
Abstract
Background:
This study investigated whether postprandial hyperglycaemia has an adverse effect on coronary microvascular function and left ventricular diastolic function.
Methods:
In all, 28 patients with type 2 diabetes mellitus with no significant stenosis in left anterior descending artery were enrolled. In all subjects, plasma 1,5-anhydroglucitol was measured, and coronary flow reserve in the left anterior descending artery was evaluated using a Doppler wire. Membrane type-1 matrix metalloproteinase expression on circulating peripheral blood mononuclear cells was measured by flow cytometry. Correlation analyses were performed for coronary flow reserve and 1,5-anhydroglucitol, other coronary risk factors, membrane type-1 matrix metalloproteinase and E/e′.
Results:
Strong correlations were found only between 1,5-anhydroglucitol and coronary flow reserve and membrane type-1 matrix metalloproteinase. On multiple regression analysis, 1,5-anhydroglucitol remained an independent predictor of coronary flow reserve (β = 0.38, p = 0.048).
Conclusion:
Postprandial hyperglycaemia appears to have an adverse effect on coronary microvascular function, suggesting that improvement of postprandial hyperglycaemia may contribute to the improvement of coronary microvascular dysfunction.
Introduction
Postprandial hyperglycaemia (PPH) is defined as a blood glucose level greater than 140 mg/dL 2 h after eating. PPH is very often seen in diabetic patients, even those with adequate glycosylated haemoglobin (HbA1c) levels under conventional management. 1 Though increasing HbA1c levels are involved in the onset and development of diabetic macrovascular disease,2,3 data on the relationship between microvascular complications and PPH are limited. In recent prospective observational studies in Japan, PPH was a more useful predictor of diabetic retinopathy than HbA1c and was independently correlated with the onset of diabetic retinopathy, despite not being correlated with the onset of diabetic neuropathy. 4
The acute hyperglycaemia that occurs in response to an oral glucose load in patients with type 2 diabetes impairs nitric oxide release from the endothelium, which is a main mediator of endothelium-dependent vasodilatation. 5 In another study, it was shown that acute hyperglycaemia in healthy people also impaired endothelium-dependent vasodilation, 6 which causes thrombosis and an increase in soluble adhesion molecules. 7 In the postprandial state, myocardial blood volume (MBV) and myocardial blood flow (MBF) decrease significantly in diabetic patients. 8 Moreover, coronary flow reserve (CFR) is reduced in diabetes mellitus (DM) patients without coronary stenosis compared with normal subjects. 9 However, there have been few reports of clinical studies on the implications of PPH in microcirculatory disturbances, especially in coronary arteries. The purpose of this study was to clarify whether PPH has an adverse effect on coronary microcirculation.
Methods
Patient selection
For this study, 44 patients with impaired glucose tolerance (IGT) or type 2 DM who underwent coronary angiography were screened. Type 2 DM was defined as HbA1c 6.5 or more, IGT was defined as fasting plasma glucose <100 mg/dL and 2-h plasma glucose ⩾140 mg/dL and 2-h plasma glucose <200 mg/dL after the oral glucose tolerance test. Patients with any of the following were excluded from the study: (1) acute coronary syndrome, (2) acute congestive heart failure, (3) ejection fraction <40%, (4) severe renal failure, (5) severe valvular disease and (6) those judged by the attending physician as unable to be included in the study. Risk factors including age, sex, hypertension (HT) (defined as systolic blood pressure ⩾140 mmHg or diastolic blood pressure ⩾90 mmHg, or treatment with antihypertensive medication), current or prior smoking and low-density lipoprotein (LDL) levels were recorded. This study was approved by the Institutional Review Board of the University of Fukui. The patients included in the study provided informed consent for participation after the purpose and method of the study were explained to them. Of the 44 patients who consented, 16 had physiologically obstructive disease [angiographic stenosis >75% or fractional flow reserve (FFR) <0.80] 10 and were therefore excluded from this analysis; thus, 28 patients were investigated.
Study procedures
Coronary angiography and physiologic evaluation
Coronary angiography was performed by a standard technique using a 4-French coronary catheter. After administration of 3000 IU of intravenous heparin and 4 mg of intracoronary isosorbide dinitrate, a 0.014-in, pressure and Doppler flow velocity monitoring guidewire (ComboWire®; Volcano Therapeutics, Inc., San Diego, CA, USA) was advanced to the tip of the catheter, and the aortic pressure and wire pressures were equalized. Heart rate, aortic pressure, distal pressure and Doppler signals were continuously recorded during maximal hyperaemia with intracoronary bolus injection of 50 µg of adenosine in the left coronary artery. 11 FFR was calculated as the ratio of the mean distal intracoronary pressure to the mean arterial pressure at maximal hyperaemia. Microvascular function was assessed by measuring CFR. The earliest abnormality associated with coronary artery disease is the demonstration of abnormal CFR, an integrating parameter of endothelial function and vascular smooth muscle relaxation. 12 CFR was calculated from the ratio of hyperaemic/basal average peak blood flow velocity during maximal hyperaemia. 13
Measurement parameters
Plasma 1,5-anhydroglucitol
Plasma 1,5-anhydroglucitol (1,5-AG) has been proposed as a short-term marker for PPH. 14 1,5-AG, a major 6-carbon unmetabolizable dietary monosaccharide that structurally resembles glucose, is filtered and completely reabsorbed by the kidneys during periods of euglycaemia. However, if glucose levels exceed 10.0 mmol/L (the average renal threshold for glucose), plasma 1,5-AG levels fall in direct proportion to the severity of glycosuria because of competitive inhibition by glucose for renal tubular reabsorption. Thus, even in patients who are below the target range for A1C, 1,5-AG could be used to monitor PPH 15 and be useful as a surrogate measure of PPH. 16
Membrane type-1 matrix metalloproteinase
The most well-characterized membrane-type matrix metalloproteinase is membrane type-1 matrix metalloproteinase (MT1-MMP), and it has been the focus of several in vitro and in vivo studies. 17 It has been demonstrated that MT1-MMP degrades fibrillar collagens and a wide range of extracellular matrix (ECM) glycoproteins and proteoglycans. Thus, the MT-MMPs are an area of active research and are likely to play an important role in ECM degradation localized to the basement membrane and cell–cell contact points.
The expression of MT1-MMP in peripheral blood mononuclear cells (PBMNCs) was determined on a FACScan flow cytometer (Becton, Dickinson and Company, Franklin Lakes, NJ, USA) using leukocytes from heparinized whole blood. MT1-MMP expression was defined as the proportion of MT1-MMP-positive cells in CD14-positive cells. 18
Tissue Doppler measurement
To evaluate left ventricular diastolic function, the mitral annulus moving speed waveform using the tissue Doppler method was used. 19
E/e′ is the ratio of the left ventricular inflow blood flow early diastolic wave (E) and the early diastolic mitral annulus velocity wave movement (e)′ and is used as an indicator of left ventricular end-diastolic pressure. It has been reported that left ventricular end-diastolic pressure is low when E/e′ is ⩽8, and it is increased when left ventricular end-diastolic pressure is ⩾15; this ratio is widely used in clinical practice. 20
Statistical analysis
All measured values are expressed as means ± standard deviation. Spearman’s correlation coefficient was used to assess the relationships between CFR, 1,5 AG, traditional coronary risk factors ((LDL-cholesterol, incidence of HT, smoking, body mass index (BMI)) and MT1-MMP in all patients. Multivariate linear regression analysis was carried out to identify the parameters affecting CFR. Individual models were assessed for goodness of fit using R values. The p values reported are two-sided with a significance level of 0.05. SPSS software (Windows ver.20; Chicago, IL, USA) was used for all statistical analyses.
Results
Patients’ clinical characteristics
A total of 28 patients (mean age, 69.3 ± 11.0 years; 68% male) were enrolled. Cardiovascular risk factors included HT (85.7%), hyperlipidaemia (89.2%), current and previous tobacco smoking (64.3%) and BMI (24.7 ± 3.4 kg/m2).
Treatment of DM included insulin (7.1%), sulfonylurea (25.0%), α-glucosidase inhibitors (28.5%) and dipeptidyl peptidase-4 inhibitors (10.7%). Treatment of HT and hyperlipidaemia is presented in Table 1.
Patients’ characteristics.
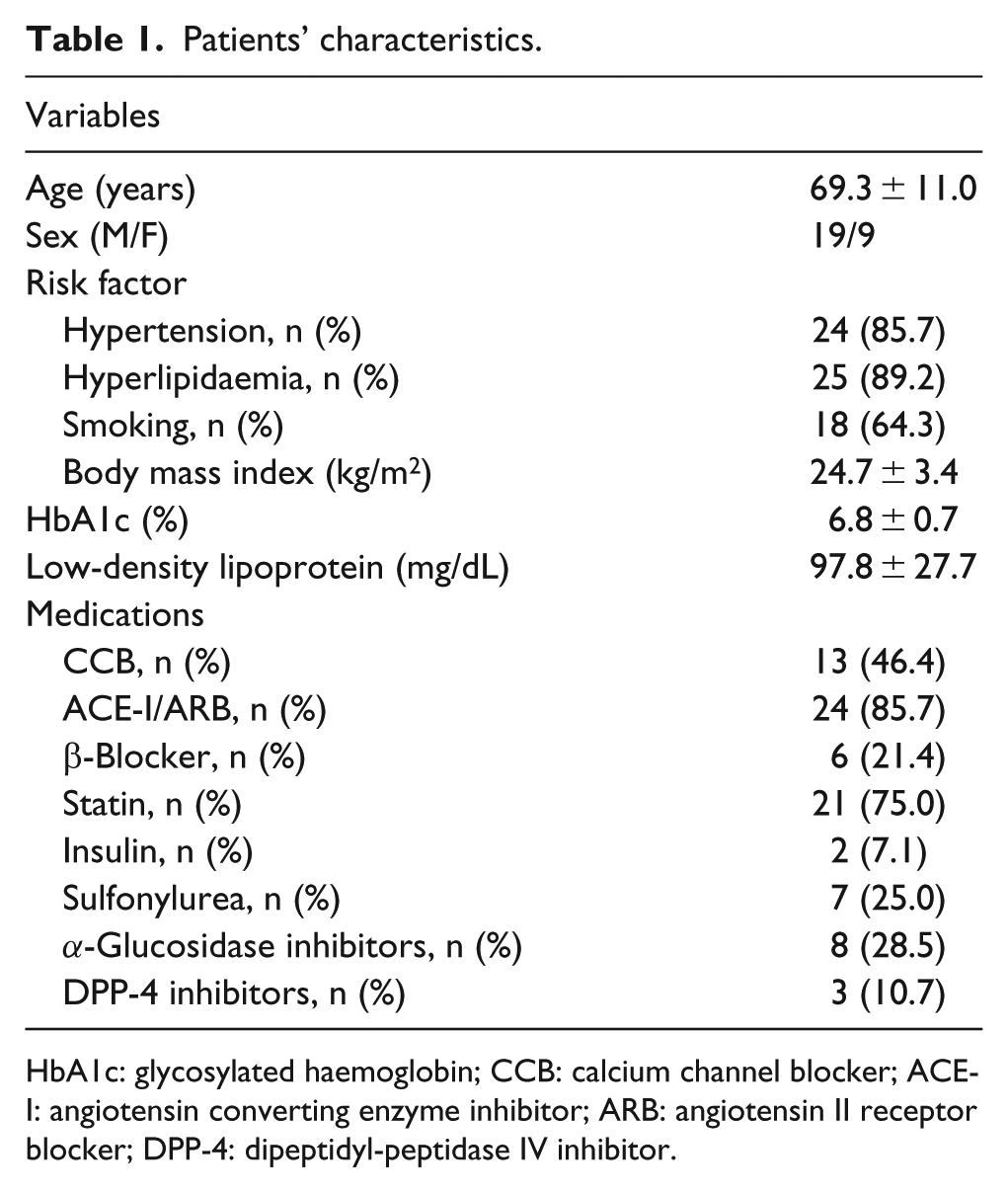
HbA1c: glycosylated haemoglobin; CCB: calcium channel blocker; ACE-I: angiotensin converting enzyme inhibitor; ARB: angiotensin II receptor blocker; DPP-4: dipeptidyl-peptidase IV inhibitor.
Measurement parameters and coronary physiological data
The data are summarized in Table 2. CFR was slightly low, and coronary endothelial function was reduced. The average E/e′ was about 15, so slight left ventricular diastolic failure was observed.
Coronary physiological data and parameters.
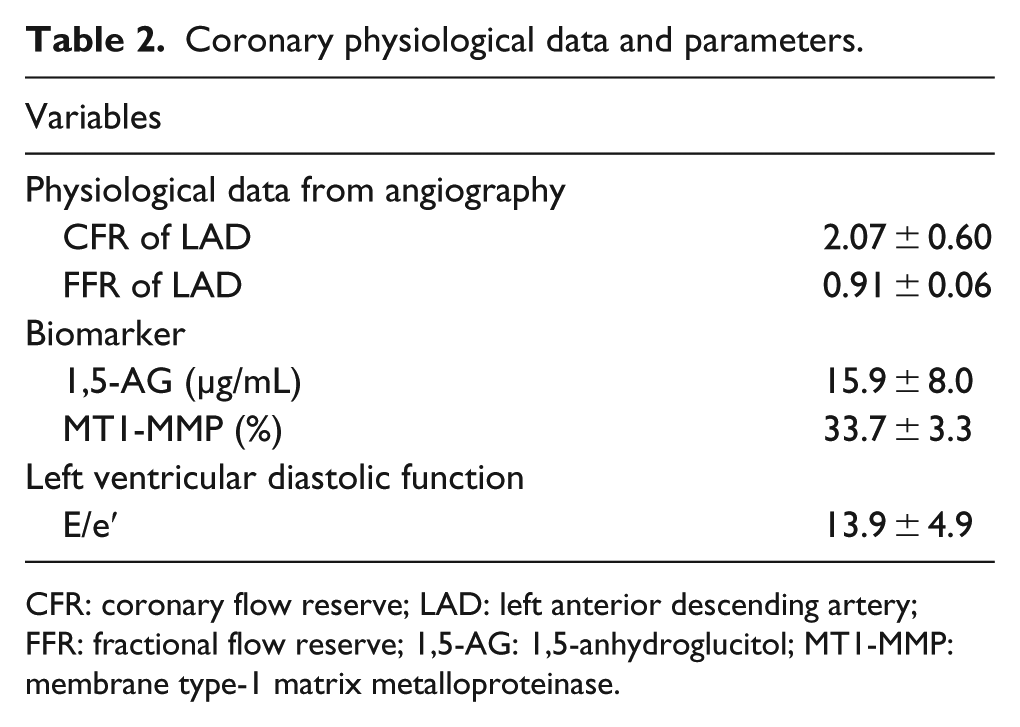
CFR: coronary flow reserve; LAD: left anterior descending artery; FFR: fractional flow reserve; 1,5-AG: 1,5-anhydroglucitol; MT1-MMP: membrane type-1 matrix metalloproteinase.
Relationship between coronary microvascular function and traditional coronary risk factors and MT1-MMP
The relationships between coronary microvascular and traditional coronary risk factors and MT1-MMP are shown in Table 4. The CFR level was positively correlated with 1,5-AG (R = 0.46, p = 0.01, Figure 1), but there was no correlation between CFR and MT1-MMP (R = −0.30, p = 0.12, Table 3). On the other hand, MT1-MMP was negatively correlated with 1,5-AG (R = −0.43, p = 0.02, Table 3).
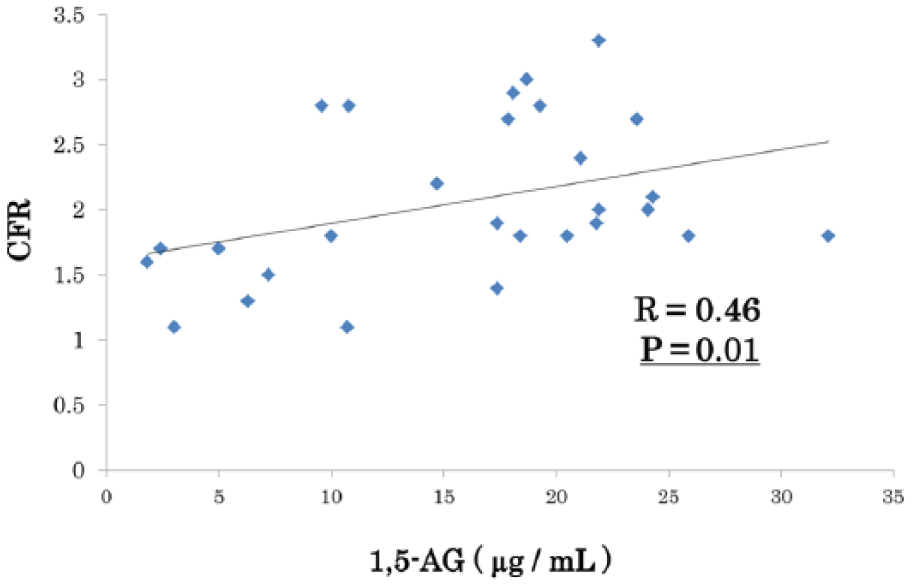
Relationship between CFR and the plasma 1,5-AG level.
Univariate relationship between microvascular function and traditional coronary risk factors and membrane type-1 matrix metalloproteinase levels.
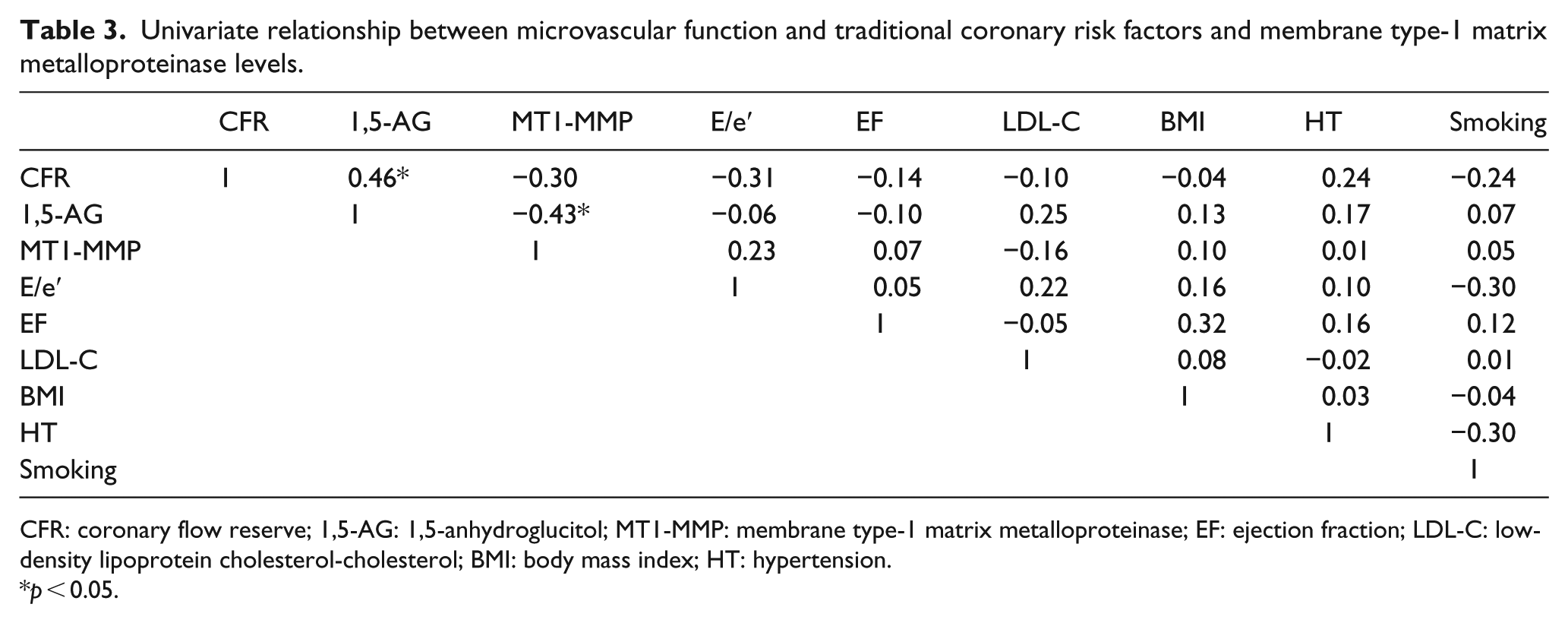
CFR: coronary flow reserve; 1,5-AG: 1,5-anhydroglucitol; MT1-MMP: membrane type-1 matrix metalloproteinase; EF: ejection fraction; LDL-C: low-density lipoprotein cholesterol-cholesterol; BMI: body mass index; HT: hypertension.
p < 0.05.
On multiple regression analysis (objective variable CFR, explanatory variables 1,5-AG, MT1-MMP), 1,5-AG remained an independent predictor of CFR (β = 0.38, p = 0.048, Table 4).
Multiple regression analysis for CFR.
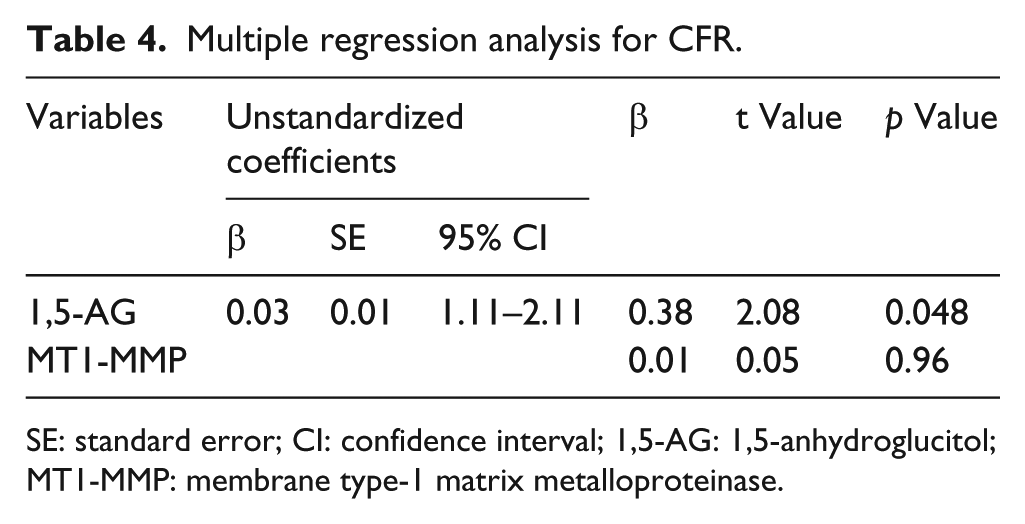
SE: standard error; CI: confidence interval; 1,5-AG: 1,5-anhydroglucitol; MT1-MMP: membrane type-1 matrix metalloproteinase.
Discussion
Major findings of this study
This study was conducted to determine whether PPH plays an important role in endothelial dysfunction of coronary arteries. In patients with DM and IGT, CFR was positively correlated with PPH, and 1,5-AG was an independent factor related to CFR on multivariate analysis. Thus, PPH may have an important impact on endothelial dysfunction of coronary arteries.
PPH and cardiovascular events and endothelial dysfunction
It has been reported that the relative contribution of postprandial blood glucose levels to overall glycaemic control is increased as the HbA1c value decreases. 21 The postprandial 2-h blood glucose level is a better predictor of all-cause mortality and cardiovascular disease than the fasting blood glucose level. 22 Furthermore, PPH may reduce the flow-mediated endothelium-dependent vasodilation (FMD) as an indicator of endothelial function by impairing nitric oxide release from vascular endothelial cells. 5 Cardiovascular events are increased in a low FMD state. 23 In addition, myocardial flow and MBF are reduced after meals in patients with type 2 diabetes. 8 From these reports, it was clear that PPH caused systemic vascular endothelial dysfunction and impaired myocardial microvascular dysfunction. In this study, coronary endothelial function was evaluated clinically by measuring CFR.
CFR and vulnerable plaque
Impaired CFR is an independent predictor of coronary events in diabetic patients. 24 In this study, whether CFR was correlated with plaque disability, possibly triggering coronary events, was evaluated using the expression of MT1-MMP in PBMNCs. The expression of MT1-MMP, which is an activated form of pro-MMP2, has an important role in ECM remodelling of human atherosclerotic plaques. 25 We have previously shown that macrophages accumulate in the shoulder region and are prone to plaque disruption in human coronary atherosclerotic plaques, and that MT1-MMP is expressed in the macrophages. 26 Thus, determining MT1-MMP expression levels on the monocyte surface is useful for the direct evaluation of unstable plaque. After treatment of DM by acarbose, which improves PPH, MT1-MMP expression in PBMNCs decreased. 18 In this study, there was no correlation between CFR and MT1-MMP expression. Therefore, CFR does not appear to be directly associated with plaque vulnerability in the early phase of DM.
Clinical implications
There has not yet been any research specifically examining the effect of management of postprandial blood glucose levels on the microcirculatory dysfunction of coronary arteries. There has been some evidence to support treatment for postprandial blood glucose levels for reducing the incidence of major cardiovascular events. The STOP-NIDDM 27 and MERIA studies 28 showed that the risk of cardiovascular events is significantly reduced when acarbose is used for the treatment of PPH. In this study, the levels of 1,5-AG, which is a short-term marker for PPH, were associated with MT1-MMP expression, suggesting that PPH is one of the mechanisms of plaque instability. Risk stratification and new targets for therapeutic intervention may be clarified by measuring 1,5-AG levels and MT1-MMP expression
Study limitations
First, the 50 µg intracoronary adenosine dose may be insufficient for the maximum hyperaemia. We determined 50 µg on the basis of 20–40 µg bolus adenosine dose in the reference, 11 but several recent articles have indicated that there might be a dose–response relationship for adenosine doses.29,30 Although the dose of 50 µg might not reach the maximum hyperaemia, we could be able to evaluate CFR adequately. 11 Second, the sample size was small, and the design was a single-centre study. It was not possible to investigate the effects of other drugs or oxidative stress markers that might be expected to affect endothelial function, such as angiotensin converting enzyme inhibitor (ACE-I)/angiotensin II receptor blockers (ARBs), statins and high-sensitive C-reactive protein (CRP), because the number of patients analyzed was too small in this study. Third, this study was an evaluation of the left anterior descending artery (LAD) alone, and it does not necessarily reflect overall microcirculatory dysfunction of the coronary arteries. Since the flow pattern of each coronary artery is different, for evaluation of coronary microcirculatory dysfunction, each coronary artery should be considered separately.
Furthermore, a cause-and-effect relationship was not established for coronary microvascular dysfunction and PPH. This mechanistic study, despite its limited size, provides hypothesis-generating data for future, larger, prospective studies.
Conclusion
In diabetic patients, PPH was found to have an adverse effect on coronary microvascular function, suggesting that improvement of PPH may contribute to the improvement of coronary microvascular dysfunction.
Footnotes
Acknowledgements
The authors would like to thank Hiromi Nishimura, Yumie Yasusaki, Motoko Oku, Mari Kurata and Yoshiko Kurose for providing excellent technical assistance and for their significant contribution to this research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.