
Abstract
We investigated the usefulness of Holter monitoring to detect cardiac disease and predict future cardiovascular risk in asymptomatic diabetic patients. This is a multi-centre, prospective study in 406 asymptomatic diabetic patients. They were categorized into three groups based on findings of Holter monitoring. A total of 377 met inclusion criteria and were classified as low (n = 172), moderate (n = 136) and high risk (n = 69). In total, 86 in moderate and 53 in high risk receive further evaluation. In total, 29 in moderate and 25 in high risk were diagnosed as cardiac disease and 12 required additional treatment, including coronary intervention. Over 1.8 years of mean follow-up, 11 (16.5 per 1000 person-years) experienced cardiovascular events. The cumulative incidence in moderate and high risk was higher than that in low risk (p = 0.029 and p = 0.014, respectively). Our study suggests that Holter monitoring may be a useful screening tool to detect cardiac disease and predict future cardiovascular risk in asymptomatic diabetic patients.
Introduction
Coronary artery disease (CAD) is a leading cause of morbidity and mortality in diabetic patients. 1 Diabetic patients without previous myocardial infarction have as a high risk of cardiovascular death and myocardial infarction as non-diabetic patients with previous myocardial infarction.2,3 Considering the specific features of diabetic CAD, a concern is that myocardial ischaemia can be silent with its first presentation of an acute coronary syndrome or a sudden death. The silent myocardial ischaemia (SMI) is two to six times more common in the diabetic patients than in the non-diabetic patients. 4 To identify CAD in diabetic patients without clear symptoms of CAD, risk factor–based approach to the initial diagnostic evaluation and subsequent follow-up is recommended.5,6 However, a recent study suggested that the conventional cardiac risk factors did not help to identify patients whose likelihood of having SMI was high. 7
Holter monitoring is a non-invasive tool for assessing the frequency and duration of silent transient myocardial ischaemia, by providing for the detection and analysis of arrhythmias and ST-segment deviation. 8 While a variety of diagnostic tests for CAD require referrals to cardiologists, Holter monitoring is available to adopt in primary care for the assessment of patients with suspected cardiac diseases by general physicians. Current evidence suggests that Holter monitoring can improve assessment of future CAD risk, particularly in patients who are post-acute myocardial infarction, those with acute coronary syndrome and in patients in the acute post-operative period. 9 There is, however, no current evidence that Holter monitoring in diabetic patients without history of cardiac disease improves future cardiac risk assessment or leads to better utilization of treatments.
The non-invasive Holter monitoring observation of new cardiac events in diabetics (NIHON) study was aimed at evaluating the usefulness of a Holter monitoring–based screening strategy for asymptomatic diabetic patients. Here, we report the results of our study.
Materials and methods
The NIHON study was a prospective, multi-centre study. A total of 406 patients with type 2 diabetes mellitus (DM) or impaired glucose tolerance (IGT) were enrolled at 28 clinics in Japan between July 2008 and July 2009.
The study recruited asymptomatic patients aged over 20 years with type 2 DM or IGT defined according to the 1999 Japan Diabetes Society criteria who had no history of organic heart disease but who did have one or more of the following risk factors: hypertension (systolic blood pressure ⩾140 mmHg or diastolic blood pressure ⩾90 mmHg; early morning home blood pressure ⩾130 mmHg systolic or ⩾80 mmHg diastolic; or use of antihypertensive medications), dyslipidaemia [low-density lipoprotein (LDL) cholesterol ⩾140 mg/dL; high-density lipoprotein (HDL) cholesterol <40 mg/dL; triglyceride ⩾150 mg/dL; or medication with lipid-lowering agents], proteinuria, diabetic nephropathy [microalbuminuria or estimated glomerular filtration rate (eGFR) ⩽60 mL/min], abdominal obesity (waist circumference ⩾85 cm in men, ⩾90 cm in women), diabetic retinopathy, diabetic neuropathy, history of cerebrovascular disease, internal carotid artery stenosis (intima-media complex ⩾1.2 mm) or peripheral artery disease (PAD; ankle brachial pressure index ⩽0.8).
This study was approved by the Institutional Review Boards of Kitano Hospital, the Tazuke Kofukai Medical Research Institute and the Institutional Review Boards at the individual collaborating physicians’ institutions, which also approved the protocol when requested. After obtaining written informed consent, baseline data were recorded including 24-h Holter monitoring.
Holter monitoring
Electrocardiograms were recorded continuously on digital storage, Holtrec (Nihon Kohden Corporation, Tokyo, Japan) with the use of two electrodes (leads CM5 and NASA). All Holter recordings were sent to a central site using Net De Holter (Morioh Co. Ltd, Morioka, Japan) via the Internet. An expert cardiologist blinded to the patient’s baseline characteristics interpreted all recordings and categorized them into the three following groups: low risk, moderate risk and high risk. These reports were overviewed by expert cardiologists in Department of EBM Research, Institute for Advancement of Clinical and Translational Science, Kyoto University Hospital.
The low-risk group included patients without abnormalities or with only mild abnormalities which did not meet the following criteria of the moderate and high risk. The moderate-risk group included patients with second-degree atrioventricular block; sick sinus syndrome, sinoatrial block, sinus arrest, sinus bradycardia or total heart beat (THB) ⩽80,000/24 h; paroxysmal atrial flutter, paroxysmal atrial fibrillation, sinus tachycardia (THB ⩾120,000/24 h) or premature atrial contractions (⩾5% of THB); premature ventricular contractions (PVCs; ⩾5% of THB) or multifocal PVCs (Lown grades 2–3); and the possibility of ischaemic ST-T changes. Ischaemic ST-T changes were defined as follows: (1) ST-segment depression at least 1 mm below the baseline ST position measured at 80 ms after the J point, (2) lasting for at least 1 min and not more than 20 min and (3) separated from other episodes by ⩾1 min. The possible ischaemic ST-T changes were defined by the presence of (1) without (2) or (3). The high-risk group included patients with third-degree atrioventricular block; sinus arrest ⩾5 min; paroxysmal atrial flutter or atrial fibrillation lasting more than 30 min, persistent atrial flutter or atrial fibrillation; frequent PVCs such as couplets or triplets, ventricular tachycardia (VT), ventricular fibrillation or R-on-T extrasystoles (Lown grades 4a and above); and heart rate–related ischaemic ST-T changes with or without long-lasting ST depression, T-wave inversion or symptoms. The definition of risk stratification was determined preliminarily by reference to Minnesota code and the guideline by the Japan Society of Ningen Dock.
Other risk stratification
We also stratified patients based on the following criteria. (1) American Diabetes Association (ADA) criteria: the ADA recommended screening for myocardial ischaemia in diabetic patients with one of the following: PAD; carotid artery disease; at least two of five cardiovascular risk factors including dyslipidaemia, hypertension, current smoking, family history of premature CAD or albuminuria. 10 (2) The French-speaking Societies for diabetes & cardiology [The French-speaking Association for the Study of Diabetes and Metabolic Diseases (ALFEDIAM)/The French Society of Cardiology (SFC)] criteria: the ALFEDIAM/SFC recommended screening for myocardial ischaemia in diabetic patients with one of the following: age over 60 years, diabetic duration over 10 years and at least two other cardiovascular risk factors, PAD, carotid artery disease or proteinuria. 6
Evaluation and follow-up
Attending physicians received a report of their patients’ results of Holter recordings including group categorizations (low, moderate and high risk) and communicated the results to the patients. Patients with moderate or high risk were referred to cardiologists for further evaluations and follow-up. Evaluation and management decisions were made according to the best-effort judgements of the cardiologists.
Cardiovascular events
The cardiovascular end point was a composite of myocardial infarction, stroke, coronary revascularization, hospitalization for heart failure, hospitalization for arrhythmias, hospitalization for angina pectoris or SMI, hospitalization for aneurysm, hospitalization for PAD or dialysis.
Statistical analysis
We summarized the baseline characteristics separately for groups (low, moderate and high risk), using means and standard deviation for normally distributed data, medians and interquartile range for non-normally distributed data and percentages for categorical data. We used the Kaplan–Meier method with a log-rank test to compare the incidence of cardiovascular events between groups. To calculate cardiac event rates, we divided the number of cardiac events by person-years of follow-up, defined as the period from the date of first visit to the date of the first event or 31 January 2011, whichever came first. We performed univariate Cox proportional hazard regression analyses to evaluate the relationships between risk classification by Holter and cardiovascular events. Statistical analyses were performed using STATA version 12.1 (STATA, Texas, USA).
Results
Characteristics
Of the 406 patients enrolled at the baseline screening, we analysed a total of 377 patients, 360 for type 2 DM and 17 for IGT. We classified them as low risk (n = 172), moderate risk (n = 136) and high risk (n = 69) based on the results of Holter recordings (Figure 1). Table 1 shows the baseline characteristics of these patients. Low-risk patients were younger, had higher HbA1c and had a higher prevalence of diabetic complications (nephropathy and retinopathy) than high-risk patients. There is no trend between high risk by ADA or ALFEDIAM/SFC criteria and the groups by Holter monitoring (p = 0.927, p = 0.392, respectively).
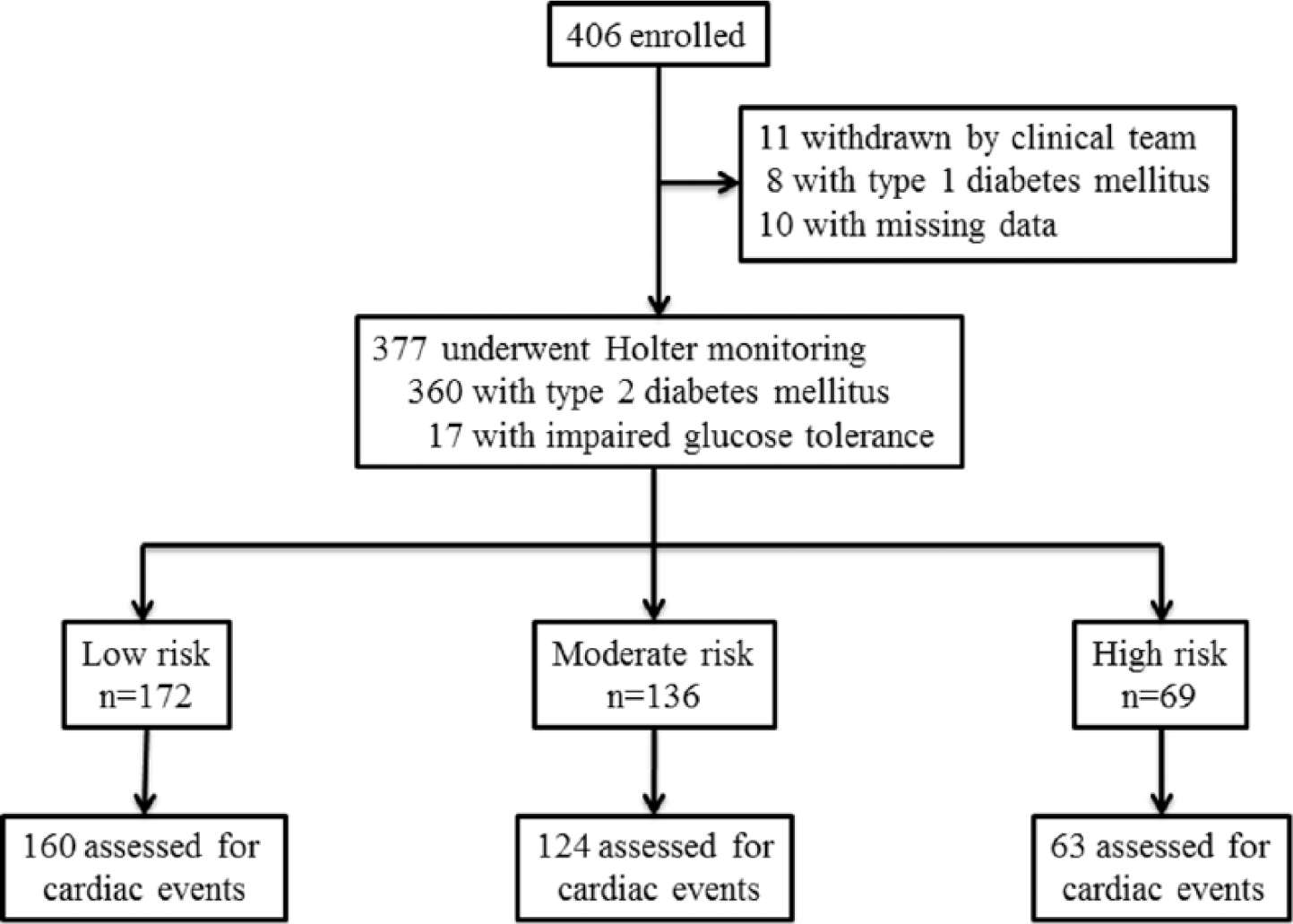
Study flow chart.
Baseline characteristics.
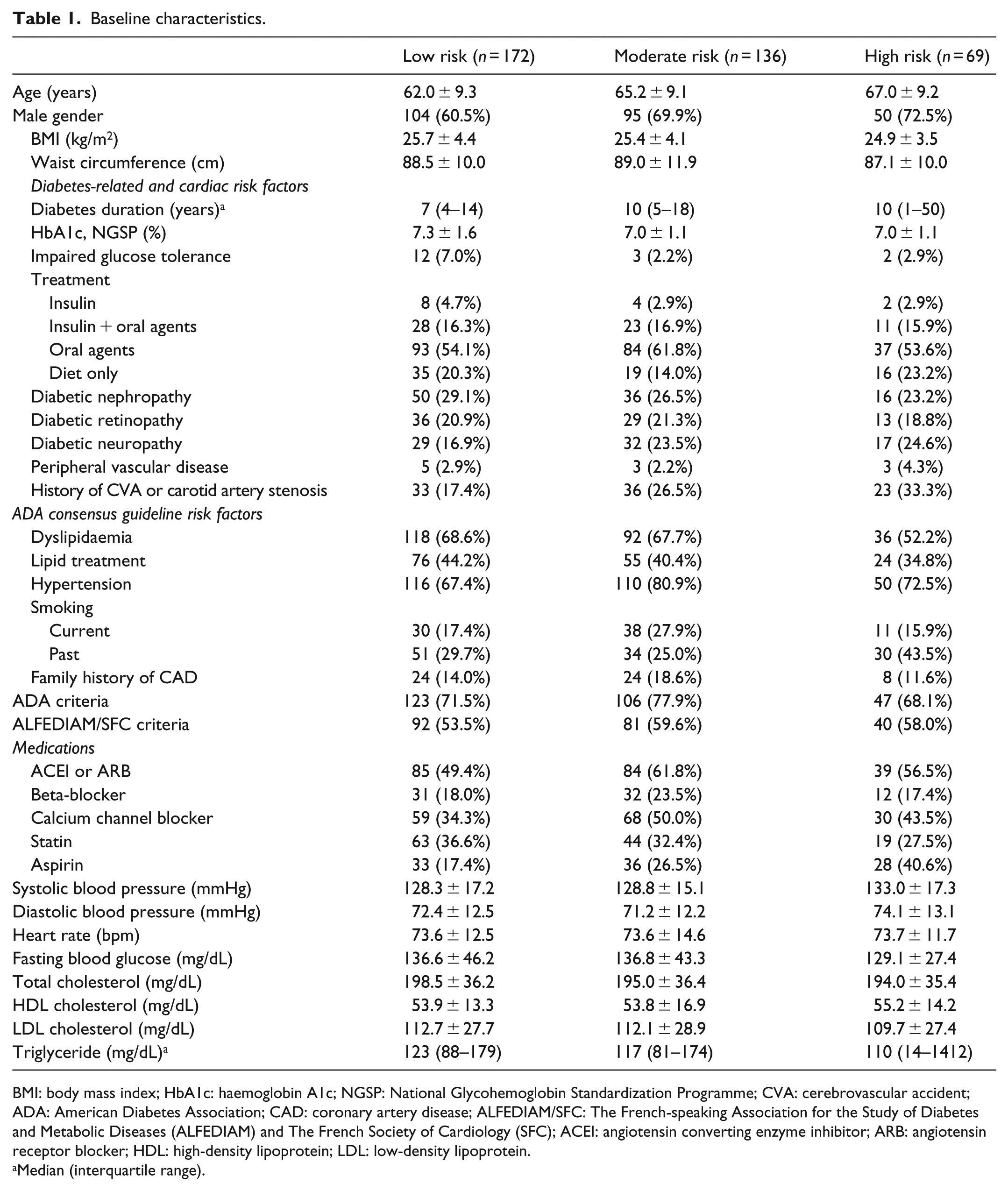
BMI: body mass index; HbA1c: haemoglobin A1c; NGSP: National Glycohemoglobin Standardization Programme; CVA: cerebrovascular accident; ADA: American Diabetes Association; CAD: coronary artery disease; ALFEDIAM/SFC: The French-speaking Association for the Study of Diabetes and Metabolic Diseases (ALFEDIAM) and The French Society of Cardiology (SFC); ACEI: angiotensin converting enzyme inhibitor; ARB: angiotensin receptor blocker; HDL: high-density lipoprotein; LDL: low-density lipoprotein.
Median (interquartile range).
Table 2 shows the detailed results of Holter recordings in patients with moderate and high risk. Both groups had high prevalence of ventricular arrhythmias (PVCs, 86.0% in moderate risk; non-sustained ventricular tachycardia (NSVT) or VT, 91.3% in high-risk patients). In addition, 16 (11.8%) patients in moderate risk and 11 (15.9%) patients in high risk had silent ischaemic ST changes on Holter recordings.
Holter recordings and subsequent diagnosed cardiovascular disease in patients with moderate risk and high risk.
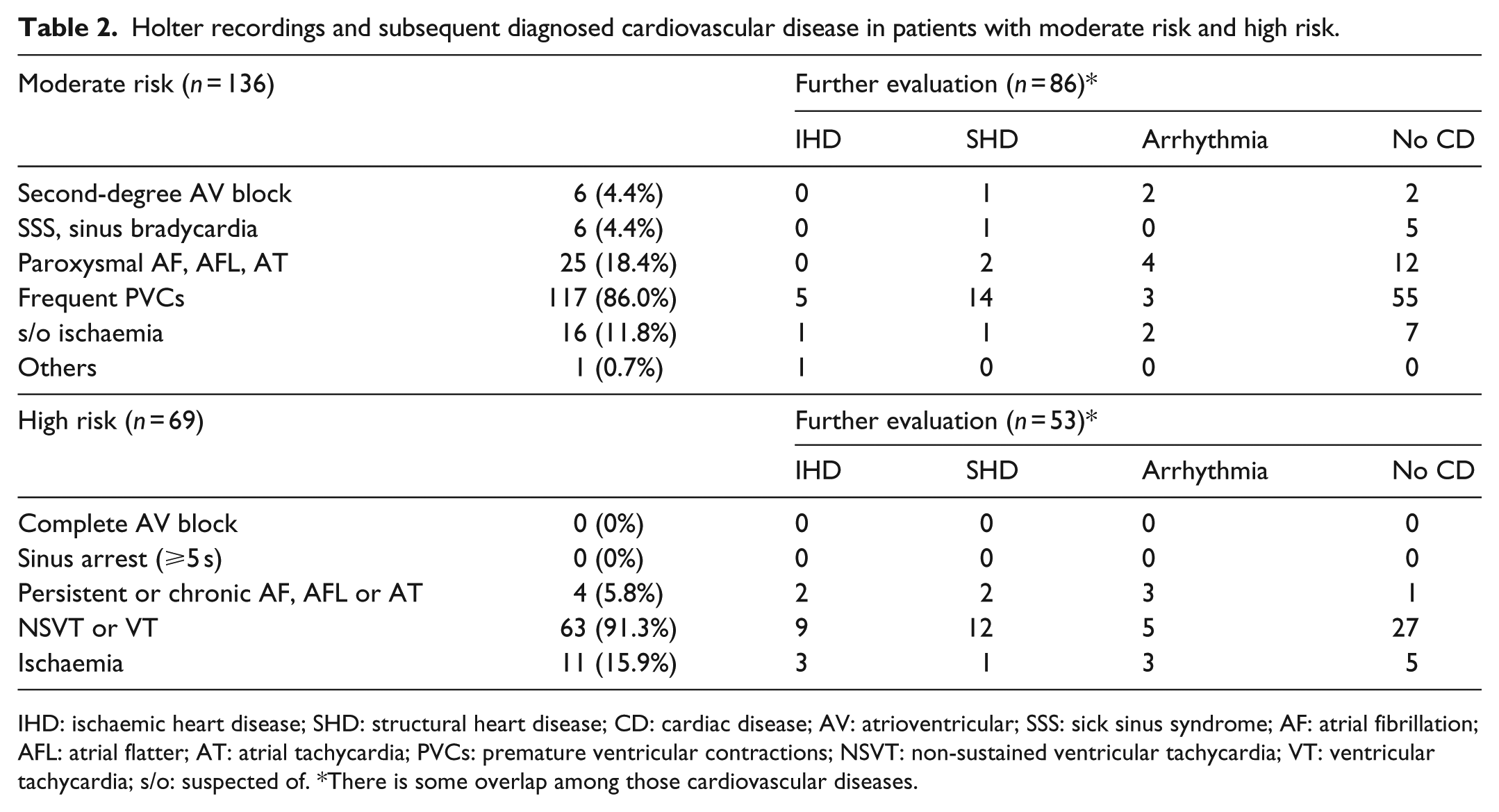
IHD: ischaemic heart disease; SHD: structural heart disease; CD: cardiac disease; AV: atrioventricular; SSS: sick sinus syndrome; AF: atrial fibrillation; AFL: atrial flatter; AT: atrial tachycardia; PVCs: premature ventricular contractions; NSVT: non-sustained ventricular tachycardia; VT: ventricular tachycardia; s/o: suspected of. *There is some overlap among those cardiovascular diseases.
Additional testing and medical treatment
In total, 86 (63.2%) patients in moderate risk and 53 (76.8%) in high risk were referred to a cardiology department during follow-up (Figure 2). Non-invasive tests were performed in 51 patients at moderate risk and in 42 at high risk (Supplementary Table 1), and 29 in moderate risk and 25 in high risk were diagnosed as cardiac disease (Table 2). In the diagnosed cardiac diseases, structural heart disease had a higher prevalence compared to ischaemic heart disease in both moderate and high risk. A total of 12 patients (5 in moderate risk and 7 in high risk) required additional treatment, including a percutaneous coronary intervention (PCI; 1 in moderate risk and 2 in high risk).
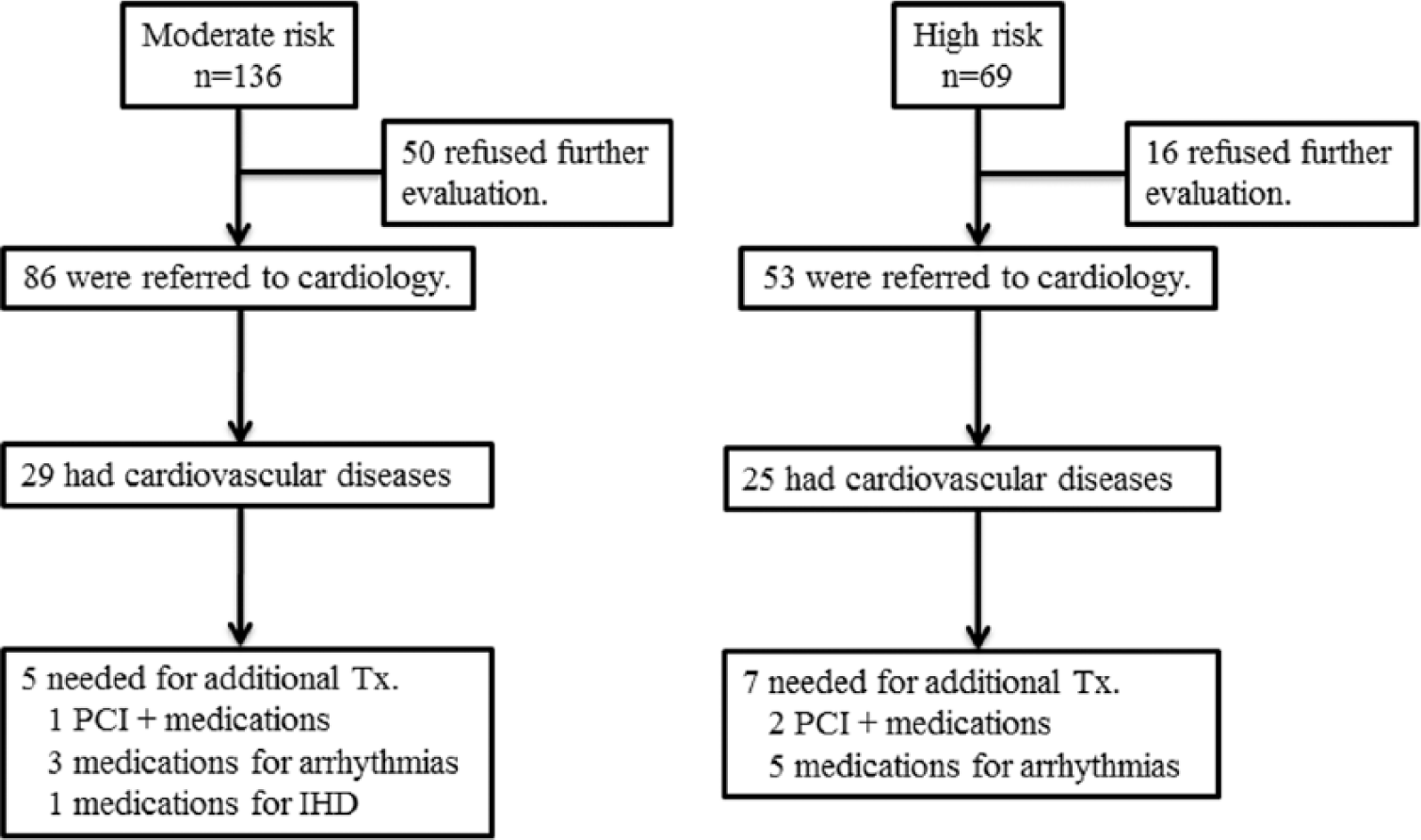
Cardiac diagnosis and additional treatments in patients with moderate or high risk.
Cardiovascular outcomes
Over 1.8 years of mean follow-up, accounting for 665 person-years, 11 patients experienced cardiovascular events (only in patients with type 2 DM): 1 at low risk (the incidence rate 3.3 per 1000 person-years), 6 at moderate risk (24.9 per 1000 person-years) and 4 at high risk (32.4 per 1000 person-years). We observed only heart disease including ischaemic heart disease, structural heart disease and arrhythmias (Table 3). The cumulative incidence was significantly higher in patients at high risk than in those at low risk (p = 0.014; Figure 3) and higher in patients at moderate risk than those at low risk (p = 0.029). Patients with high risk showed a trend towards increased cardiovascular events (p for trend = 0.028). After exclusion of IGT patients, this trend was significant in patients with type 2 DM (p for trend = 0.034). Table 4 shows clinical factors associated with cardiovascular events. We also found that age, HbA1c and diabetic neuropathy were associated with increased risk of cardiovascular events. The current two criteria (ADA and ALFEDIAM/SFC) which commonly used CAD screening in patients with diabetes were not predictors of significant cardiovascular events in our setting. The low number of cardiovascular events precluded multivariate analyses.
Cardiovascular events.

There is an overlap among those cardiovascular diseases.
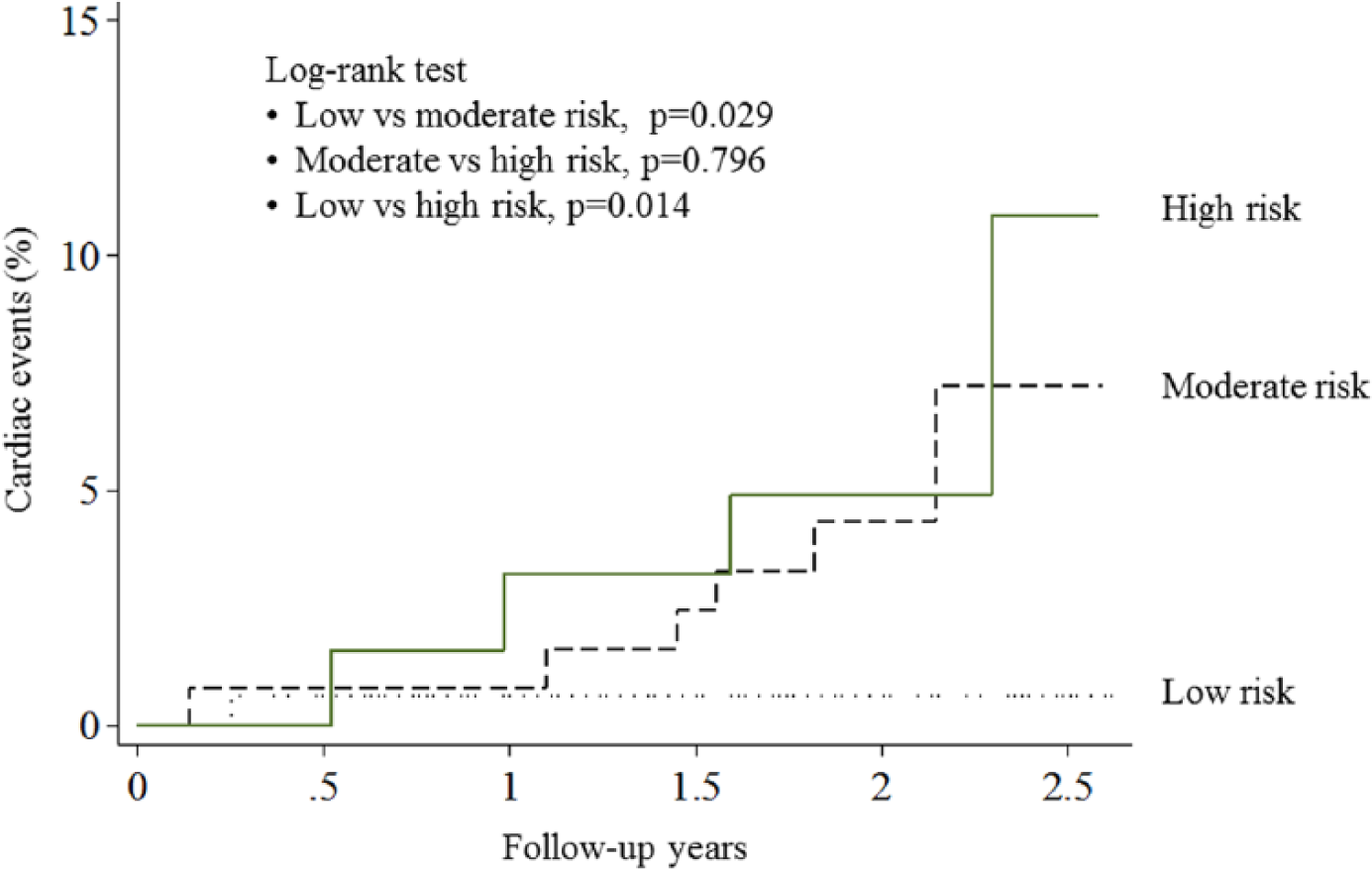
Cardiovascular events from Kaplan–Meier estimates.
Hazard ratios of cardiac events according to risk and clinical variables.
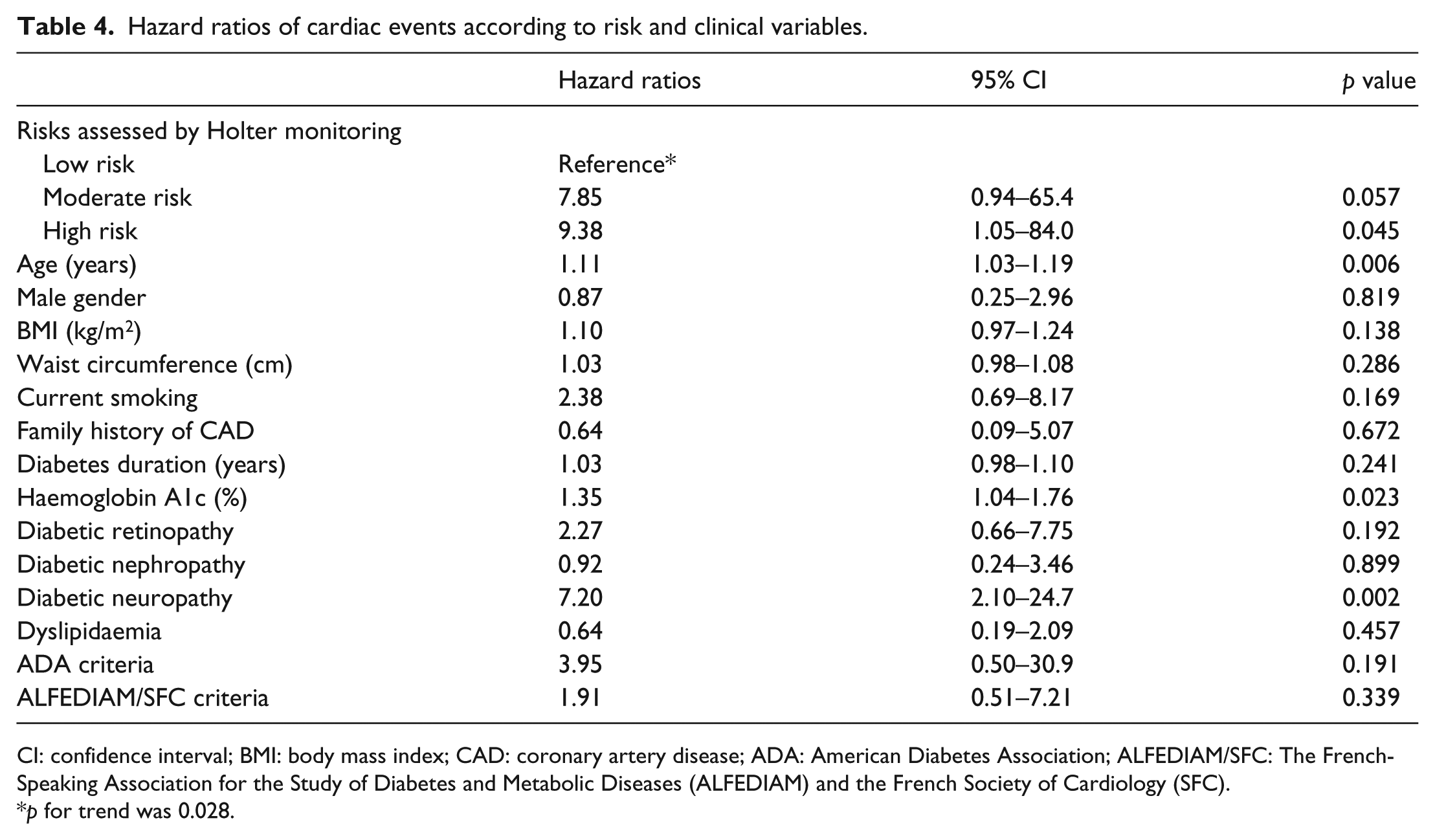
CI: confidence interval; BMI: body mass index; CAD: coronary artery disease; ADA: American Diabetes Association; ALFEDIAM/SFC: The French-Speaking Association for the Study of Diabetes and Metabolic Diseases (ALFEDIAM) and the French Society of Cardiology (SFC).
p for trend was 0.028.
Discussion
In this study, Holter monitoring detected high prevalence of abnormality including ischaemic ST changes in asymptomatic diabetic patients. Patients classified as moderate or high risk by Holter monitoring were diagnosed as cardiac disease with high frequency, and some required additional treatments including PCI. The proportions of patients who underwent the diagnosis of cardiac disease and received additional treatment were higher in the high-risk group than in the moderate-risk group. Furthermore, diabetic patients at high risk detected by Holter monitoring had a poorer prognosis than those with low risk.
The current strategy of screening patients with diabetes for advanced asymptomatic CAD is a risk factor–guided approach to identify patients with high cardiac risk whose outcomes might be improved through more aggressive intervention. 10 Both ADA and ALFEDIAM/SFC considered that multiple risk factors in the same patient substantially increase the overall cardiovascular risk 11 and that intervention directed at risk factors significantly improved cardiovascular prognosis. 12 In addition, considering the high likelihood of a positive screening test result, ALFEDIAM/SFC defined the first selection criterion for inclusion in a screening programme for SMI as age >60 years and a duration of diabetes of >10 years. 6 However, those traditional risk factors do not always predict which patients will have abnormal screening test,7,13 and negative screening tests in diabetic patients do not uniformly confer a benign prognosis.14,15 In the Detection of Ischaemia in Asymptomatic Diabetics (DIAD) study, 16 none of the current stratification schemes using conventional cardiac risk factors predicted abnormalities on screening-stress myocardial perfusion imaging (MPI), and neither the presence nor severity of MPI abnormalities was greater in the high-risk patients. Our study confirms these findings in an Asian diabetic population whose mean body mass index (BMI) at baseline was around 25 kg/m2. Together, these findings suggest that current recommendations for routine cardiovascular screening in asymptomatic patients with diabetes require reconsideration.
The very limited number of clinical trials conducted to date means that no comprehensive strategy for CAD screening in diabetic patients can be proposed.10,17 Although exercise treadmill test is recommended in asymptomatic diabetic patients or in individuals who are about to embark on moderate to high-intensity exercise,18,19 its use is limited to patients who can exercise and have a normal baseline electrocardiogram. Furthermore, many diabetic patients are obese and have additional comorbidities such as hypertension, peripheral neuropathy, PAD, decreased functional capacity and physical deconditioning – all of which may adversely influence the ability of the patient to exercise for a sufficiently long time to allow the evaluation of ischaemic changes on electrocardiography.20,21 While the clinical usefulness of several cardiac imaging for CAD detection has continued to improve over the past few years, their use is hampered by the disadvantages of radiation exposure 22 and costs and are not appropriate as an initial screening test. The DIAD study reported that among 1123 diabetic patients without symptomatic or previously recognized CAD, many of whom had two or more cardiac risk factors, MPI screening for myocardial ischaemia did not significantly reduce cardiac event rates over 4.8 years. 23 Although the coronary artery calcium score by cardiac computed tomography is a valuable marker for the overall coronary atherosclerotic burden and identifies asymptomatic individuals at higher risk for inducible ischaemia,24,25 the usefulness of screening asymptomatic moderate-risk populations is currently unknown. 26
Holter monitoring is non-invasive, inexpensive, widely available and one of the most frequently used modalities in the assessment of suspected or proven cardiovascular disease. The prevalence of SMI in diabetes as assessed by Holter monitoring varies between 35% and 58%.27–30 Although the predicted value of cardiac disease by Holter monitoring in diabetic patients is expected to be more useful than that by other non-invasive modalities, findings to date have been inconsistent.
In Asymptomatic Cardiac Ischaemia Pilot (ACIP) study, diabetic patients tended to have less measurable ischaemia during the 48-h Holter monitoring despite them having more extensive and diffuse CAD. 31 One reason for these results is that evaluation was restricted to Holter monitoring of ST-segment changes. Holter monitoring provides for the detection and analysis of two important factors, arrhythmias and ST-segment deviation. 8 In the NIHON study, we assessed both the arrhythmias and ST-segment changes, and ventricular arrhythmias detected by Holter monitoring led to the diagnosis of SMI in patients who required additional cardiac evaluations and treatments.
There are several limitations to this study and analysis. First, as not all patients in high and moderate risk had referred to cardiology, there is a possible risk of selection bias. Second, another important limitation is that an oral glucose tolerance test was not performed to diagnose IGT or newly diagnosed DM. Third, cardiovascular event rates were low due to the relatively short duration of follow-up, and the study does not have sufficient statistical power to allow for the adjustment of potential confounding factors. In our study, low-risk group had a higher HbA1c level and a higher prevalence of diabetic complications compared to moderate- or high-risk group at baseline. We need to further evaluate the associations between Holter monitoring and cardiovascular outcomes with a variety of risk factors including glycaemic control. Forth, we did not evaluate the possibility of cardiac disease among low-risk patients. One low-risk patient experienced a cardiovascular event during 1.8 years of mean follow-up, but this event rate (3.3 per 1000 person-years) was the lowest among groups. Finally, we were unable to compare the Holter screening and non-screening groups because this study was not designed to assess the hypothesis. In the NIHON study, we suggested that the potential benefits of screening by Holter monitoring would be greater for diabetic patients with at least one risk factor. Studies are needed to directly evaluate whether screening for CAD by Holter monitoring identifies diabetic patients at high cardiac risk and whether it affects clinical outcome compared with no screening.
In conclusion, Holter monitoring detected high prevalence of abnormality including ischaemic ST changes and arrhythmias and enabled to detect cardiac disease and stratify the risk of serious cardiovascular events in asymptomatic diabetic patients. These findings suggest that a screening by a combination of conventional risk factors and Holter monitoring may be advantageous to early detection of CAD and the prevention of subsequent cardiovascular events.
Footnotes
Appendix 1
Acknowledgements
Y.M.N. performed analyses and drafted the manuscript. K.U. designed the study, secured data, managed data, performed analyses and drafted the manuscript. R.N. designed the study and revised the manuscript. Y.M. evaluated the Holter recordings and revised manuscript. I.S. designed the study and secured data. S.T. secured data, managed data, performed analyses and drafted the manuscript. S.Y. secured data, managed data, performed analyses and drafted the manuscript. K.N. managed data and revised the manuscript. K.H. designed the study and revised the manuscript. Y.K. designed the study, managed data and revised the manuscript. All authors had full access to all of the data in the study. All authors approved the final manuscript. K.U., Y.M., I.S. and K.H. are stakeholders of Morioh Co. Ltd. Participation is listed in ![]() .
.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This study was financially supported by the Japan Research Promotion Society for Cardiovascular Diseases.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.