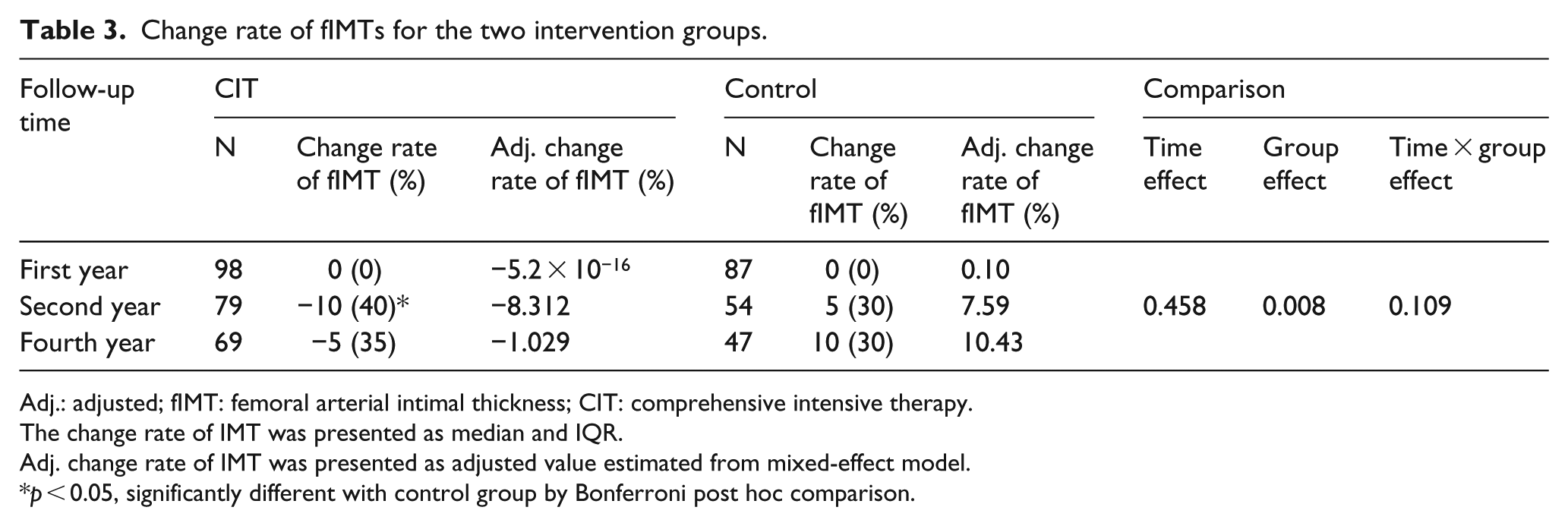
Adj.: adjusted; fIMT: femoral arterial intimal thickness; CIT: comprehensive intensive therapy.
The change rate of IMT was presented as median and IQR.
Adj. change rate of IMT was presented as adjusted value estimated from mixed-effect model.
p < 0.05, significantly different with control group by Bonferroni post hoc comparison.
Effects of therapy on the clinical factors associated with DM
Mean HbA1c and HDL-C were significantly different in time effect (all p ⩽ 0.001), but not significantly different in effect of group and the interaction; the mean HbA1c was increased in second and fourth year in CIT and control groups; the mean HDL-C was increased in fourth year (Table 4). The mean TG, SBP and DBP was significantly different in group effect (p ⩽ 0.011), but not in the time effect and interaction; the mean TG, SBP and DBP were higher in control group compared with CIT group in each year. There were no significant differences in time, group and the interaction effects in FBG and LDL-C.
Data of other metabolic parameters of the two intervention groups.
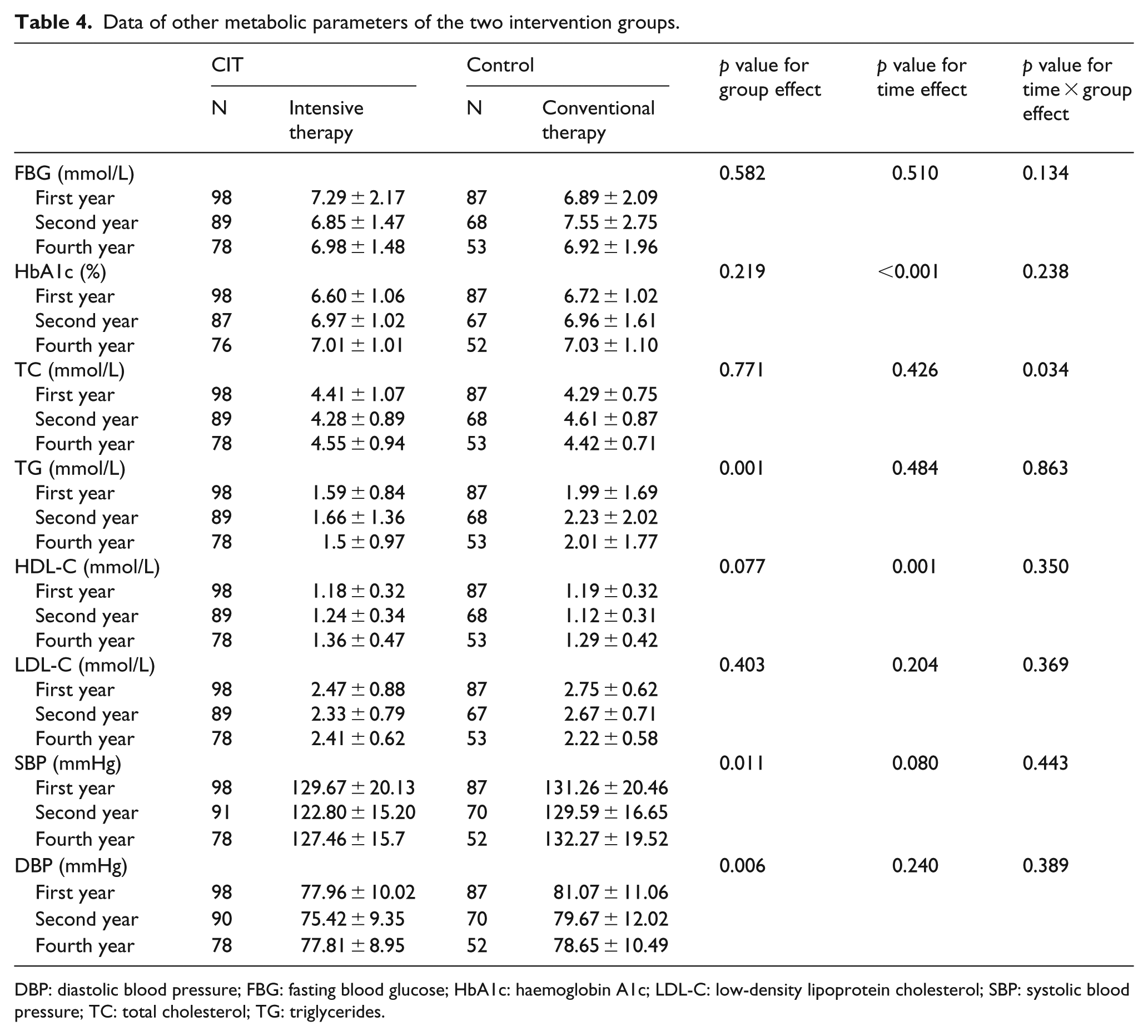
DBP: diastolic blood pressure; FBG: fasting blood glucose; HbA1c: haemoglobin A1c; LDL-C: low-density lipoprotein cholesterol; SBP: systolic blood pressure; TC: total cholesterol; TG: triglycerides.
Literature review
We performed a literature review to evaluate reported data of published studies that assessed the effects of multi-disciplinary intensive therapies on cIMT in patients with newly diagnosed type 2 DM. Our initial search identified 22 potential studies, 17 of which were excluded for not being relevant or not providing outcomes of interest (Figure 1). Two studies14,20 were excluded for being the same study as the others. The remaining three studies were included in the systematic review.13,15,16
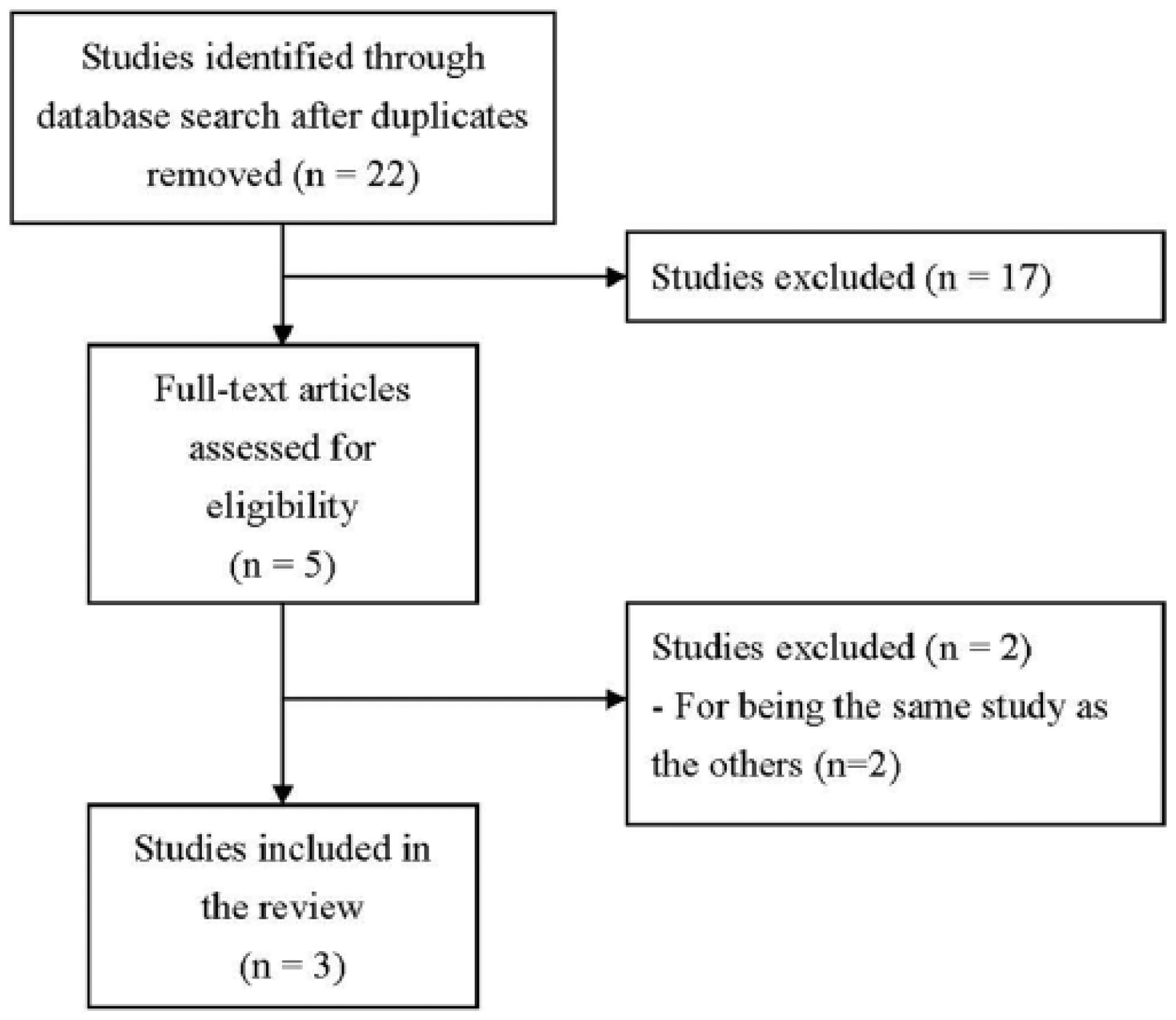
Study selection flow chart.
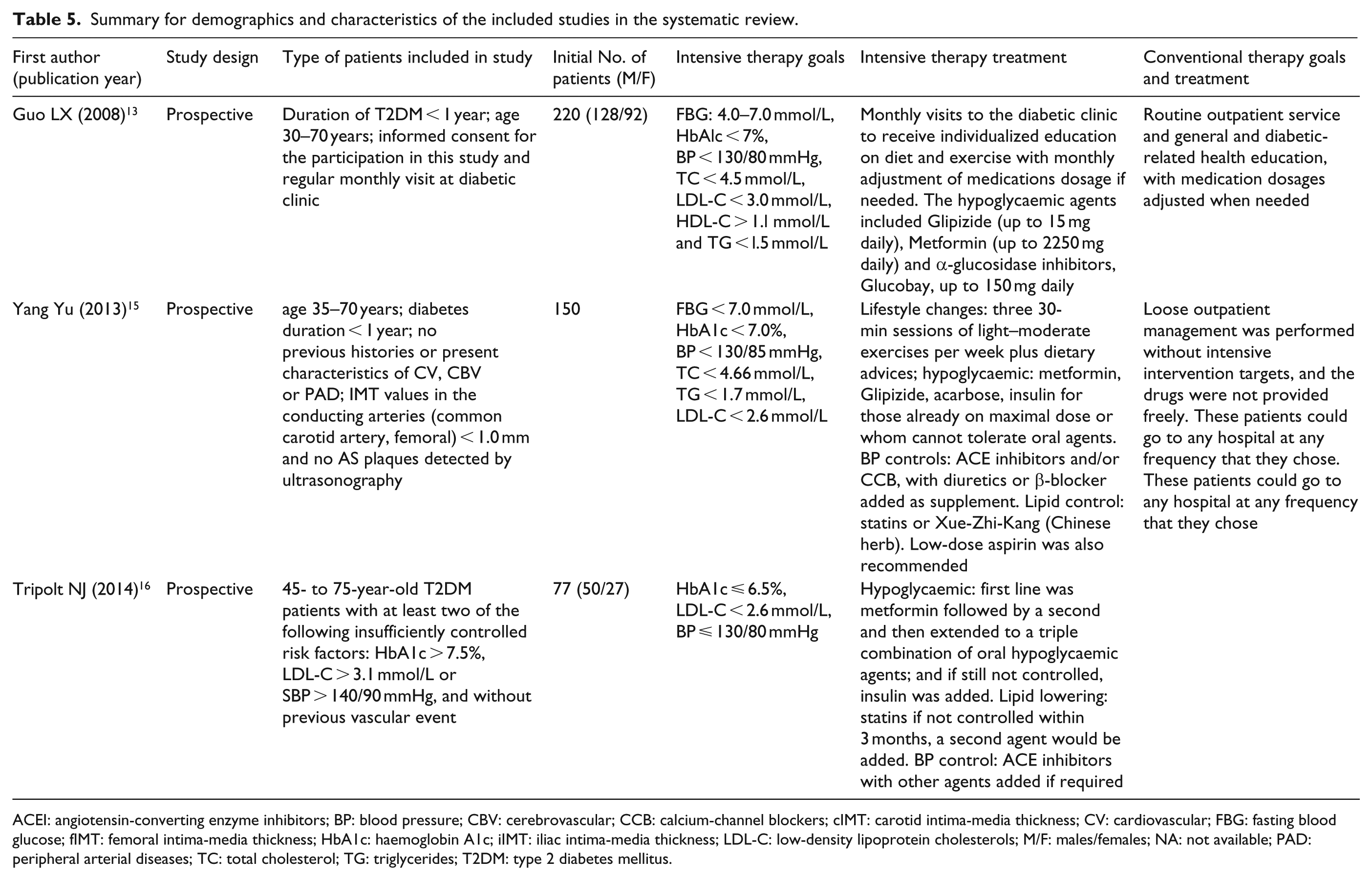
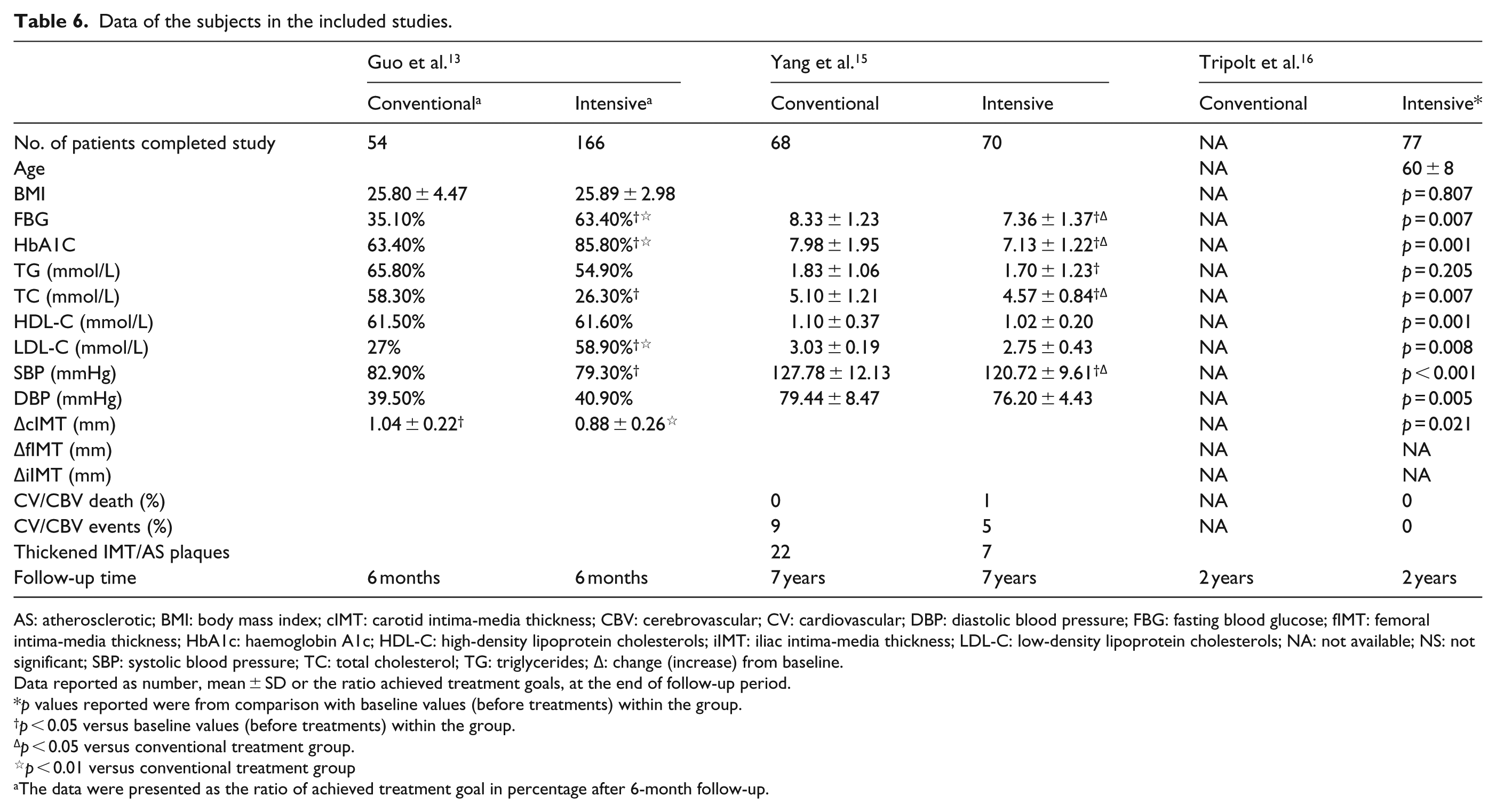
The study of Guo et al. 13 randomly assigned 220 patients who were diagnosed with type 2 DM within 1 year to receive either intensive multi-therapy (n = 166) or conventional (n = 54) therapy, and these patients were followed for 6 months. In both groups, patients were coached on a healthy lifestyle. The study found that the percentage of patients (%) who achieved treatment goal in intensive multi-factorial treatment group was significantly greater than that in conventional treatment in serum levels of FBG, HbA1C and LDL-C after 6-month follow-up (all p values <0.05) (Table 6). In addition, in this study, cIMT thickening in intensive multi-factorial treatment group (0.88 ± 0.26 mm) was significantly less than that in conventional therapy (1.04 ± 0.22 mm) after 6-month follow-up (p values <0.01). 13
Yang et al. 15 performed prospective 7-year study that assessed the changes in a number of diabetes-associated risk factors in Chinese patients with newly diagnosed type 2 DM (n = 138) who either received conventional therapy (n = 68) or an intensive multi-factorial integrated therapy (n = 70). The multi-factorial integrated therapy targeted hyperglycaemia, hypertension and dyslipidemia. Subjects were about 50 years of age and there were a similar number of males and females (Table 5). They found that intensive therapy was associated with significantly greater reductions in FBG, HbA1C, TC serum levels and SBP compared with conventional treatment (all p values <0.05) (Table 6). No difference was observed between treatment groups for changes in HDL-C, LDL-C level and DBP. There were 22 patients in the conventional therapy group who developed thickened IMT (defined as cIMT > 1.0 mm) or atherosclerotic (AS) plaques over the course of 7 years, compared to only seven patients in the intensive therapy group who developed thickened IMT/AS plaques (Table 6).
Summary for demographics and characteristics of the included studies in the systematic review.
ACEI: angiotensin-converting enzyme inhibitors; BP: blood pressure; CBV: cerebrovascular; CCB: calcium-channel blockers; cIMT: carotid intima-media thickness; CV: cardiovascular; FBG: fasting blood glucose; fIMT: femoral intima-media thickness; HbA1c: haemoglobin A1c; iIMT: iliac intima-media thickness; LDL-C: low-density lipoprotein cholesterols; M/F: males/females; NA: not available; PAD: peripheral arterial diseases; TC: total cholesterol; TG: triglycerides; T2DM: type 2 diabetes mellitus.
Data of the subjects in the included studies.
AS: atherosclerotic; BMI: body mass index; cIMT: carotid intima-media thickness; CBV: cerebrovascular; CV: cardiovascular; DBP: diastolic blood pressure; FBG: fasting blood glucose; fIMT: femoral intima-media thickness; HbA1c: haemoglobin A1c; HDL-C: high-density lipoprotein cholesterols; iIMT: iliac intima-media thickness; LDL-C: low-density lipoprotein cholesterols; NA: not available; NS: not significant; SBP: systolic blood pressure; TC: total cholesterol; TG: triglycerides; Δ: change (increase) from baseline.
Data reported as number, mean ± SD or the ratio achieved treatment goals, at the end of follow-up period.
p values reported were from comparison with baseline values (before treatments) within the group.
p < 0.05 versus baseline values (before treatments) within the group.
p < 0.05 versus conventional treatment group.
p < 0.01 versus conventional treatment group
The data were presented as the ratio of achieved treatment goal in percentage after 6-month follow-up.
Tripolt et al. 16 in a prospective, open label, 2-year study investigated the impact of multiple risk factor intervention on cIMT thickening in subjects with type 2 DM (N = 97) and poorly treated risk factors (i.e. HbA1C > 7.5% (58 mmol/mol and LDL > 3.1 mmol/L or blood pressure >140/90 mmHg) (Table 5). Subjects were about 60 years of age and there were about twice as many males as females. They found that at 2 years, FBG, HbA1C, triglycerides, TC, HDL and LDL, and blood pressure decreased significantly from baseline. They also found that multiple risk factor intervention was associated with a significant decrease in IMT of the carotid artery (cIMT) from baseline (0.883 vs 0.860, p = 0.021) (Table 6).
Discussion
Our study evaluated the efficacy of CIT in reducing the thickening of cIMT and fIMT in patients with newly diagnosed type 2 DM. CIT involved changes in lifestyle where physicians guided patients to perform regular exercise and promote healthy diets. It also included pharmacotherapy interventions to reduce glucose levels and blood pressure and to modulate blood lipid levels. During the 4-year follow-up period, physicians maintained communication with patients and made patients aware of the harm of the disease with an aim to increase therapy compliance. In addition, physicians adjusted the therapeutic protocol based on the findings at each scheduled examination.
We found that over the 4-year study period, the control (conventional therapy) group had a significantly greater rate of cIMT increase than that of the CIT group. The cIMT in the CIT group changed little over the course of 4 years, while the adjusted rate of change in the conventional therapy group increased by about 12.6%. The adjusted change rate of fIMT decreased by 1%–8% over the 4-year study period in the CIT group, while it increased by about 10% in the conventional therapy group. Taken together, while comparison of fIMT of two different treatments did not show significant difference, the cIMT remained stable in the group who received CIT but markedly increased in the group who received conventional therapy, indicating CIT can potentially reduce atherosclerosis in subjects with type 2 DM. Throughout the course of study, we also found that side effects such as severe hypoglycaemia, abnormal kidney/liver dysfunction and muscular soreness were not noticeably higher in the CIT group than the conventional therapy group.
Our therapeutic goals were comparable to the other studies. Among the three studies included in the review,13,15,16 two studies found that intensive multi-factorial intervention which targeted hyperglycaemia, hypertension and dyslipidemia was associated with reduced cIMT change compared with conventional therapy,13,15 and one study found intensive multi-factorial therapy reduced cIMT compared to baseline. 16 Similar to our findings, the studies of Guo et al. 13 also found with intensive multi-factorial therapy, the cIMT remained unchanged from baseline. The study of Tripolt et al. 16 was an one-arm study with slightly different therapeutic targets (lower HbA1c than the others) that found the multi-factorial therapy was associated with a decrease in thickness of the cIMT compared to the baseline (0.883 vs 0.860 mm, respectively; p = 0.021).
The prior studies also monitored changes in blood pressure, blood glucose and lipid levels.12–16 In general, the earlier studies consistently found that intensive multi-factorial treatment was associated with greater reductions in HbA1C, TC and blood pressure.12–16 These findings suggest that this approach to therapy can have positive impact on a number of risk factors. We did not assess these risk factors in our study.
Our data were based on a longer follow-up period (4 years) than most of the other prior studies (2 years or less). Although Yang et al. 15 performed a 7-year study, they used thickened cIMT (>1.0 mm) and AS plaques as the outcome, whereas our study followed the change of cIMT and fIMT over the course of 4 years.
There are several limitations to this study that should be considered when interpreting the results. The use of cIMT thickness as a marker for predicting cardiovascular events is still controversial. One meta-analysis included eight studies which represented 39,179 subjects and found that cIMT was a strong predictor of future vascular events. 18 However, a large-scale study that included 4220 individuals with diabetes found that the addition of cIMT to the Framingham risk score did not improve the cardiovascular risk prediction in this patient population. 21 Our study was 4 years in length, but longer studies may be needed to fully assess the benefit of intensive multi-factorial therapy in the long-term outcome and quality of life in patients with type 2 DM. In our study, the CITs varied across patients. But since only overall effects were observed, it is not possible to evaluate the contribution of each treatment, without subgroup analyses, to the overall findings. Moreover, the subjects were heterogeneous with regard to underlying health status and compliance to therapy which may have confounded the results.
Type 2 DM is a complex disease with concomitant risk factors for cardiovascular diseases. This study showed that CIT could slow the increase in cIMT in patients with newly diagnosed type 2 DM, but its effect on fIMT was promising but unfortunately did not reach statistical significance, so more and better controlled studies are needed in the future.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.