
Abstract
Introduction
Early-onset type 2 diabetes is a serious health concern for children and adolescents, as a significant portion of their lives will be spent controlling this disease. Poor long-term glycemic control can lead to significant morbidity, including macrovascular and microvascular complications. 1 Type 2 diabetes in children and adolescents is due to a combination of insulin resistance and relative B-cell failure. 2 Risk factors include a family history of type 2 diabetes, 3 obesity, and increased abdominal fat. 3-5
Carotid intima-media thickness (CIMT) is a marker of generalized atherosclerosis that correlates with the extent of coronary artery disease in adults and predicts future cardiovascular events. 6-8 Several studies have shown an association between increased CIMT with myocardial infarction and stroke in old and middle-aged subjects. Factors associated with increased CIMT in the adult population include hypertension, dyslipidemia, obesity, and diabetes. 9 Studies of the association of CIMT with clinical and biochemical parameters in adolescents with type 2 diabetes are scarce. The aim of this study was to identify the clinical parameters associated with increased CIMT in overweight and obese adolescents with type 2 diabetes.
Methods
The study protocol was approved by the Research Committee of Tanta University, Tanta, Egypt. Patients were enrolled from the diabetes outpatient clinic of Tanta University Hospital. Criteria for selection were: age between 12 and 19 years, body mass index above the 95th percentile for age and gender, a positive family history of diabetes, normal or high fasting C-peptide, and negative tests for islet cell antibodies. A control group of age- and gender-matched healthy subjects was also studied. All participants underwent clinical examination. Laboratory investigations included total cholesterol, low-density lipoprotein (LDL), high-density lipoprotein (HDL), triglycerides, hypersensitive C-reactive protein, and hemoglobin A1C (HbA1C; glycated hemoglobin). Insulin resistance was evaluated using the homeostasis model of assessment (HOMA) calculated as fasting glucose (mmol/L) × fasting insulin (mU/ml)/22.5. According to HbA1C, diabetic patients were divided into patients with controlled diabetes (HbA1C ≤ 6.5) and uncontrolled diabetes (HbA1C > 6.5).
Biochemical analysis
Blood samples were centrifuged within 20 minutes of collection at 4 °C. Ethylenediaminetetraacetic acid (EDTA) plasma was separated from cells immediately after centrifugation and stored at -80 °C until analyzed. Total cholesterol, triglycerides, and HDL cholesterol were analyzed using standard enzymatic methods. LDL cholesterol was calculated using the Friedewald formula. Hypersensitive C-reactive protein was measured using the immunoturbidimetric technique, as previously described in the literature. 10 The percentage of glycated hemoglobin was measured by colorimetric method using kits supplied by Stanbio Laboratory (Boerne, TX, USA). A preparation of whole blood is mixed with a weakly binding cation-exchange resin. The non-glycated hemoglobin binds to the resin, leaving HbA1C to be removed by means of a resin separator in the supernatant. 11 Plasma levels of islet cell antibodies, fasting insulin, and fasting C-peptide were measured by sandwich enzyme-linked immunosorbent assay (ELISA) method based on monoclonal antibody (DRG International, Inc., Mountainside, NJ, USA).
Carotid studies
Measurements of CIMT were performed on a common carotid artery. All participants underwent carotid duplex scanning of both carotid arteries. CIMT was evaluated using a high-resolution 7.5 MHz linear transducer in B mode (Vivid 7 ultrasound machine; GE Healthcare, Bethesda, MD, USA). Far-wall measurements were obtained. CIMT of the far wall was defined as the distance between the leading edge of the lumen-intima interface and the leading edge of the media-adventitia interface. CIMT was measured on each side at three sites (thickest point, and at sites 1 cm upstream and downstream, free from plaques) on the longitudinal views. In cases with uniform CIMT, measurements were obtained 1 cm from the bifurcation to the end of the common carotid artery. CIMT was calculated as the average of measurements from three different sites on each side. Figure 1 shows the measurement of CIMT in a patient with normal CIMT and a patient with increased CIMT.
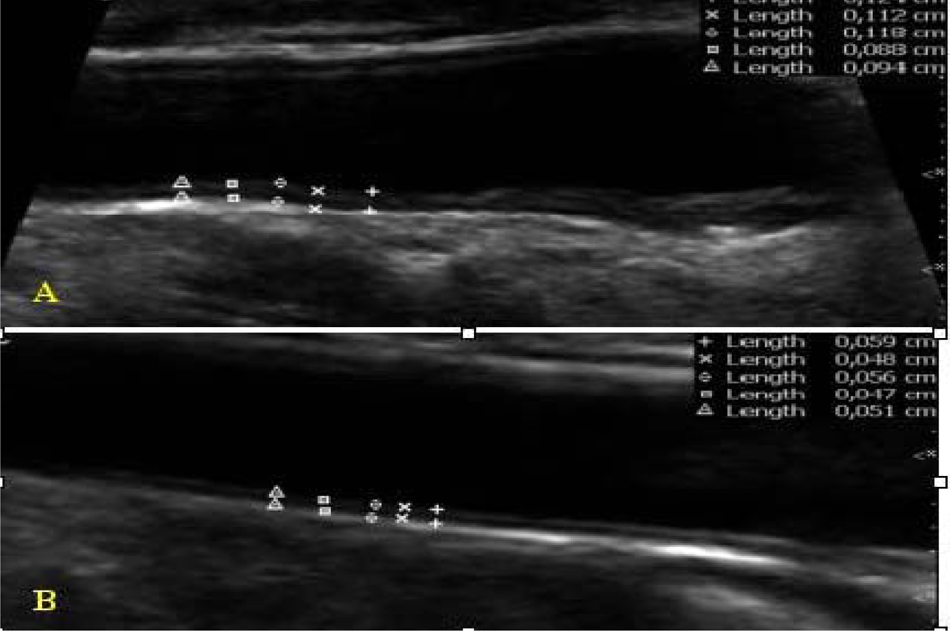
Measurement of CIMT. Panel (A) shows increased thickness. Panel (B) shows normal thickness.
Statistical analysis
Data are presented as mean ± SD. The Student’s t-test was used to compare parameters between the two groups. The ANOVA test was used to compare the data between three groups. The Tukey’s test was used to compare data between each two groups. A p value of < 0.05 was considered significant. Pearson’s correlation was used to correlate between variables. All statistical analyses were carried out using the SPSS software (version 17; IBM Corporation, Armonk, NY, USA).
Results
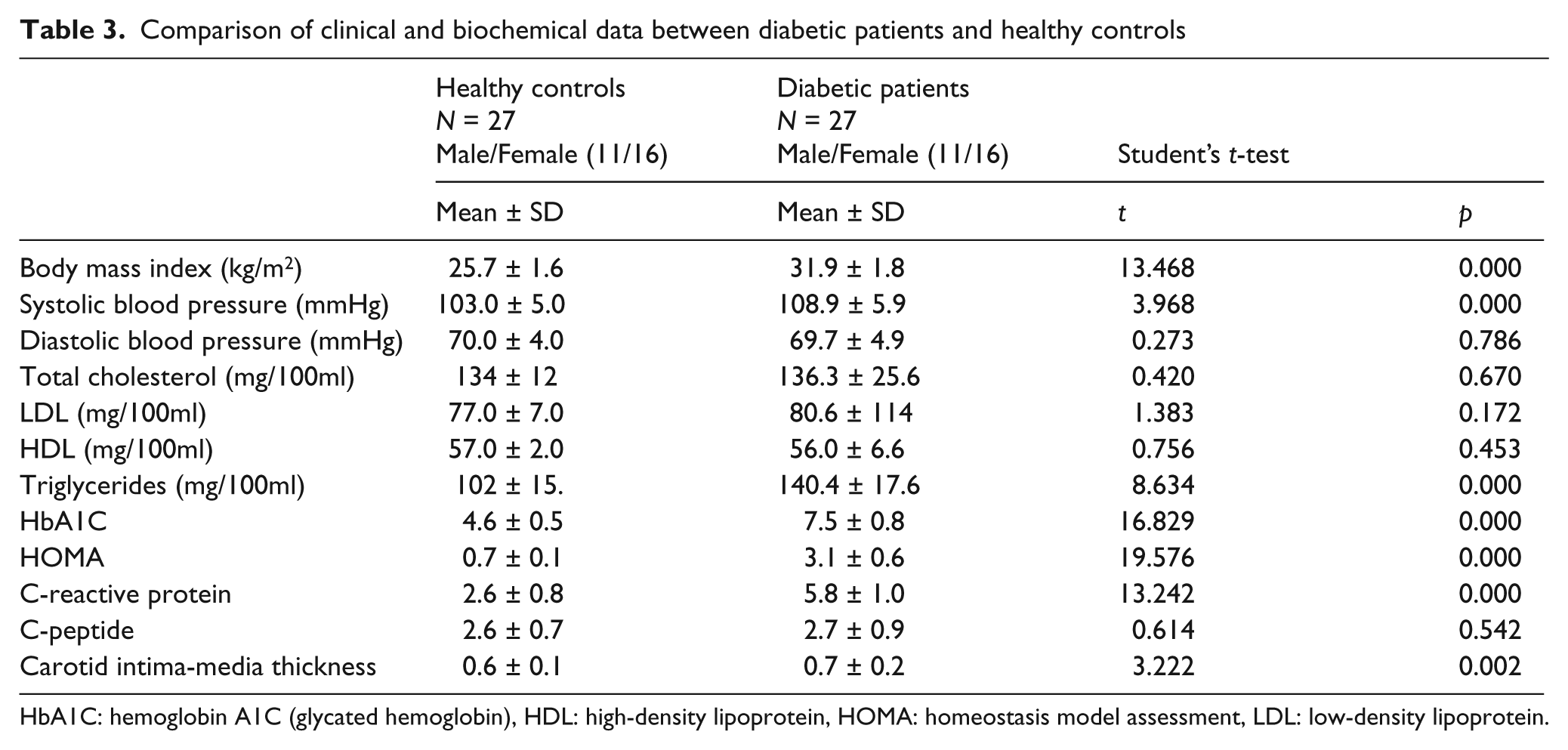
Forty-five diabetic patients were selected. Only 27 of them (16 female, 11 male) tested negative for islet cell antibodies, had a high or normal C-peptide, and represented the final population. Seven patients (26%) had a positive family history of coronary heart disease. None of the study patients was receiving medications other than insulin [short-acting insulin plus neutral protamine Hagedorn (NPH) insulin] and metformin. Insulin was indicated due to the inability to control diabetes with metformin alone. The range of HbA1C in the 15 patients with uncontrolled diabetes was 7.6–10.4 while the mean was 8.9 ± 0.9. Twenty-seven age- and gender-matched healthy adolescents were included as a control group. Table 1 shows the clinical and laboratory data for diabetic patients. Table 2 compares the clinical and biochemical data of the three groups studied. Body mass index, triglycerides, C-reactive protein, HbA1C, and HOMA were significantly increased in controlled and uncontrolled diabetic patients than in healthy subjects. CIMT was significantly increased in uncontrolled diabetic patients than in healthy subjects while there was no statistically significant difference between controlled diabetic patients and healthy subjects regarding CIMT (Figure 2). Table 3 shows the clinical and biochemical comparisons between diabetic patients and healthy controls.
Clinical and laboratory data of diabetic patients
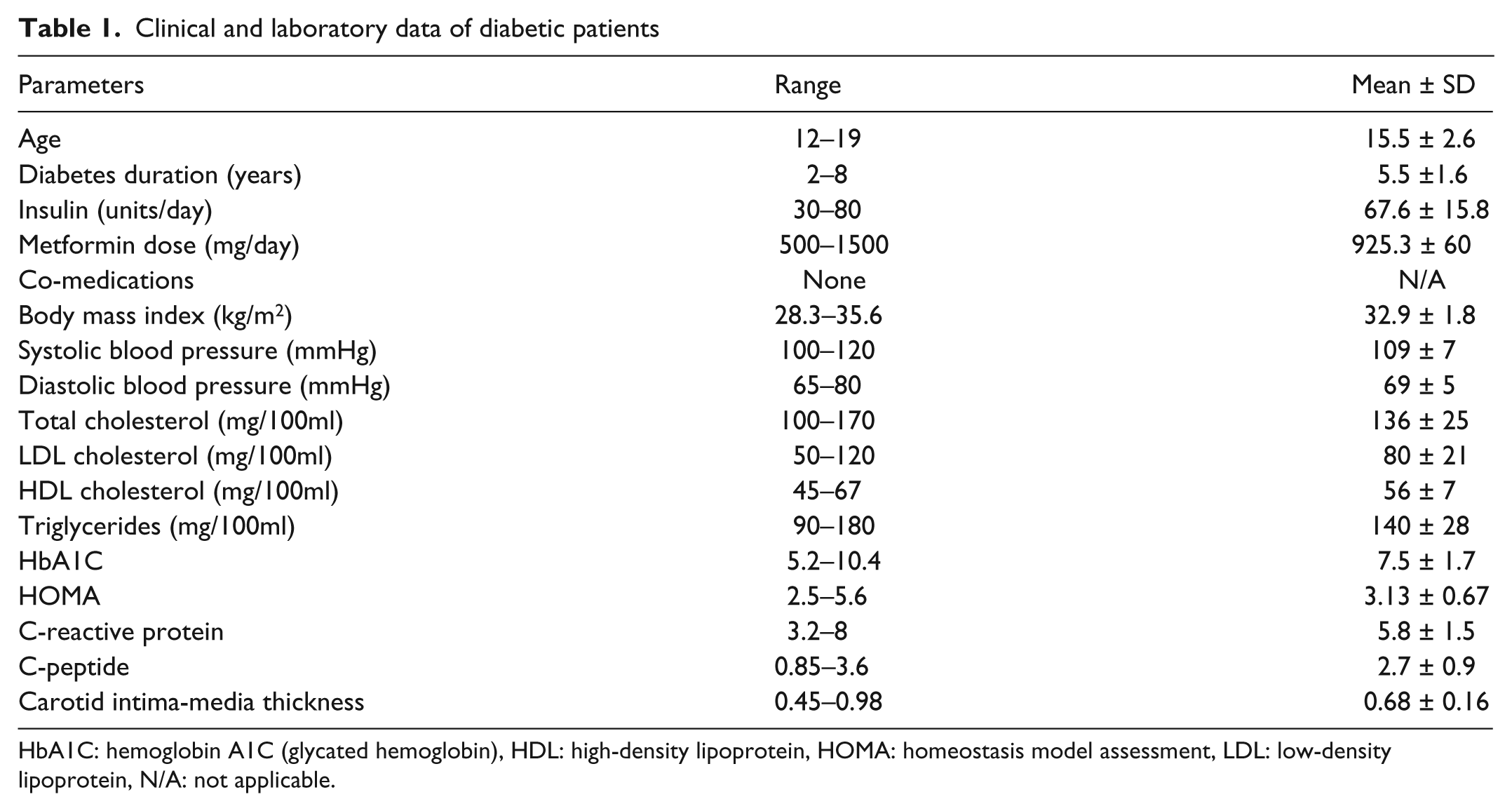
HbA1C: hemoglobin A1C (glycated hemoglobin), HDL: high-density lipoprotein, HOMA: homeostasis model assessment, LDL: low-density lipoprotein, N/A: not applicable.
Comparison of clinical and biochemical data of the study groups
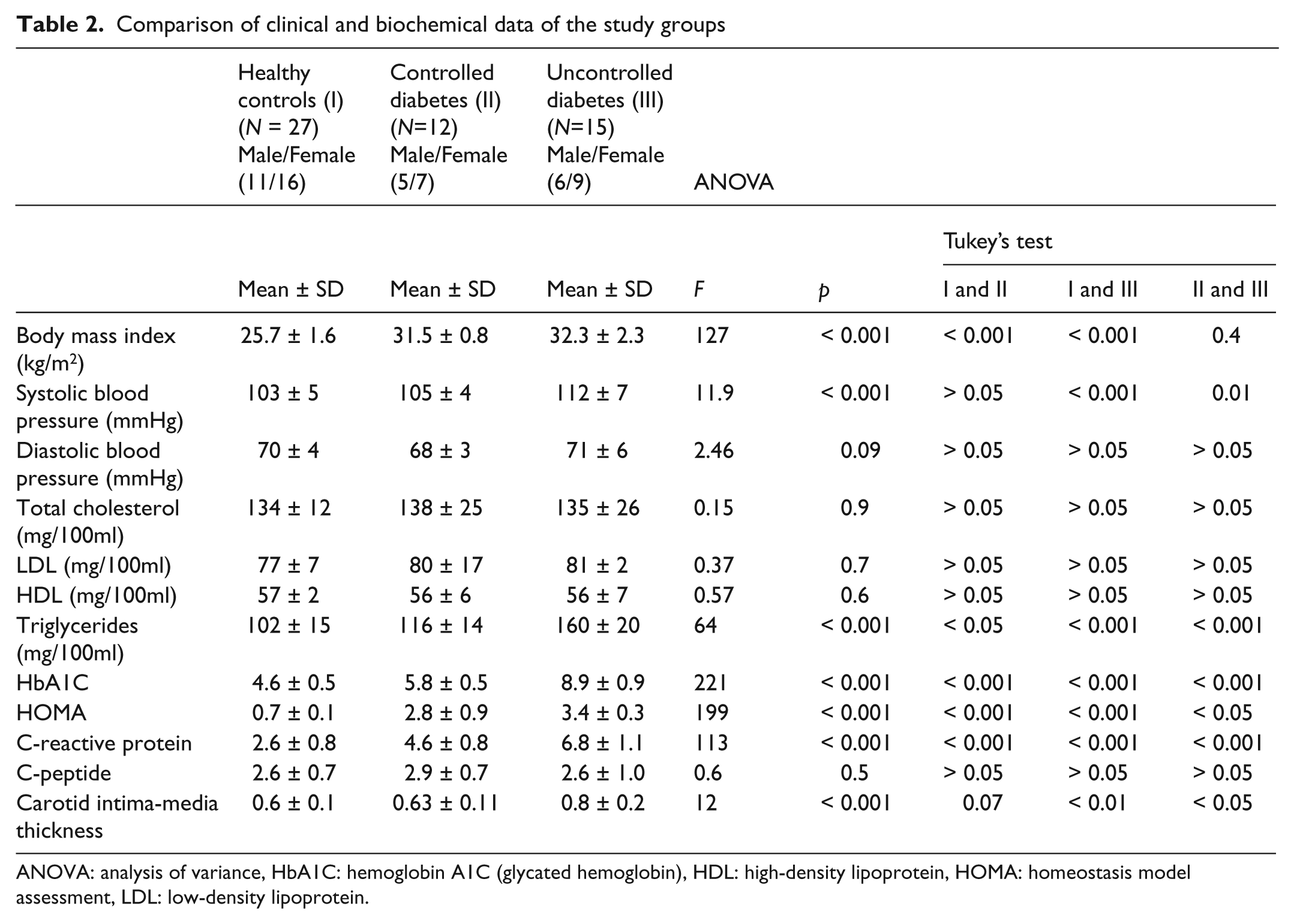
ANOVA: analysis of variance, HbA1C: hemoglobin A1C (glycated hemoglobin), HDL: high-density lipoprotein, HOMA: homeostasis model assessment, LDL: low-density lipoprotein.
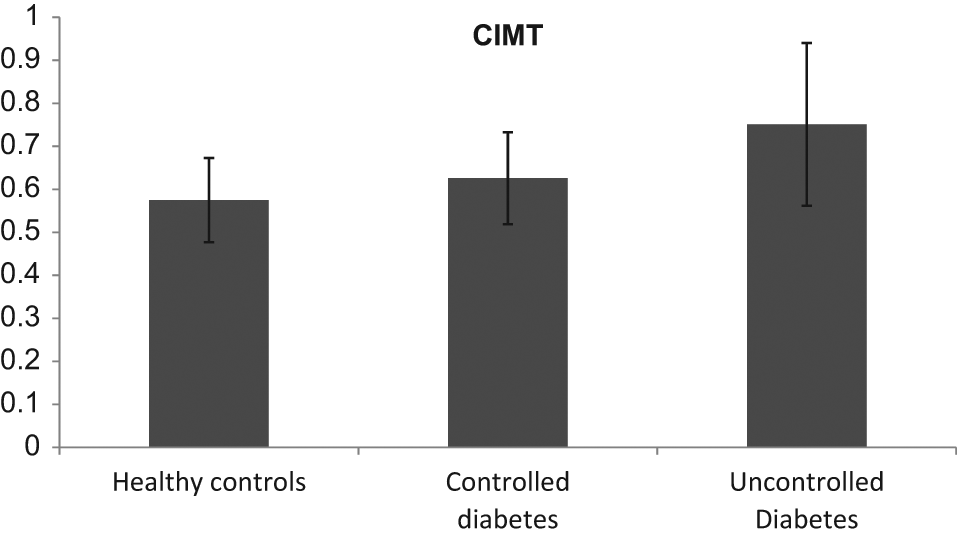
Comparison of CIMT among the three study groups.
Comparison of clinical and biochemical data between diabetic patients and healthy controls
HbA1C: hemoglobin A1C (glycated hemoglobin), HDL: high-density lipoprotein, HOMA: homeostasis model assessment, LDL: low-density lipoprotein.
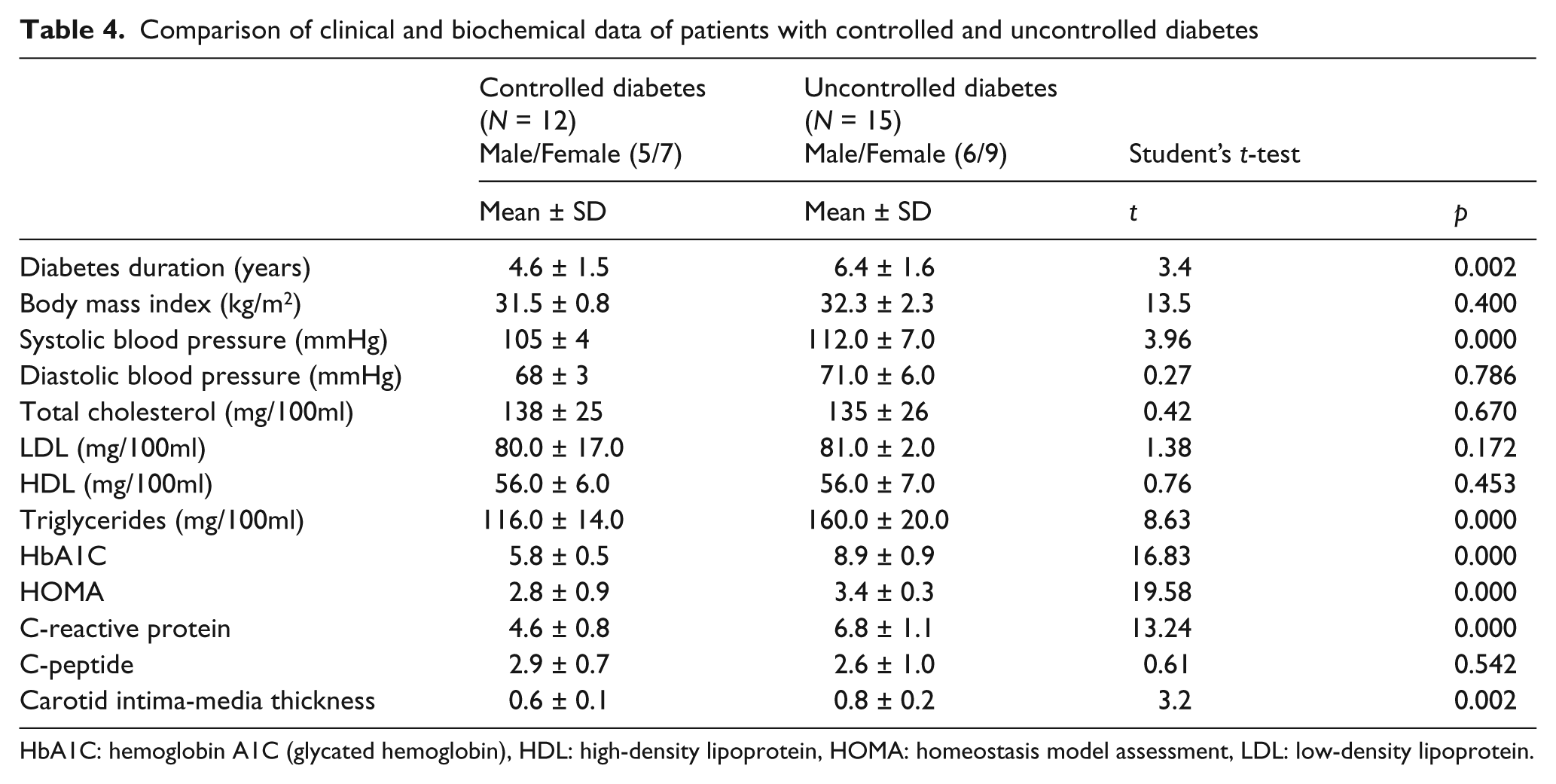
Table 4 shows the data of patients with controlled versus uncontrolled diabetes. Triglycerides, C-reactive protein, HbA1C, and HOMA were significantly higher in uncontrolled diabetic patients compared to controlled diabetic patients. HbA1C, systolic blood pressure, triglycerides, HOMA, C-reactive protein, and duration of diabetes were significantly higher in uncontrolled than controlled diabetic patients. There was no significant difference between the diabetic groups with regard to body mass index, diastolic blood pressure, cholesterol, LDL, HDL, and C-peptide (Table 4). CIMT was significantly higher in diabetic patients than in controls (Table 3) and significantly higher in uncontrolled diabetic patients than in controlled diabetic patients (Table 4). CIMT was not significantly different between patients with a family history of cardiovascular disease (0.52 ± 0.45) as compared to patients without (0.73 ± 0.14).
Comparison of clinical and biochemical data of patients with controlled and uncontrolled diabetes
HbA1C: hemoglobin A1C (glycated hemoglobin), HDL: high-density lipoprotein, HOMA: homeostasis model assessment, LDL: low-density lipoprotein.
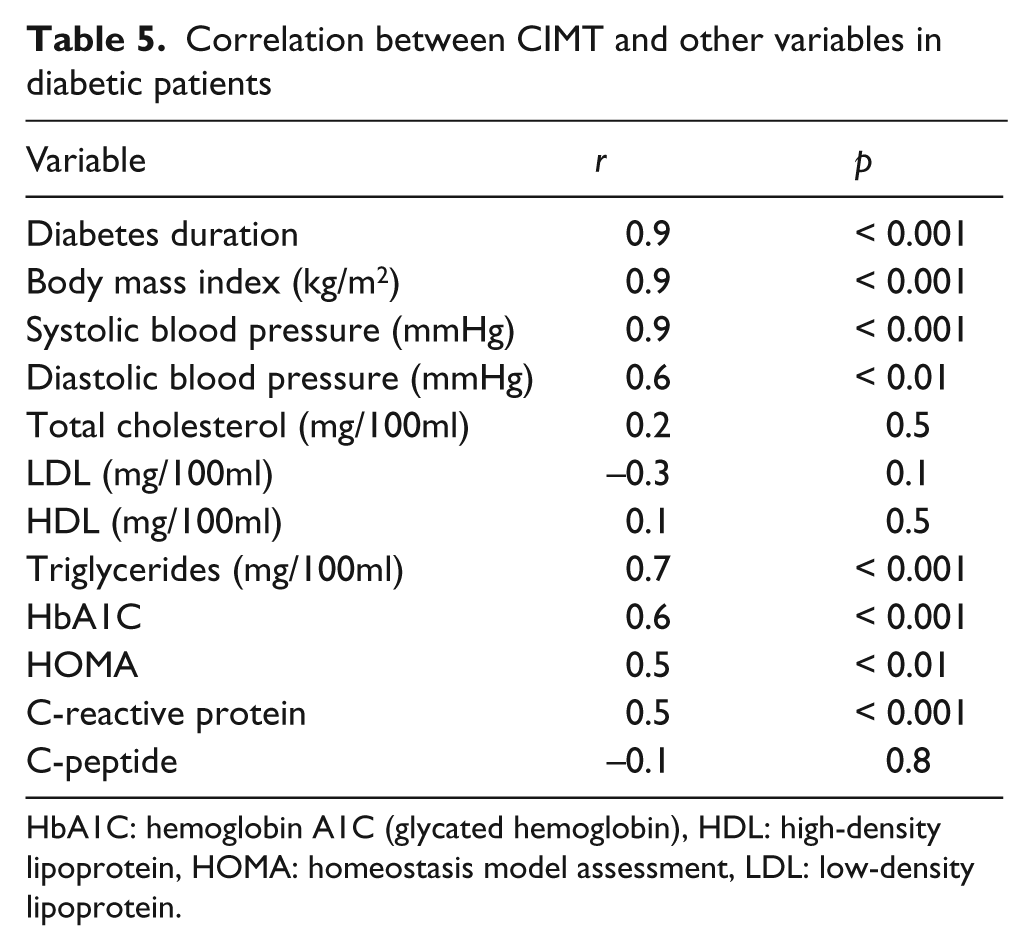
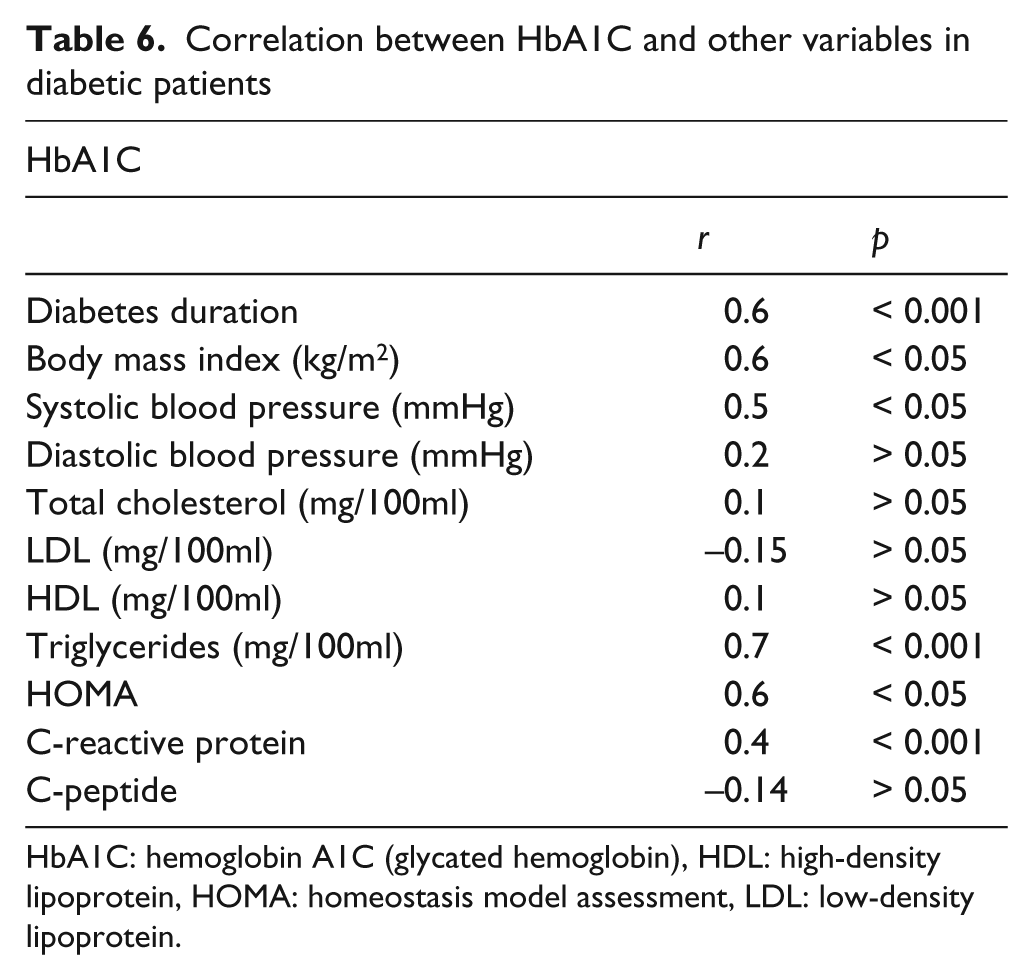
Table 5 shows the correlation between CIMT and other variables in diabetic patients. CIMT correlated positively with body mass index, systolic and diastolic blood pressure, triglycerides, HbA1C, HOMA, and C-reactive protein. CIMT correlated positively with duration of diabetes in all patients (p < 0.001). This correlation was observed in patients with controlled diabetes (p < 0.05) as well as in patients with uncontrolled diabetes (p < 0.001). There was no correlation between CIMT, age, LDL, HDL, and total cholesterol. Table 6 shows the correlation between HbA1C and other variables in diabetic patients. Figure 3 specifically shows the correlation between CIMT and HbA1C in diabetic patients. HbA1C correlated positively with body mass index, systolic blood pressure, triglycerides, HOMA, C-reactive protein, and CIMT. There was no correlation between HbA1C, diastolic blood pressure, LDL, HDL, and total cholesterol.
Correlation between CIMT and other variables in diabetic patients
HbA1C: hemoglobin A1C (glycated hemoglobin), HDL: high-density lipoprotein, HOMA: homeostasis model assessment, LDL: low-density lipoprotein.
Correlation between HbA1C and other variables in diabetic patients
HbA1C: hemoglobin A1C (glycated hemoglobin), HDL: high-density lipoprotein, HOMA: homeostasis model assessment, LDL: low-density lipoprotein.
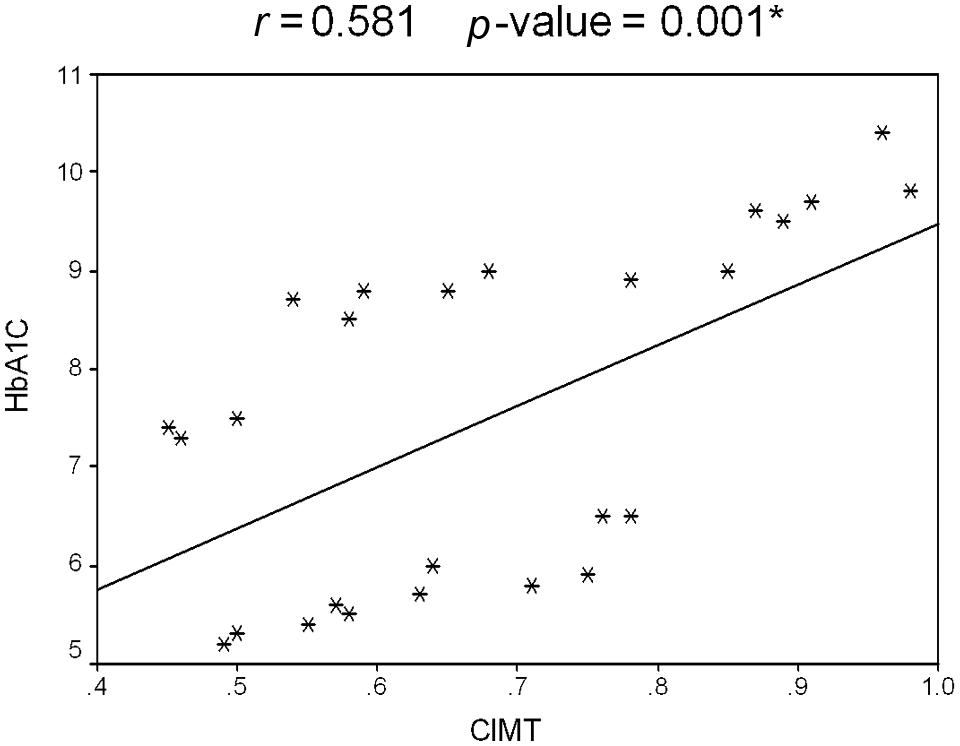
Correlation between CIMT and HbA1C in diabetic patients.
Discussion
Obesity has led to a dramatic increase in the incidence of type 2 diabetes among children and adolescents over the past two decades. Obesity is strongly associated with insulin resistance, which, when coupled with relative insulin deficiency, leads to the development of overt type 2 diabetes. Children and adolescents with type 2 diabetes may experience vascular complications at younger ages than individuals who develop diabetes in adulthood, including atherosclerotic cardiovascular disease, stroke, myocardial infarction, sudden death, renal insufficiency, neuropathy, and retinopathy leading to blindness. 12
Measurement of CIMT using high-resolution B-mode ultrasound is a well-validated, non-invasive method of assessing early cardiovascular disease. 13,14 In type 2 diabetes mellitus, CIMT is significantly higher than in corresponding healthy, age- and gender-matched non-diabetic subjects. 15,16 Although the incidence of cardiovascular disease is increasing among patients with diabetes, 17,18 the role of glycemia in this process remains uncertain. 19 Most of the data on the evolution of atherosclerosis in young diabetic patients is driven by autopsy studies. Changes in CIMT are suspected to be reversible at a young age as thickening of the carotid artery wall in younger people consists of more fatty buildup and fewer calcifications. 20 Further studies are needed to confirm this.
In the present study CIMT was significantly greater in adolescent with type 2 diabetes than in healthy subjects and correlated positively with the duration of diabetes, body mass index, systolic and diastolic blood pressure, HbA1C, HOMA, and C-reactive protein. Studies of the clinical and biochemical predictors of CIMT in young patients with type 2 diabetes are scarce. Shah et al. 20 studied 129 patients, aged 10–23, with type 2 diabetes. CIMT was related to the duration of diabetes and to levels of HbA1C. Urbina et al. 21 compared carotid arteries in young people who were either lean, obese, or had type 2 diabetes. Cardiovascular risk factors worsened from the lean to the obese to the diabetes groups. Diabetic patients had greater CIMT than that measured in lean and obese subjects for the common carotid artery and bulb. Determinants of CIMT were age, gender, and systolic blood pressure.
In our study, there was no significant difference between patients with uncontrolled diabetes, patients with controlled diabetes, and healthy controls in terms of total cholesterol, HDL or LDL, whereas triglycerides were significantly increased in the uncontrolled diabetes group than in the other groups. Although lipoproteins are important biomarkers for vascular risk, they do not completely account for the excess vascular complications in diabetes. Therefore, more recently, plasma biomarkers of inflammation and endothelial dysfunction have been investigated as possible risk factors for diabetic complications. Interleukin 6 (IL-6) and C-reactive protein are known to be increased in obesity and type 2 diabetes. 22 Our results showed a significant elevation of hypersensitive C-reactive protein in uncontrolled than in controlled diabetic patients and this correlated positively with CIMT.
Several epidemiological studies have shown that fasting hyperinsulinemia predicts cardiovascular events. 23 This was initially interpreted as evidence that insulin is atherogenic. However, because hyperinsulinemia is a reflection of an insulin-resistant state, it is now increasingly accepted that insulin resistance rather than hyperinsulinemia is pro-atherogenic. Recent data suggest that insulin has a potent anti-inflammatory effect that may inhibit atherogenesis in the long term. 24 This may also explain why insulin-resistant states may be pro-inflammatory and pro-atherogenic. In our study, HOMA was significantly higher in patients with uncontrolled than with controlled diabetes and it also correlated positively with CIMT.
Finally, in our study, HbA1C correlated positively with CIMT, body mass index, systolic blood pressure, triglycerides, HOMA, and C-reactive protein. Our results demonstrate the significant influence of quality of blood sugar control on CIMT, metabolic parameters, and the importance of effective blood sugar control.
Limitations of the study
One limitation of the study was the small number of patients. We used the HOMA test as a simple, indirect method for assessing insulin resistance, which is less accurate than the gold standard of the hyperinsulinemic euglycemic clamp. Finally, CIMT was measured manually. The use of a semi-automated ultrasound border detection program could further improve the accuracy and efficiency of measurements of CIMT.
Conclusions
CIMT is a useful tool for the early detection of atherosclerosis in adolescents with type 2 diabetes. Poor glycemic control, HOMA, increased C-reactive protein, body mass index, duration of diabetes, and elevated blood pressure are associated with early atherosclerosis in these patients.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
None declared.