
Abstract
It is unclear whether prior antidiabetic treatment affects stroke severity and outcome. To evaluate this association, we prospectively studied all patients who were admitted in our Department with acute ischaemic stroke (n = 378, mean age = 78.8 ± 6.5 years). The severity of stroke was assessed at admission with the National Institutes of Health Stroke Scale. The outcome was assessed with the modified Rankin Scale at discharge and with in-hospital mortality. A total of 123 patients had type 2 diabetes mellitus. At admission, there was a trend for lower National Institutes of Health Stroke Scale in patients treated with dipeptidyl peptidase 4 inhibitors compared with patients treated with other antidiabetic agents (6.1 ± 7.5 vs 10.0 ± 9.2, respectively; p = 0.079). At discharge, patients treated with dipeptidyl peptidase 4 inhibitors had lower modified Rankin Scale than patients treated with other antidiabetic agents (2.1 ± 1.9 vs 3.2 ± 2.1, respectively; p < 0.05). Patients treated with dipeptidyl peptidase 4 inhibitors also had lower in-hospital mortality than patients treated with other antidiabetic agents (0.0% vs 15.1%, respectively; p < 0.05). In conclusion, prior treatment with dipeptidyl peptidase 4 inhibitors in patients with acute ischaemic stroke appears to be associated with better functional outcome and lower mortality risk.
Keywords
Introduction
Type 2 diabetes mellitus (T2DM) is a major risk factor for stroke and given its rising prevalence driven by ageing and increasing obesity rates, T2DM is expected to contribute more to the global burden of stroke. 1 Moreover, stroke in patients with T2DM appears to be more severe and to result in higher rates of dependency and mortality. 2 On the other hand, preclinical data show that prior treatment with a variety of antidiabetic agents might result in less severe stroke and better functional outcome.3 –5 However, very few clinical studies assessed whether prior treatment with older antidiabetic agents (i.e. metformin, sulfonylureas or insulin) is associated with stroke severity and outcome.6–9 In addition, there are no data regarding the potential effects of the newer incretin mimetic antidiabetic agents in patients who suffer an acute ischaemic stroke.
The aim of this study was to evaluate whether prior antidiabetic treatment affects acute ischaemic stroke severity and in-hospital outcome and whether there are differences between antidiabetic agents regarding these effects.
Methods
We prospectively studied all patients who were admitted in our Department with acute ischaemic stroke between September 2010 and November 2012 (n = 378; 38.9% males, mean age = 78.8 ± 6.5 years).
At admission, demographic data, history of cardiovascular risk factors or established cardiovascular disease and pharmacological treatment were recorded. T2DM was defined as self-reported T2DM or antidiabetic treatment. Anthropometric parameters (weight, height, waist and hip circumference, waist-to-hip ratio) and systolic and diastolic blood pressure were also measured. The severity of stroke was assessed at admission with the National Institutes of Health Stroke Scale (NIHSS).
Routine laboratory investigations were performed after overnight fasting on the first day after admission and included serum levels of glucose, total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides, creatinine, uric acid and glycated haemoglobin (HbA1c). All patients underwent brain-computed tomography at admission, and a second brain-computed tomography was performed if clinically indicated. The outcome was assessed with the modified Rankin Scale (mRS) score at discharge and with in-hospital mortality.
Statistical analysis
All data were analysed with the statistical package SPSS (version 17.0; SPSS, Chicago, IL, USA). Data are presented as percentages for categorical variables and as mean and standard deviation for continuous variables. Differences in categorical variables between groups were assessed with the chi-square test. Differences in continuous variables between groups were assessed with one-way analysis of variance, and post hoc tests were performed with the Holm–Sidak test. Binary logistic regression analysis was used to identify independent predictors of in-hospital mortality. In all cases, a two-tailed p < 0.05 was considered significant.
Results
A total of 123 patients had T2DM (32.5% of the study population). Clinical and laboratory characteristics of the total study population and of patients with T2DM are shown in Table 1. The duration of T2DM was 11.2 ± 8.6 years, and HbA1c levels in patients with T2DM were 7.1 ± 1.3. Antidiabetic treatment at admission included metformin (n = 60), sulfonylureas (n = 46), dipeptidyl peptidase 4 (DPP-4) inhibitors (n = 27), insulin (n = 24), glinides (n = 4), acarbose (n = 2), pioglitazone (n = 1) and exenatide (n = 1). In total, 48 patients were on antidiabetic monotherapy [metformin (n = 15), sulfonylureas (n = 17), insulin (n = 10), DPP-4 inhibitors (n = 3), glinides (n = 2) and pioglitazone (n = 1)], 52 patients were receiving two or more antidiabetic agents and 23 patients with T2DM (18.7%) were not receiving any antidiabetic agent.
Clinical and laboratory characteristics of the total study population and of patients with type 2 diabetes treated with dipeptidyl peptidase 4 (DPP-4) inhibitors or other antidiabetic agents.
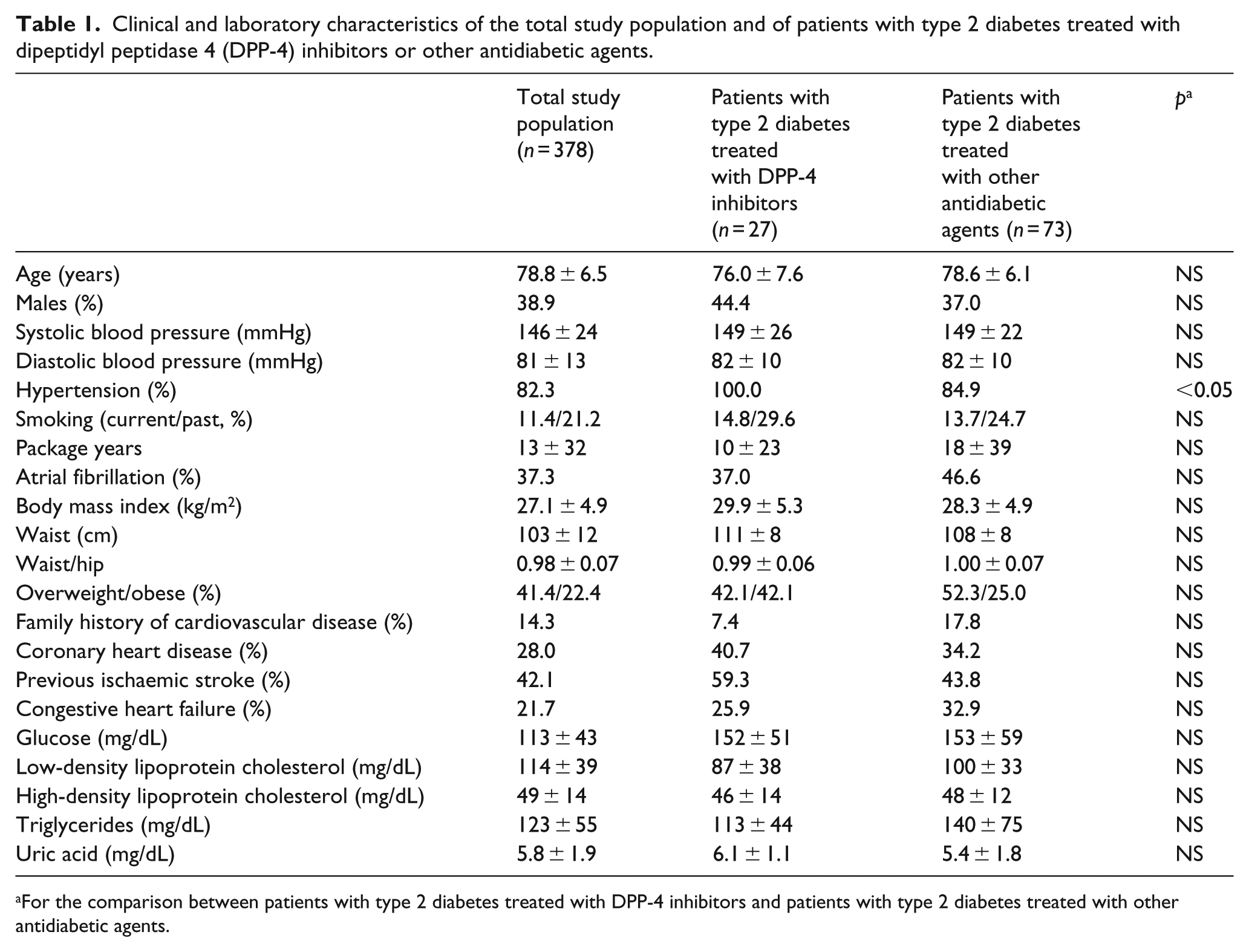
For the comparison between patients with type 2 diabetes treated with DPP-4 inhibitors and patients with type 2 diabetes treated with other antidiabetic agents.
Patients treated with DPP-4 inhibitors had higher prevalence of hypertension than patients who were treated with other antidiabetic agents (100.0% vs 84.9%, respectively; p < 0.05). Other clinical and laboratory characteristics did not differ between the two groups (Table 1).
At admission, the NIHSS did not differ between patients who were receiving monotherapy with metformin, sulfonylureas or insulin (7.1 ± 5.9, 11.5 ± 10.6 or 11.2 ± 10.2, respectively; p = NS). In contrast, there was a trend for lower NIHSS in patients treated with DPP-4 inhibitors compared with patients who were treated with other antidiabetic agents (6.1 ± 7.5 vs 10.0 ± 9.2, respectively; p = 0.079; Table 2). On the other hand, the NIHSS did not differ between patients treated with metformin and those who were treated with other antidiabetic agents (8.7 ± 9.1 vs 9.3 ± 8.8, respectively), between patients treated with sulfonylureas and those who were treated with other antidiabetic agents (8.7 ± 9.5 vs 9.1 ± 8.6, respectively) or between patients treated with insulin and those who were treated with other antidiabetic agents (10.0 ± 10.5 vs 8.6 ± 8.4, respectively).
Outcomes of patients with type 2 diabetes mellitus who were treated with dipeptidyl peptidase 4 (DPP-4) inhibitors prior to stroke compared with patients who were treated with other antidiabetic agents.
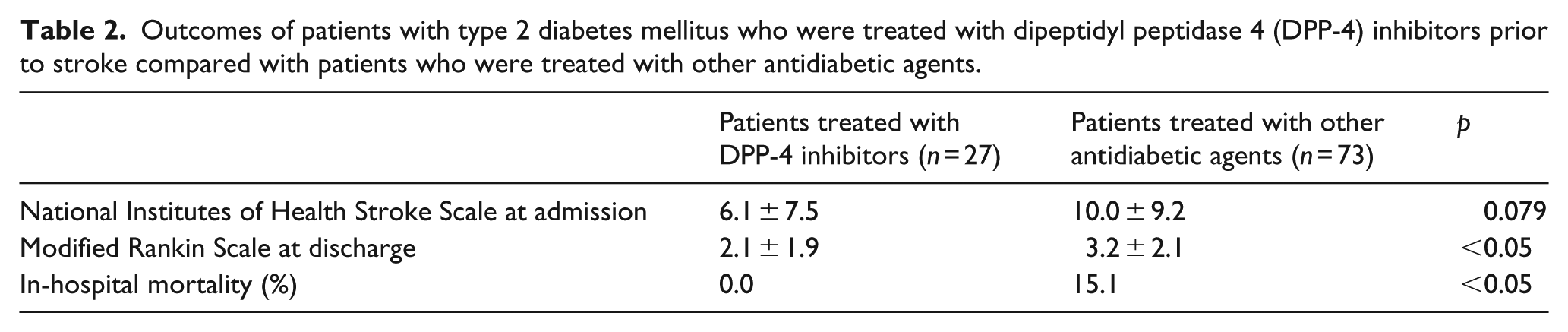
At discharge, the mRS score did not differ between patients who were receiving monotherapy with metformin, sulfonylureas or insulin (3.1 ± 2.2, 3.5 ± 2.2 or 3.3 ± 2.3, respectively). In contrast, patients treated with DPP-4 inhibitors had lower mRS score than patients who were treated with other antidiabetic agents (2.1 ± 1.9 vs 3.2 ± 2.1, respectively; p < 0.05; Table 2). On the other hand, the mRS score did not differ between patients treated with metformin and those who were treated with other antidiabetic agents (2.8 ± 2.2 vs 3.1 ± 2.0, respectively), between patients treated with sulfonylureas and those who were treated with other antidiabetic agents (2.8 ± 2.2 vs 2.9 ± 2.1, respectively) or between patients treated with insulin and those who were treated with other antidiabetic agents (2.9 ± 2.4 vs 2.9 ± 2.1, respectively).
In-hospital mortality rates did not differ between patients who were receiving monotherapy with metformin, sulfonylureas or insulin (13.3%, 11.8% or 20.0%, respectively). In contrast, patients treated with DPP-4 inhibitors had lower in-hospital mortality than patients who were treated with other antidiabetic agents (0.0% vs 15.1%, respectively; p < 0.05; Table 2). On the other hand, in-hospital mortality rates did not differ between patients treated with metformin and those who were treated with other antidiabetic agents (11.7% vs 10.0%, respectively), between patients treated with sulfonylureas and those who were treated with other antidiabetic agents (8.7% vs 13.0%, respectively) or between patients treated with insulin and those who were treated with other antidiabetic agents (20.8% vs 7.9%, respectively). Patients who died during hospitalization were also older than those who were discharged (83.6 ± 6.6 vs 77.7 ± 6.2 years, respectively; p < 0.005) and had higher prevalence of atrial fibrillation (81.8% vs 36.6%, respectively; p < 0.005) and higher NIHSS at admission (25.7 ± 8.2 vs 7.8 ± 7.6, respectively; p < 0.001). In binary logistic regression analysis, independent predictors of in-hospital mortality were age [risk ratio (RR) = 1.27, 95% confidence interval (CI) = 1.01–1.60; p < 0.05] and the NIHSS at admission (RR = 1.33, 95% CI = 1.09–1.61; p < 0.005).
Discussion
To the best of our knowledge, this is the first study that evaluated the effects of prior treatment with DPP-4 inhibitors on acute ischaemic stroke severity and outcome. The lower mortality in patients treated with DPP-4 inhibitors in our study was primarily explained by the zero mortality in this group, which is rather unusual for elderly patients with multiple comorbidities and suggests the possibility of a type I error. On the other hand, patients treated with DPP-4 inhibitors also had better functional outcome at discharge and a trend for less severe stroke at admission, suggesting the presence of a real beneficial effect of these agents. Moreover, recent preclinical data also suggest that administration of DPP-4 inhibitors before experimental stroke results in less severe stroke compared with pre-treatment with sulfonylureas.3,5 This neuroprotective effect appears to be independent of the glucose-lowering actions of DPP-4 inhibitors and might be due to the increase in glucagon-like peptide 1 (GLP-1) levels or in other substrates of DPP-4, which appear to exert neurotrophic and antiapoptotic effects on the brain. 5 On the other hand, two recent randomized placebo-controlled trials did not show any effect of DPP-4 inhibitors on cardiovascular events, including stroke.10,11 Nevertheless, stroke severity and functional outcome were not evaluated in the latter trials.10,11 Clearly, more studies are needed to evaluate whether prior treatment with DPP-4 inhibitors reduces stroke severity and improves the outcome of patients with acute ischaemic stroke.
In this study, stroke severity and outcome did not differ between patients treated with metformin, sulfonylureas or insulin. Very few studies have addressed this association and yielded conflicting results. An early small retrospective study (n = 146) did not identify an effect of prior treatment with sulfonylureas on stroke severity or outcome. 6 In contrast, another early small retrospective study (n = 61) reported more favourable functional outcomes at discharge in patients who were treated with sulfonylureas before stroke. 7 More recently, in a larger prospective study (n = 1050), patients treated with metformin, sulfonylureas or insulin prior stroke had similar stroke severity at admission and comparable functional outcomes and mortality rates at 90 days after stroke. 8 In contrast, in another recent large retrospective study (n = 4817), prior treatment with metformin or insulin was associated with lower mortality compared with prior treatment with sulfonylureas; stroke severity was not evaluated. 9 Preclinical studies that evaluated the neuroprotective potential of metformin, sulfonylureas or insulin in experimental ischaemic stroke also reported discordant results.3–5 Since current guidelines recommend that the choice of the second antidiabetic agent in patients who do not achieve glycaemic targets despite treatment with metformin should be individualized; 12 it is important to perform more studies to clarify whether DPP-4 inhibitors, sulfonylureas or insulin are more beneficial in patients who suffer an ischaemic stroke.
In conclusion, this study suggests that prior treatment with DPP-4 inhibitors in patients who suffer an acute ischaemic stroke is associated with better functional outcome and lower mortality risk compared with other antidiabetic agents, potentially through a reduction in stroke severity. On the other hand, treatment with metformin, sulfonylureas and insulin before stroke appears to have similar effects on stroke severity and outcome. However, it should be emphasized that the data reported in this study are not conclusive and that our findings are merely hypothesis generating. Larger studies will be required to fully understand the role of DPP-4 inhibitors in clinical outcome following cerebrovascular events. Ongoing trials evaluating the cardiovascular benefits of incretin-based therapies offer an excellent opportunity to address this important issue.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.