
Abstract
The effect of dapagliflozin on blood pressure was evaluated in non-hypertensive (<140 mm Hg) and hypertensive (⩾140 mm Hg) patients with type 2 diabetes mellitus. Data were pooled from 13 placebo-controlled studies. Patients received dapagliflozin 10 mg/day (n = 2360) or placebo (n = 2295) for up to 24 weeks. Dapagliflozin was associated with placebo-subtracted changes from baseline in systolic and diastolic blood pressures of −3.6 and −1.2 mm Hg, respectively, in hypertensive patients and −2.6 and −1.2 mm Hg, respectively, in non-hypertensive patients. At 24 weeks, a similar proportion of patients experienced measured orthostatic reactions with dapagliflozin versus placebo in hypertensive (6.1% and 6.6%, respectively) and non-hypertensive (4.0% and 4.2%) patients. No clinically relevant difference was observed between dapagliflozin and placebo in heart rate. In conclusion, dapagliflozin 10 mg induces a modest reduction in blood pressure compared with placebo in patients with diabetes with a low risk of orthostatic reactions, regardless of baseline blood pressure.
Keywords
Introduction
Patients with diabetes are more than twice as likely as those without diabetes to develop hypertension. 1 As with non-diabetic patients, hypertension predisposes patients with diabetes to an increased risk of cardiovascular disease. However, this risk increases significantly in patients with both diabetes and elevated blood pressure (BP) compared with normotensive patients.1–3
Hypertension is a multifactorial disease, and the causes leading to an increase in incidence in the diabetic population are complex. It is estimated that close to 90% of the patients with type 2 diabetes mellitus (T2DM) are overweight or obese. 4 Because weight gain is associated with an accompanying increase in BP, 5 this may, in part, contribute to the higher incidence of hypertension in this population. Angiotensin II, a vasoconstrictor with salt-retaining activity, is a component of the renin-angiotensin-aldosterone system (RAAS). Activation of RAAS, resulting in an increase in insulin resistance, has also been implicated as a potential causal factor in the development of hypertension in T2DM.6,7 In addition, it has been proposed that during periods of hyperglycaemia, insulin itself may have a sodium-retentive effect that may be sufficient to promote or exacerbate hypertension. 8
Reducing BP in patients with diabetes is associated with a reduced risk of macrovascular disease.9,10 The European Society of Hypertension and the European Society of Cardiology recommend initiating treatment in patients with a systolic blood pressure (SBP) of ⩾140 mm Hg or a diastolic blood pressure (DBP) of ⩾90 mm Hg. 11 In addition, the American Diabetes Association and European Society of Cardiology/European Association for the Study of Diabetes recommend achieving an SBP of <140 mm Hg in patients with diabetes, although a lower goal (<130 mm Hg) may be appropriate in younger patients or those with kidney disease.12,13 Despite those threshold-driven recommendations, guidelines recognise a continuous, independent relationship of seated BP, ranging from high to relatively low (110–115/70–75 mm Hg), with the risk of cardiovascular events. 11 Meta-analysis data indicate similar risk reductions associated with BP lowering regardless of pre-treatment BP or cardiovascular risk. 14
Dapagliflozin is a highly selective inhibitor of sodium-glucose co-transporter 2 (SGLT2) that improves glycaemic control and reduces body weight in an insulin-independent manner in patients with T2DM through a reduction in renal glucose reabsorption and accompanying urinary glucose excretion. 15 Dapagliflozin also reduces BP in patients with T2DM.16–19 The BP-lowering effect may partly be explained by osmotic diuresis and possibly an altered sodium balance. 20 There is also a strong indication that the BP effect is also influenced by weight loss, 21 or rather a negative energy balance, as the full effect is visible before maximal weight loss has been attained.22,23
The aim of this pooled analysis was to evaluate whether baseline BP would have any impact on the subsequent BP-lowering effect of dapagliflozin in patients with T2DM.
Methods
Data were pooled from 13 phase 2b/3 dapagliflozin placebo-controlled clinical studies (Figure 1). Each study was designed and performed in accordance with the ethical principles that have their origin in the Declaration of Helsinki and are consistent with the International Conference on Harmonisation/Good Clinical Practice, the applicable regulatory requirements and the AstraZeneca policy on bioethics. All patients provided informed consent.
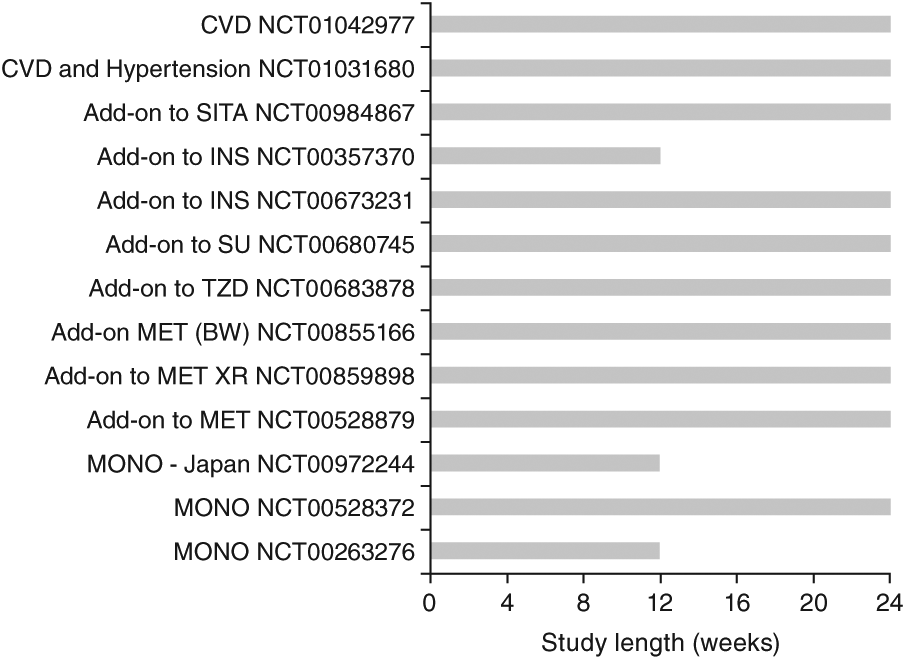
Studies included in the analyses.
Patients with T2DM were randomised to receive dapagliflozin 10 mg/day (n = 2360) or placebo (n = 2295) as monotherapy or in combination with other anti-hyperglycaemic medications for up to 24 weeks. The primary objective of this analysis was to evaluate the effect of dapagliflozin 10 mg/day on BP in patients with T2DM and baseline SBP > 140 mm Hg (hypertensive) or baseline SBP ⩽ 140 mm Hg (non-hypertensive). BP levels were used to define hypertension in this analysis regardless of the use of anti-hypertensive agents, and as such, there were patients in both groups with a medical diagnosis of hypertension. Baseline BP was determined by a single time point measurement performed in triplicate with the patient in a seated position. Heart rate and measured orthostatic reactions (defined as a decrease of >20 mm Hg in SBP or >10 mm Hg in DBP when transferring from a supine to standing position) were also measured. Additionally, any observed adverse events of orthostatic hypotension, as defined by the Medical Dictionary for Regulatory Activities, were recorded over the treatment period. The data were analysed using a linear model with factors for treatment, study and baseline SBP category, with the baseline measurement as a covariate. In addition to the above-mentioned analyses in hypertensive and non-hypertensive patients, a sub-analysis of the non-hypertensive group only consisting of those patients with a pre-treatment SBP ⩽ 120 mm Hg was performed in order to further characterise the safety profile of dapagliflozin in patients with very low BP.
Results
Patients
Overall, 2294 patients receiving dapagliflozin and 2222 receiving placebo who had baseline BP measurements and at least one post-baseline BP measurement were included in these analyses. Patient demographics and baseline characteristics were generally balanced between dapagliflozin and placebo groups (Table 1). Hypertensive patients tended to be older, weigh more, have a longer duration of T2DM and to have a higher prevalence of pre-existing cardiovascular disease and/or hypertension than their normotensive counterparts. In addition, more patients with SBP > 140 mm Hg at baseline were being treated with BP-lowering medications in the dapagliflozin and placebo groups (91.5% and 91.1%, respectively), either because of a diagnosis of hypertension or other indications, compared with patients with baseline SBP ⩽ 140 mm Hg (68.2% and 72.6%, respectively, Table 2). The use of specific anti-hypertensive treatments at baseline was balanced between dapagliflozin- and placebo-treated patients; angiotensin-converting enzyme inhibitors and angiotensin receptor blockers were most commonly used. The proportion of patients on anti-hypertensive drugs remained stable over the 24-week treatment period in both groups (change ⩽1%).
Demographics and baseline characteristics.
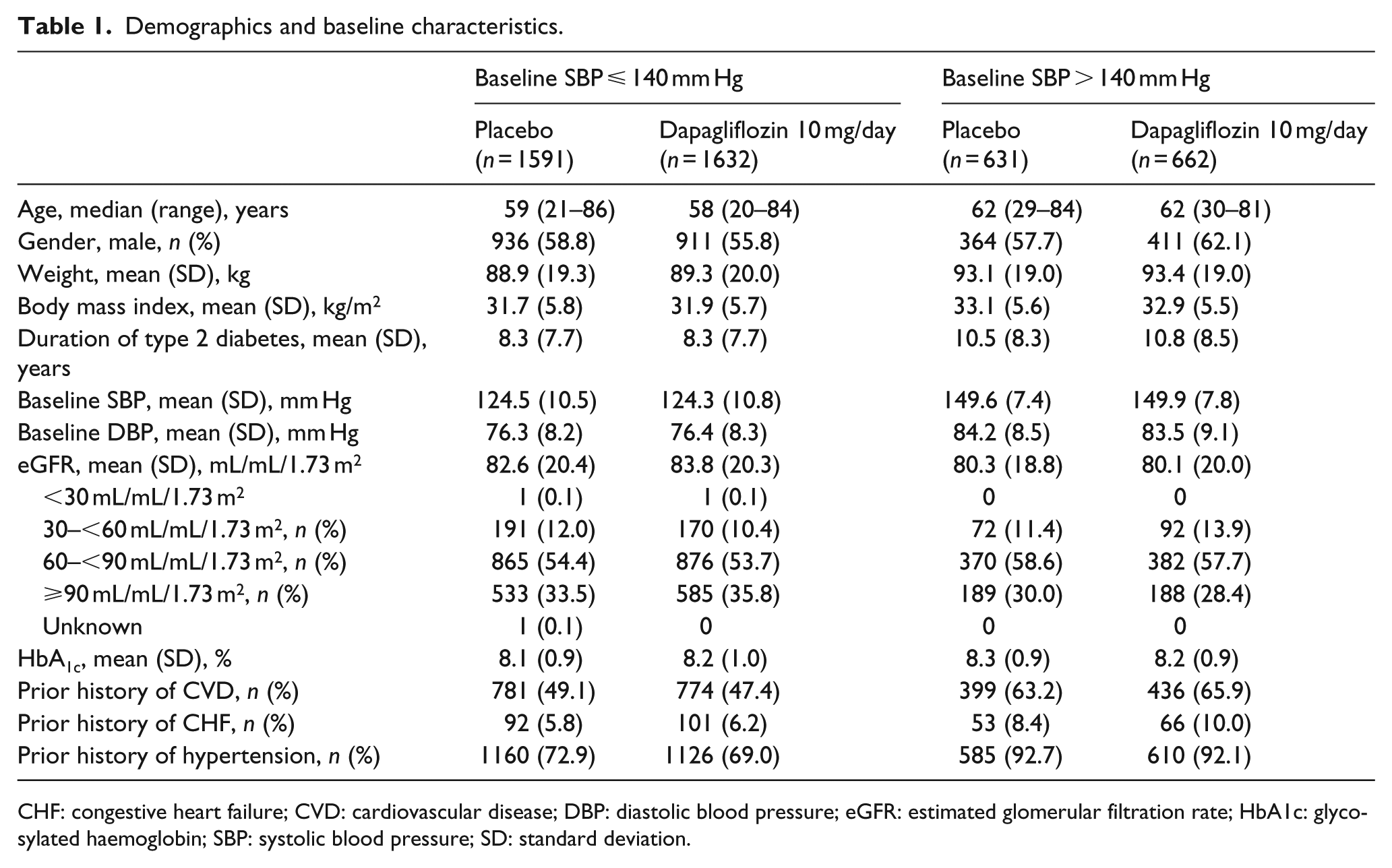
CHF: congestive heart failure; CVD: cardiovascular disease; DBP: diastolic blood pressure; eGFR: estimated glomerular filtration rate; HbA1c: glycosylated haemoglobin; SBP: systolic blood pressure; SD: standard deviation.
Anti-hypertensive medication use at baseline and week 24 in hypertensive versus non-hypertensive patients with type 2 diabetes mellitus.
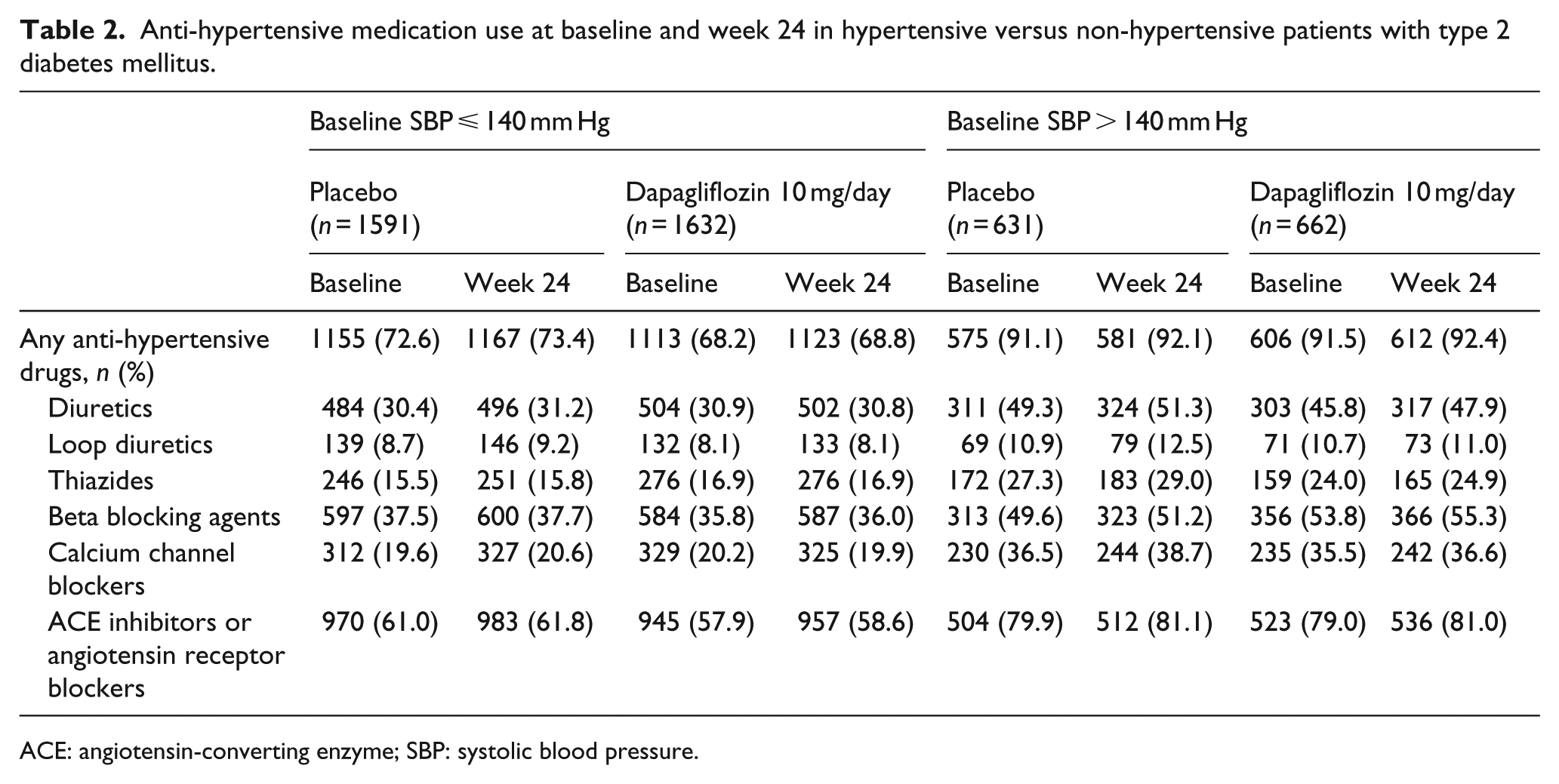
ACE: angiotensin-converting enzyme; SBP: systolic blood pressure.
BP
Following initiation of treatment, SBP dropped in hypertensive patients in both dapagliflozin and placebo treatment groups over the first week and levelled off thereafter through week 24 (Figure 2(a)). SBP in hypertensive patients treated with dapagliflozin dropped to a greater extent and remained below that of the placebo group throughout the entire study period: adjusted mean placebo-subtracted change [95% confidence interval (CI)] in SBP from baseline to week 24 was −3.6 mm Hg (−4.9 to −2.4 mm Hg). In non-hypertensive patients, SBP remained relatively constant over time with dapagliflozin, while SBP increased with placebo over the same time period (Figure 2(b)). The adjusted mean placebo-subtracted change (95% CI) in SBP from baseline to week 24 with dapagliflozin was −2.6 mm Hg (−3.4 to −1.8 mm Hg) in non-hypertensive patients.
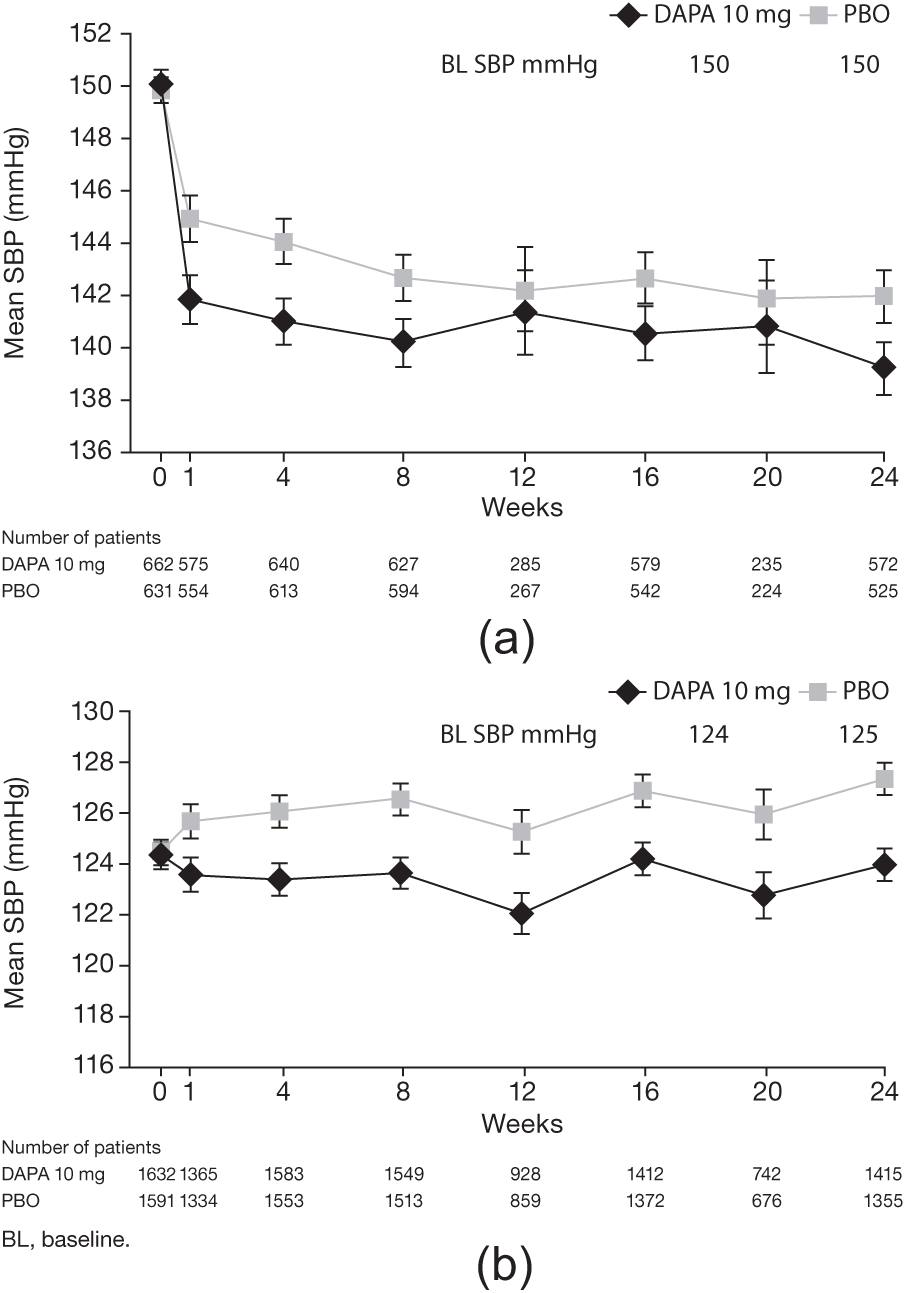
Change in systolic blood pressure (SBP) over time in patients with baseline SBP (a) >140 mm Hg or (b) ⩽140 mm Hg.
A similar pattern in DBP was observed over time. In hypertensive patients, DBP dropped in both treatment groups over the first week, remaining comparatively constant thereafter until week 24 (Figure 3(a)). Patients treated with dapagliflozin showed a greater decrease from baseline in DBP; the placebo-corrected change in DBP from baseline to week 24 was −1.2 mm Hg (−2.0 to −0.4 mm Hg). In non-hypertensive patients, little change from baseline in DBP was observed over time in the dapagliflozin group, compared with a slight increase in the placebo group [placebo-corrected change from baseline to week 24, −1.2 mm Hg (−1.8 to −0.7 mm Hg)] (Figure 3(b)).
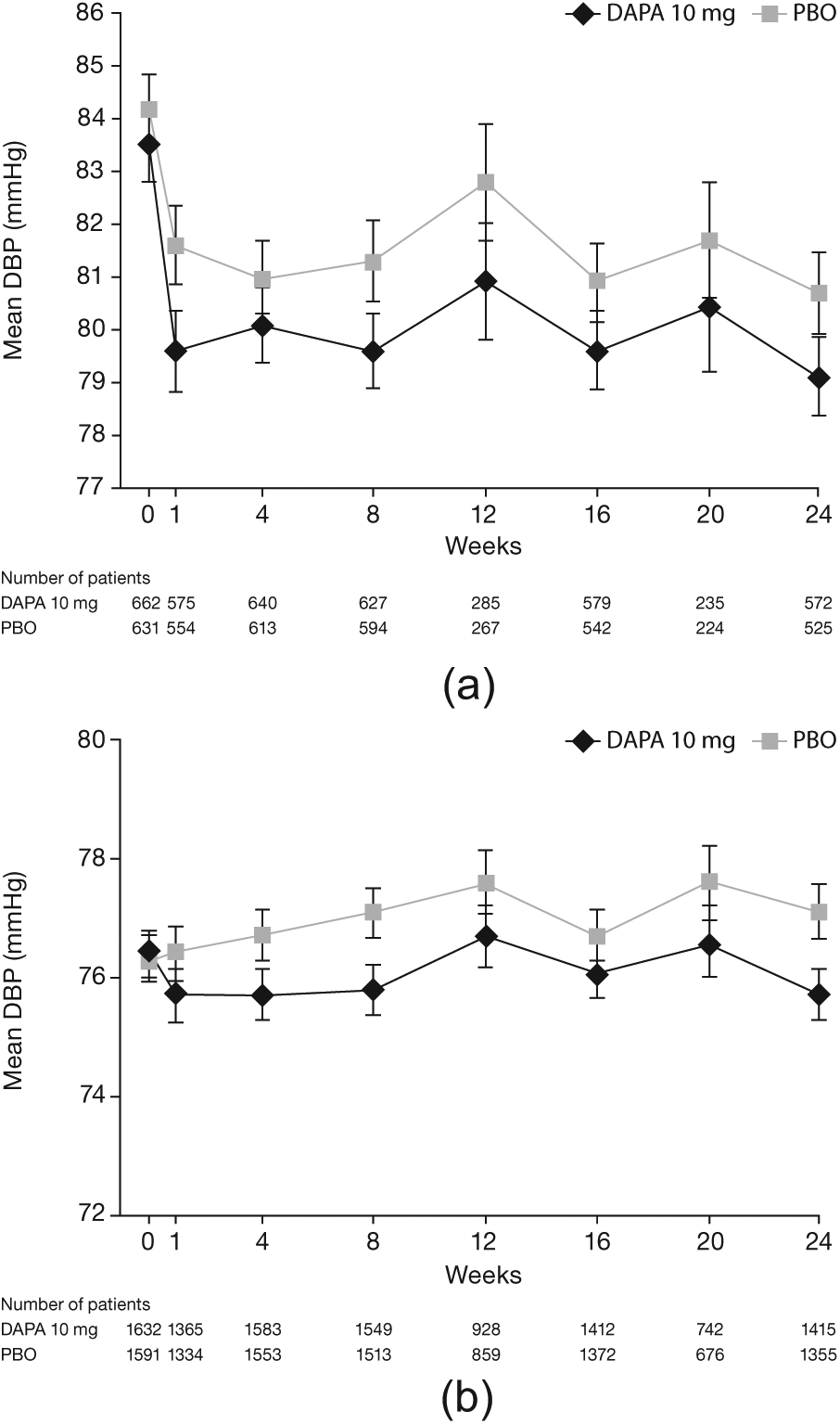
Change in diastolic blood pressure (DBP) over time in patients with baseline systolic blood pressure (SBP) (a) >140 mm Hg or (b) ⩽140 mm Hg.
Heart rate
No clinically relevant change from baseline in heart rate was observed in either dapagliflozin- or placebo-treated patients (Figure 4). In hypertensive patients, the mean change from baseline to week 24 was −0.5 and 0.4 beats/min, respectively, in dapagliflozin- and placebo-treated patients and was 0.1 and 0.7 beats/min, respectively, in non-hypertensive patients.
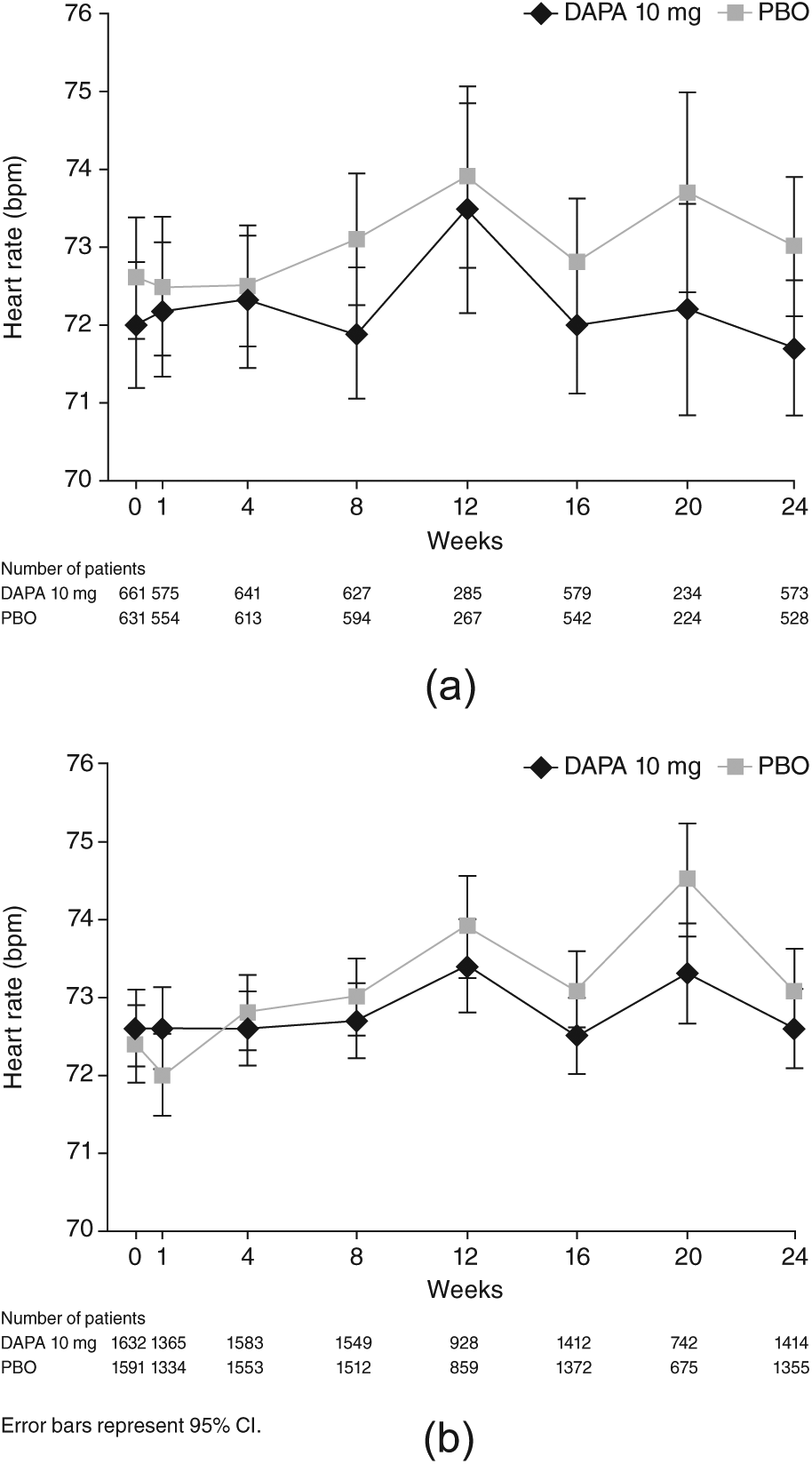
Change in heart rate in patients with baseline systolic blood pressure (SBP) (a) >140 mm Hg or (b) ⩽140 mm Hg.
Orthostatic hypotension
The proportion of dapagliflozin-treated patients with any measured postural orthostatic reaction over the 24-week treatment period was similar to placebo in hypertensive patients (dapagliflozin, 17.4%; placebo, 15.5%). Similarly, although the frequency of orthostatic reactions over the 24-week period was lower in non-hypertensive patients, the proportion of patients with postural orthostatic hypertension was also similar between the treatment groups (dapagliflozin, 11.4%; placebo, 9.6%). At the 24-week visit, the difference was small between dapagliflozin and placebo in the proportion of patients with measured orthostatic reactions in either hypertensive (6.1% vs 6.6%) or non-hypertensive (4.0% vs 4.2%) patients, respectively (Figure 5). Adverse events falling under the MedDRA preferred term ‘orthostatic hypotension’ were rare, and none were classified as serious. The highest rate was observed in the non-hypertensive placebo group (0.4%), and lower rates were observed in the non-hypertensive dapagliflozin group (0.1%) and both of the hypertensive groups (dapagliflozin, 0.2%; placebo 0%).
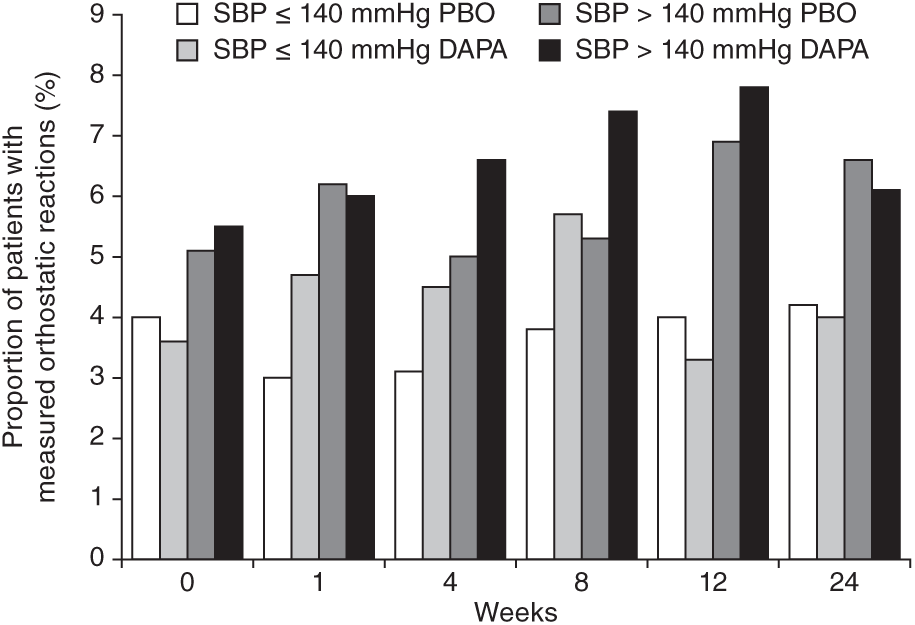
Measured orthostatic reactions.
Patients with SBP ⩽ 120 mm Hg
An additional subgroup analysis of the non-hypertensive patients described above was performed in 1081 patients with SBP ⩽ 120 mm Hg. In the dapagliflozin group, 566 patients had a baseline SBP ⩽ 120 mm Hg, and the corresponding number for placebo was 515 patients. The mean [standard deviation (SD)] SBP was 112.0 mm Hg (6.5 mm Hg) and 112.2 mm Hg (6.9 mm Hg) for dapagliflozin and placebo, respectively. SBP values ranged from 81.7 to 120 mm Hg. The corresponding values for DBP were 71.9 mm Hg (7.1 mm Hg) and 71.7 mm Hg (7.7 mm Hg), respectively. The adjusted mean placebo-subtracted change (95% CI) in SBP from baseline to week 24 with dapagliflozin was −2.5 mm Hg (−3.9 to −1.1 mm Hg) and for DBP was −1.7 mm Hg (−2.6 to −0.9 mm Hg). Heart rate increased on average 0.7 beats/min in the dapagliflozin group and 1.4 beats/min in the placebo group.
The proportion of dapagliflozin-treated patients with any measured postural orthostatic reaction over the 24-week treatment period was similar to placebo (dapagliflozin, 9.9%; placebo, 8.7%). The corresponding proportion of patients with a measured postural orthostatic reaction at the 24-week visit was 3.8% and 2.6%, respectively. There were no registered adverse events of orthostatic hypertension among the dapagliflozin-treated patients with a baseline SBP ⩽ 120 mm Hg.
Discussion
These analyses were performed to evaluate whether baseline BP prior to initiating dapagliflozin would have any impact on the subsequent BP-lowering effect of dapagliflozin in patients with T2DM. A safety analysis was also performed to evaluate possible differential effects on heart rate and orthostatic reactions in hypertensive and non-hypertensive patients. To our knowledge, this is the first analysis evaluating the impact of pre-treatment BP on the BP-lowering effect observed with an SGLT2 inhibitor in patients with T2DM.
Oral dapagliflozin 10 mg/day, administered as monotherapy or add-on to existing anti-hyperglycaemic agents, induced a modest reduction in BP versus placebo over the first week of treatment that persisted thereafter, regardless of baseline BP category. The apparently larger absolute reductions from baseline observed in hypertensive versus non-hypertensive patients, independent of treatment assignment, are most likely an effect of regression to the mean. This would be expected after an arbitrary dichotomisation of a study cohort with patients above the cut-off level showing reduced repeat values and those below showing a tendency toward increased values over time. We do not believe that this would compromise the main findings, as both placebo- and dapagliflozin-treated patients would be affected equally. Taking this into account, the most appropriate comparison under such circumstances was to use the placebo-corrected values to compare effects in hypertensive and non-hypertensive patients.
A slightly higher proportion of patients (~2%) receiving dapagliflozin compared with placebo experienced any measured orthostatic reaction over the entire 24-week observation period. This difference from placebo seemed independent of baseline BP category. Overall, hypertensive patients displayed a higher frequency of orthostatic reactions as compared with those with lower baseline BP, independent of the treatment assignment. This may be due to the more frequent use of anti-hypertensive medications by hypertensive patients as well as more adverse cardiovascular status such as arterial stiffness and compromised compensatory mechanisms. Also, the definition of measured orthostatic reactions might lead to more patients with high SBP fulfilling the criteria for an event. It was, therefore, reassuring that the number of clinically registered adverse events of orthostatic hypotension was not increased in the dapagliflozin group as compared with placebo. No clinically relevant change from baseline in heart rate was observed in either dapagliflozin- or placebo-treated patients.
The main findings of this investigation were corroborated in a sensitivity analysis comprising only those patients with SBP ⩽ 120 mm Hg. In this cohort, dapagliflozin induced a modest reduction in BP similar in magnitude to the cohorts with higher baseline BP, without a substantial increase in orthostatic reactions as compared with placebo.
A limitation when interpreting these results is that the change in BP was not defined as the primary study objective in most of the studies pooled for this analysis. As such, the control, or monitoring of BP medication changes, was suboptimal, making it not possible to control for possible changes in dosage, even though the number of patients on anti-hypertensive medications across the trials was known. However, given the stable number of patients using different types of anti-hypertensives over the 24-week period, it is unlikely that the observed placebo-corrected reductions in BP levels are explained by dose adjustments.
These results accumulated from placebo-controlled studies across the dapagliflozin clinical programme indicate a lowering of SBP regardless of baseline BP category not accompanied by orthostatic hypotension. These data may provide guidance for physicians when prescribing dapagliflozin, particularly in patients on concomitant anti-hypertensive medications who could benefit from additional glycaemic, weight and BP control. The long-term clinical benefits of dapagliflozin treatment were not studied here but are currently under investigation in a large-scale outcome study (DECLARE, NCT01730534 – clinicaltrials.gov).
Footnotes
Declaration of conflicting interests
C. David Sjöström, Peter Johansson and Eva Johnsson are employees and shareholders of AstraZeneca. Agata Ptaszynska is an employee and shareholder of Bristol-Myers Squibb. James List was an employee and shareholder of Bristol-Myers Squibb at the time the analysis was conducted.
Funding
This analysis was funded by AstraZeneca. Editorial support was provided by Karen Pemberton, PhD, of PPSI (a PAREXEL company) and was funded by AstraZeneca.