
Abstract
Background:
Limited data are available about the characteristics, treatment and survival in patients without diabetes mellitus (DM), previously diagnosed DM and patients with hyperglycaemia who present with acute decompensated heart failure (ADHF). Our objectives were to examine differences in these endpoints in patients hospitalized with ADHF.
Methods:
Patients hospitalized with ADHF during 1995, 2000, 2002 and 2004 comprised the study population.
Results:
A total of 5428 non-diabetic patients were hospitalized with ADHF, 3807 with diagnosed DM and 513 with admission hyperglycaemia. Patients with admission hyperglycaemia experienced the highest in-hospital death rates (9.9%) compared to those with diagnosed DM (6.5%) and non-diabetics (7.5%). Patients with diagnosed DM had the greatest risk of dying after hospital discharge.
Conclusions:
Patients with elevated blood glucose levels at hospital admission are more likely to die acutely. After resolution of the acute illness, patients with previously diagnosed DM need careful monitoring and enhanced treatment.
Introduction
Heart failure is an increasingly common chronic medical condition that is associated with significant morbidity, mortality and health-care burden. 1 Given the advanced age of patients with heart failure, patients hospitalized for this clinical syndrome typically have a substantial number of additional comorbidities present, one of the most prevalent of which is diabetes mellitus (DM).1–3 DM has also been linked to the development of increased vascular stiffness and impaired diastolic function.4,5
The prevalence of DM in American men and women has been rising steadily over time, with approximately 1 in 14 adults affected by this metabolic disorder.6–8 Recent estimates project a continuing increase in the prevalence of diagnosed DM over the next several decades.9,10 A limited number of studies have shown that upwards of 40% of patients with heart failure have co-occurring DM, nearly four times greater than the prevalence of DM in the general population.11,12 Among patients with heart failure, DM is associated with increased mortality.13,14 Reduced survival among patients with heart failure and DM is, in part, attributable to the presence of hyperglycaemia, which has been associated with an increased risk of cardiovascular events, heart failure-related hospitalizations and total mortality.10,13–15 Despite an increased risk of dying among heart failure patients with DM,16,17 the health-care practices in those with and without DM may be similar.3,10–12 Furthermore, long-term mortality has been shown to be similar among both diagnosed and undiagnosed diabetics with hyperglycaemia.14,15 Limited data also exist to suggest that elevated serum glucose level at the time of hospital presentation, in the absence of a history of DM, may be an important prognostic factor in patients with an acute exacerbation of heart failure.
The objectives of this observational study were to describe the epidemiology of DM and hyperglycaemia in a large population-based cohort of patients hospitalized with acute decompensated heart failure (ADHF) at all 11 medical centres in central Massachusetts. Our primary study aims were to examine differences in patient characteristics, hospital treatment practices, in-hospital survival and post-discharge mortality in non-diabetics, previously diagnosed diabetics, and in patients with elevated blood glucose levels at the time of hospital admission for ADHF using data from the Worcester Heart Failure Study (WHFS).18–20
Methods
The WHFS is a population-based surveillance study of adult male and female residents of the Worcester, MA, metropolitan area (2000 census estimate = 478,000) admitted to all 11 central MA medical centres for possible ADHF during the years 1995, 2000, 2002 and 2004.18–20 These study years were selected due to the availability of federal funding support and to correspond with population census estimates.
The medical records of residents of central Massachusetts admitted to all greater Worcester medical centres during the years under study were reviewed in a standardized manner for primary and/or secondary International Classification of Diseases–9 (ICD-9) discharge diagnoses consistent with possible ADHF.18–20 Patients with a discharge diagnosis of ADHF (ICD-9 code 428) comprised the primary diagnostic category reviewed for the identification of possible cases of ADHF. In addition, trained study physicians and nurses reviewed the medical records of patients with discharge diagnoses of rheumatic heart failure, hypertensive heart and renal failure, acute cor pulmonale, cardiomyopathy, pulmonary heart disease and congestion, acute lung oedema, oedema, dyspnoea and respiratory abnormalities for purposes of identifying patients who may have experienced new-onset heart failure. The diagnosis of heart failure was confirmed using the Framingham criteria. 21
Data collection
Information about patient demographics, medical history, clinical characteristics and laboratory test results was collected through the review of information contained in hospital medical records. This information included patient’s age, sex, race, prior comorbidities (e.g. history of DM, hypertension), laboratory findings (e.g. admission serum glucose and creatinine findings), clinical characteristics (e.g. presenting heart rate, blood pressure) and hospital survival status. Due to our methods of data collection, we did not collect information about the specific cause of death in patients who died either in the hospital or after hospital discharge.
Information about the diagnosis of DM was obtained from hospital medical records. Three diabetes groupings were created: non-diabetics (absence of a history of DM and a random admission serum glucose <200 mg/dL measured at the time of hospitalization for ADHF); diagnosed diabetics (prior history of DM or receipt of diabetic medications on admission as documented in hospital medical records) and admission hyperglycaemic patients (absence of a history of DM but serum glucose findings at the time of hospital admission for ADHF⩾ 200 mg/dL based on current American Diabetes Association guidelines). 22 In addition, because some patients with DM might have been misclassified as being non-diabetic based on the extent of information contained in hospital medical records, a sensitivity analysis was performed to examine the impact of a different working definition of DM on our principal study findings. For this analysis, patients without a history of DM were re-classified as being diabetic if their serum glucose level was ⩾ 140 mg/dL at the time of hospital admission for ADHF. This additional cut point was chosen because the American Diabetes Association considers patients to be prediabetic with an oral glucose tolerance test ⩾ 140 mg/dL.
Physician’s progress notes and daily medication logs were reviewed for information related to the prescribing of selected cardiac medications. The cardiac medications examined included those shown to be of benefit in improving the prognosis of patients with ADHF [angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs) and beta-blockers], those shown to be effective at improving the symptomatic status of patients with acute heart failure, 23 as well as other effective cardiac medications (e.g. aspirin, lipid lowering agents). Survival status after hospital discharge through the end of 2011 was ascertained through a review of subsequent hospital medical records and a statewide and national search of death certificates for residents of the Worcester metropolitan area.
Data analysis
We examined differences between our three primary comparison groups with regard to their demographic characteristics, medical history, presenting symptoms, clinical admission data and receipt of hospital therapies using chi-square tests and analysis of variance (ANOVA) for discrete and continuous variables, respectively.
Differences in hospital case-fatality rates (CFRs) according to DM status were examined using unadjusted and multivariate logistic regression modelling. Differences in 3-month, 1-year and 2-year post-discharge survival estimates were examined using Cox proportional hazards models, which adjusted for patient’s age, sex, presenting symptoms, medical history and clinical admission data in addition to duration of long-term follow-up.
Results
Patient characteristics
The study sample consisted of 9748 residents of the Worcester metropolitan area hospitalized at all 11 medical centres in central Massachusetts with independently confirmed ADHF in whom information about a history of DM and admission serum glucose levels was available. Our study population comprised 5428 (56%) non-diabetics, 3807 (39%) diagnosed diabetics and 513 (5%) patients with hyperglycaemia at the time of hospital admission for ADHF. The average age of the study sample was 76 years, 56% were women, and 29% were diagnosed with an initial episode of ADHF.
Patients with diagnosed DM tended to be younger than the other comparison groups, whereas patients with admission hyperglycaemia included a greater proportion of women. There were a greater proportion of patients with diagnosed DM who had additional comorbid conditions previously diagnosed. Diabetic patients were more likely to present with symptoms of angina/chest pain, oedema/recent weight gain, nausea/vomiting and orthopnoea; admission hyperglycaemic patients were more likely to have presented with dyspnoea and non-diabetics with weakness (Table 1). Among the three groups of patients, diabetics had the highest body mass index (BMI) and lowest estimated glomerular filtration rate (eGFR), and admission hyperglycaemic patients had the highest systolic and diastolic blood pressures, heart rate, and presented with higher mean serum glucose levels (260 mg/dL) at the time of hospital admission for ADHF as compared with the two other groups.
Characteristics of patients with acute decompensated heart failure.
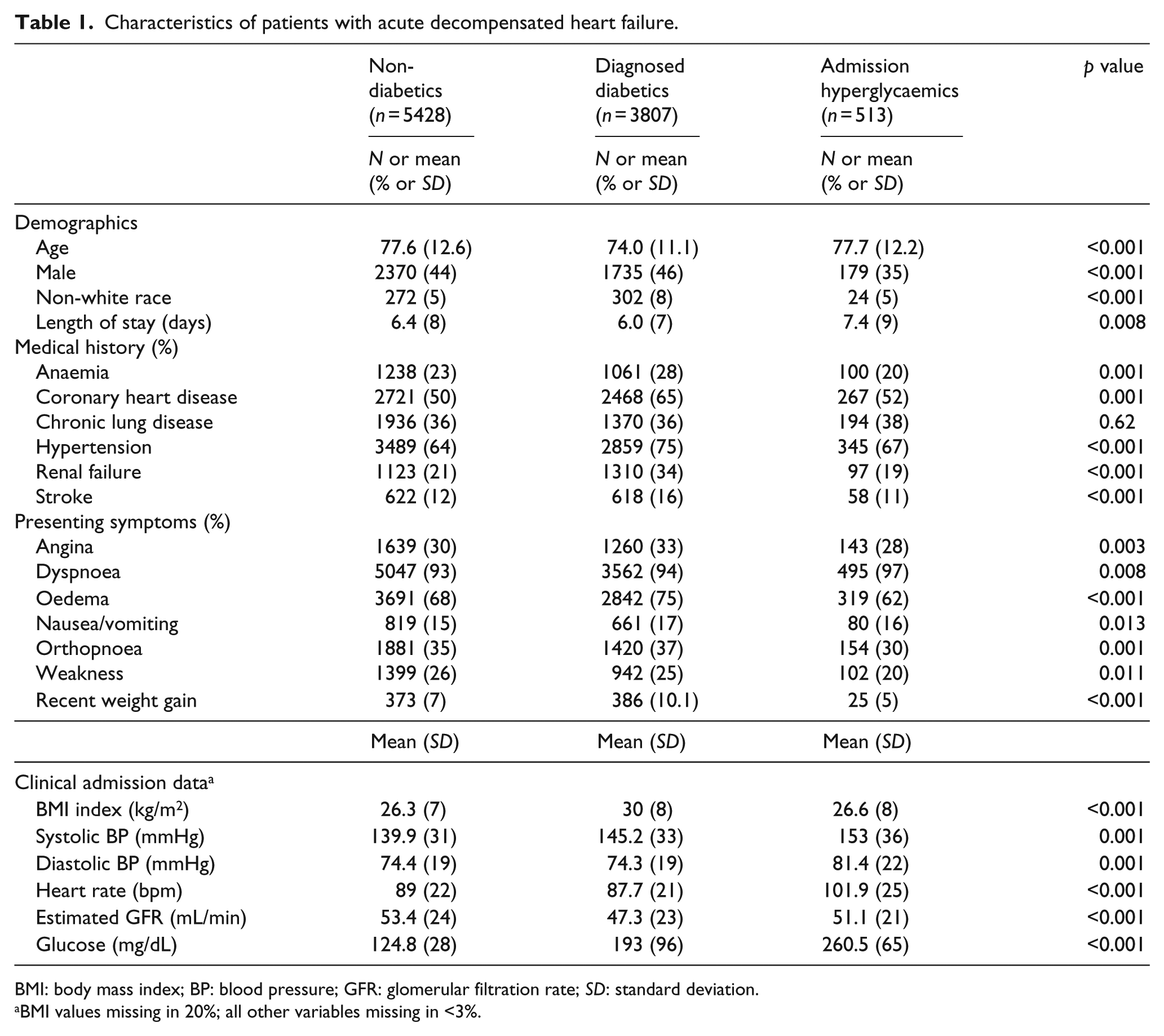
BMI: body mass index; BP: blood pressure; GFR: glomerular filtration rate; SD: standard deviation.
BMI values missing in 20%; all other variables missing in <3%.
Hospital treatment practices
In examining between-group differences with regard to hospital treatment practices, diagnosed diabetics were the most likely to have been treated with effective cardiac medications including ACE inhibitors/ARBs, aspirin, beta-blockers and lipid lowering agents. Admission hyperglycaemic patients were the most likely to have undergone coronary angioplasty (8% vs 5%–6%) and coronary artery bypass graft surgery (1.8% vs 0.6%) during their index hospitalization, but the rates across all three study groups were low (Table 2).
Hospital treatment practices in patients with acute decompensated heart failure.
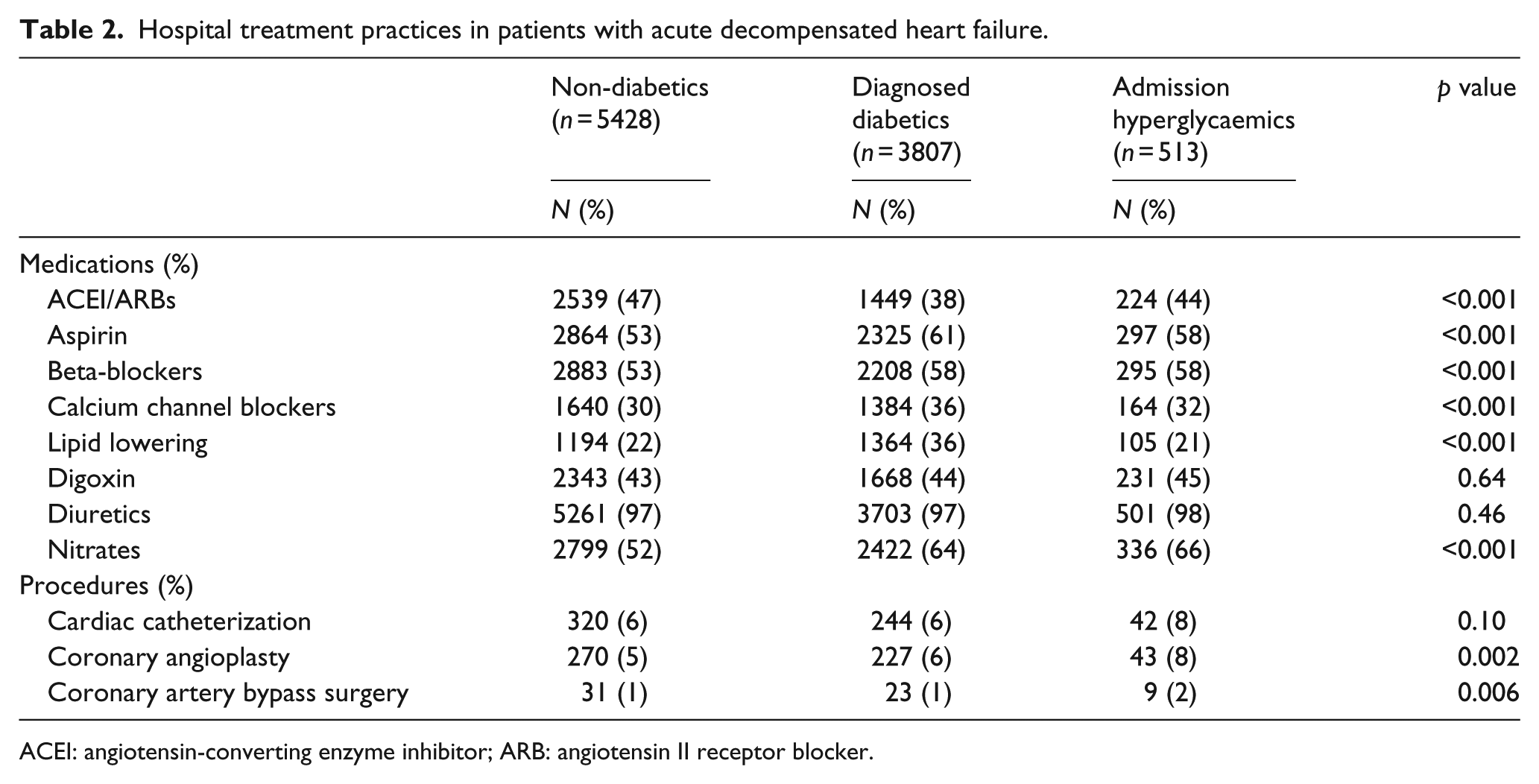
ACEI: angiotensin-converting enzyme inhibitor; ARB: angiotensin II receptor blocker.
Hospital death rates
Patients with admission hyperglycaemia experienced the highest hospital CFRs at nearly 10%, non-diabetics had lower hospital CFRs (7.5%) and diagnosed diabetics (6.5%) had the lowest in-hospital CFRs. In our fully adjusted regression model, controlling for several demographic and clinical factors of prognostic importance, admission hyperglycaemic patients were at a 49% higher risk of dying in the hospital compared with non-diabetics (Table 3).
Odds of dying during hospitalization for acute decompensated heart failure.
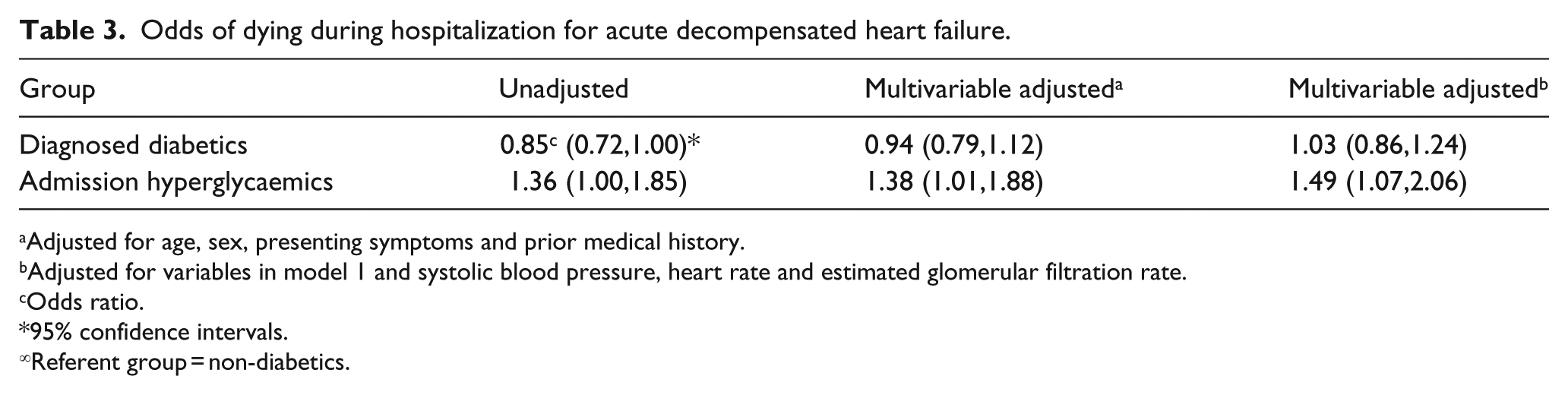
Adjusted for age, sex, presenting symptoms and prior medical history.
Adjusted for variables in model 1 and systolic blood pressure, heart rate and estimated glomerular filtration rate.
Odds ratio.
95% confidence intervals.
Referent group = non-diabetics.
In a sensitivity analysis using an admission serum glucose cut-off of ⩾ 140 mg/dL, admission hyperglycaemic patients experienced the highest short-term CFRs (8.6%), followed by diagnosed diabetics (7.7%) and non-diabetics (6.5%). In our fully adjusted regression model, patients with admission hyperglycaemia were at a 26% higher risk for dying in the hospital compared with non-diabetics.
Post-discharge mortality
Patients with previously diagnosed DM had a 14% higher risk for dying at 3-months post-discharge [hazard ratio (HR) = 1.14, 95% confidence interval (CI) = 1.09,1.20] and an 18% higher risk of dying from all causes at 1 and 2 years post-discharge (HR = 1.18, 95% CI = 1.11,1.24; HR = 1.18, 95% CI = 1.11,1.26). On the other hand, although not statistically significant, admission hyperglycaemic patients had an intermediate risk for dying from all causes at 3 months, 1 year, and 2 years post-discharge between that of the non-diabetics and previously diagnosed diabetics (Table 4). Similar findings were observed when we carried out a sensitivity analysis using a serum glucose cut-off of ⩾ 140 mg/dL.
Odds of dying after hospital.
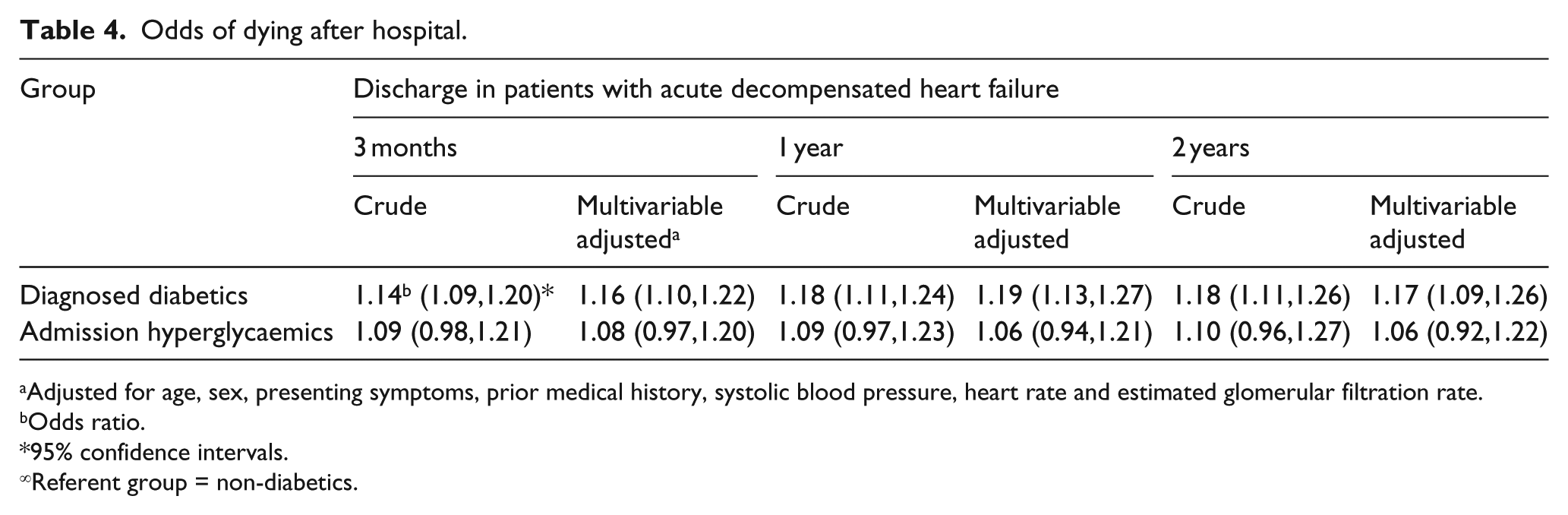
Adjusted for age, sex, presenting symptoms, prior medical history, systolic blood pressure, heart rate and estimated glomerular filtration rate.
Odds ratio.
95% confidence intervals.
Referent group = non-diabetics.
Discussion
The results of our study among residents of a large central New England metropolitan area hospitalized for ADHF suggest that admission hyperglycaemic patients are more likely to die during their acute hospitalization than non-diabetics and patients with previously diagnosed DM. We hypothesize that the higher short-term death rates experienced by patients with transiently elevated levels of blood glucose at the time of hospitalization for ADHF may serve as a marker for an acute stress response to severe illness. This hypothesis is supported by the high acute mortality rates as well as the higher utilization of cardiac procedures (coronary artery bypass surgery and coronary angioplasty) in these patients. After hospital discharge and resolution of the acute illness, the adverse impact of previously diagnosed DM on patient’s long-term survival emerges. 24 Patients with previously diagnosed DM experienced the highest post-discharge death rates at all time points examined compared with the other groups under study in this population-based investigation.
Risk of hyperglycaemia in diabetics and non-diabetics
Hyperglycaemia is associated with increased mortality, risk of re-hospitalization and other adverse outcomes, including dementia, 25 in patients with and without DM.26,27 In a study of 1886 critically ill patients who were hospitalized at a community teaching hospital in Atlanta, Georgia, 26% had a history of DM and 12% had hyperglycaemia. 27 Patients with hyperglycaemia, as measured by an admission or in-hospital fasting blood glucose level of ⩾ 126 mg/dL or a random blood glucose level of ⩾ 200 mg/dL on two or more determinations had a higher risk for intensive care unit (ICU) admission, longer hospital stay, higher risk of discharge to extended care and higher in-hospital death rates than persons with either DM or normal serum glucose levels. In a study of 1122 non-diabetics with ADHF, in-hospital mortality in patients with the highest admission blood glucose levels was twice as high compared to patients with lower blood glucose levels. 28 However, there were no between-group differences in mortality rates at the time of the 1-year follow-up.28,29 Among a large multinational cohort of more than 6000 patients with ADHF, elevated levels of blood glucose at the time for hospitalization for ADHF were associated with an increased risk of dying at 30 days, irrespective of a history of DM and other important covariates of prognostic importance. 30 Our study extends previous findings by comparing three distinct groups of admission hyperglycaemic patients, non-diabetics and patients with previously diagnosed DM who were derived from a large population-based study of patients with independently confirmed ADHF.
Hospital treatment practices
In our study, patients with previously diagnosed DM were more likely to have been treated with effective cardiac medications than admission hyperglycaemic patients or those without a history of DM. Our findings suggest that these patients may have been receiving closer monitoring and more aggressive treatment by their physicians. However, patients with elevated blood glucose levels at the time of hospital admission were most likely to have undergone an interventional cardiac procedure, supporting our hypothesis of an acute stress response to ADHF and potentially more severe cardiac disease.
Long-term prognosis
In patients with heart failure, the presence of comorbid DM is associated with an increased risk of long-term mortality.13,29 Among more than 600 patients with heart failure and DM in Olmsted County, Minnesota, the 5-year survival rate was 37% among patients with DM and 46% among patients without DM. 17 In addition, among a cohort of 528 individuals hospitalized for a first episode of heart failure in Leicestershire, UK, elevated admission plasma glucose levels (~180 mg/dL) were associated with increased all-cause mortality during follow-up, even among patients without a clinical diagnosis of DM. 31 It is clear that DM is associated with a greater risk of dying in general, and more so in the face of heart failure.
Non-diabetic patients who developed hyperglycaemia during an acute illness have been shown to be at increased risk for developing DM. In a study of 511 individuals admitted to an ICU in a single University Hospital in Croatia between 2000 and 2002, patients with modest levels of hyperglycaemia (>140 mg/dL) were at a more than fourfold increased risk of developing Type II DM over the ensuing 5 years in comparison to persons with normal serum glucose levels. 32 These findings suggest the need for careful long-term monitoring of patients with transiently elevated blood glucose levels in the setting of an acute illness, including ADHF.
Study strengths and limitations
Strengths of this study include its large sample size, the population-based design and its decade-long prospective follow-up. Identification of patients with elevated serum glucose levels in the setting of duress, such as ADHF, offers a novel finding, and sensitivity analyses showed that multiple definitions for hyperglycaemia yielded similar results. Our study has several limitations, however, that must be kept in mind in interpreting the study results. Due to our methods of data abstraction, we were only able to characterize patients with a history of diabetes if the medical record indicated DM as a diagnosis, or if the patient was being treated with insulin or diabetic medications at admission. Information about the use of diabetic medications and insulin during hospitalization was not recorded as part of our data collection procedures, so it is possible that some patients with hyperglycaemia were identified as incident cases of DM and treated as such during their hospitalization for ADHF. Laboratory information about serum glycated haemoglobin (HbA1c) levels was not available, nor were data collected on additional follow-up glucose measurements during hospital admission; inasmuch, it is unknown to what extent persistent hyperglycaemia played a role in patients’ in-hospital or long-term survival. We were unable to determine whether or not patients developed DM over the course of our extended follow-up. Finally, our study population consisted predominantly of older Caucasian patients and our findings may not be generalizable to other patient groups hospitalized with ADHF.
Conclusion
The results of this population-based study show that in patients hospitalized with ADHF, elevated serum glucose levels in non-diabetic patients at the time of hospital admission may deserve special attention. Admission hyperglycaemia serves to identify patients at high risk for hospital mortality, but this risk decreases with resolution of the acute illness. However, hyperglycaemic non-diabetic patients may be at increased risk of developing diabetes over the long term, justifying the careful monitoring of these individuals after hospital discharge.
Footnotes
Acknowledgements
We are indebted to the nurses and physicians who were involved in the abstraction of data from the medical records of patients hospitalized with acute decompensated heart failure. This work is dedicated to the memory of Joshua Bryan Inouye Helfand.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
Grant support for this project was provided by the National Heart, Lung, and Blood Institute (R01 HL69874).