
Abstract
Attendance at diabetic retinopathy screening in minority ethnic groups, including the South Asian population, is known to be poor. We describe a cluster randomised controlled trial conducted in 10 general practitioner (GP) surgeries in Coventry, UK, during 2007 which aimed to evaluate the use of a Link Worker–delivered intervention to improve attendance. The intervention consisted of a simple telephone reminder with the main outcome measure being attendance at diabetic retinopathy screening. We found a statistically significant difference between mean attendance proportions for intervention (0.89) and control (0.74) practices: difference (95% confidence interval (CI)) 0.15 (0.04–0.27), t = 3.03, p = 0.0162; this difference remained significant when adjusted for previous year’s proportions. In this proof-of-concept study, in inner city Coventry, we demonstrated increased attendance at diabetic retinopathy screening by use of a simple Link Worker–implemented telephone call intervention. The use of Link Worker phone calls may be a useful tool to increase attendance for diabetic retinopathy screening in a group with high did-not-attend (DNA) rates and a high prevalence of diabetic retinopathy and visual impairment.
Keywords
Introduction
Diabetic retinopathy is the leading cause of blindness among the working age group, the incidence of blindness is increasing and the prevalence of visual impairment is high in South Asians in the United Kingdom.1–4 UK resident South Asians with diabetes have a significantly higher prevalence of any retinopathy and maculopathy compared to indigenous White Europeans. 5 It is reported that uptake for health screening programmes, including diabetic retinopathy screening, is poor among minority groups. 6 In 2005, retinopathy screening uptake was 64.3% in Coventry and Warwickshire general practitioner (GP) practices with high proportions of patients of South Asian origin, compared to 72% in practices with predominantly patients of White European origin.
During the United Kingdom Asian Diabetes Study (UKADS) 7 carried out in the mainly South Asian Foleshill area of Coventry during 2004–2007, uptake of retinopathy screening in GP practices involved increased by up to 20% (personal communication – J Paul O’Hare (2008), local screening data). As part of the UKADS complex intervention, Link Workers encouraged patient attendance at practice diabetes clinics and promoted patient understanding of their condition and treatments. 7 We hypothesised that the improved retinopathy screening uptake might have been influenced by the Link Workers’ activities.
This proof-of-concept study aimed to test this hypothesis using a cluster randomised controlled trial (RCT); to our knowledge, this is a novel study aimed at increasing uptake of retinopathy screening in a hard-to-reach and high-risk population group.
Patients and methods
Study design and patients
The study was a cluster RCT; random allocation and the main comparative statistical analyses were performed at the cluster (GP practice) level. A total of 10 GP practices in Coventry with a high proportion of patients of South Asian ethnicity consented to be randomised for the study to either intervention or control. Following randomisation and throughout the study, there was no further contact with control practices.
In Coventry and Warwickshire, the standard diabetic retinopathy screening procedure is to invite all eligible patients to attend a screening appointment. Patients who fail to attend their initial screen date are sent a further appointment date by post. Screening is organised on a practice-by-practice basis.
Link Workers
Three multi-lingual Link Workers already employed by Coventry Primary Care Trust (PCT) were trained in diabetes management and care and assigned to work with specific intervention GP surgeries.
Intervention
The intervention was conducted from 1 January 2007 to 31 December 2007 and consisted of Link Worker telephone calls to individual patients to encourage attendance at diabetic retinopathy screening. Name and contact details of all patients from intervention practices failing to attend first screening appointment were sent to the study coordinator and passed to the relevant surgery-specific Link Worker. During the day prior to the second screening appointment, Link Workers contacted patients by telephone to remind them of the screening and to encourage attendance. The telephone intervention was conducted in a language appropriate to the patient. Time spent on the intervention was recorded by Link Workers and the study coordinator.
Data were collected on attendance at screening dates for control and intervention practice patients. Screening attendance proportions were calculated for all practices and differences between intervention and control practices plus 95% confidence intervals (95% CI) estimated. Date collected for the previous year (2006) were also extracted and compared.
Sample size and power
Based on 2005 uptake rates, to achieve a 6% increase in intervention practices, with 80% power and p = 0.05, 860 patients were required in each arm of the trial; 10 GP practices each with 200 patients.
Statistical analyses
Data available for analyses comprised routinely collected and collated attendance data from the retinopathy screening unit; there were no individual patient level data. We estimated and compared proportions, differences between proportions and 95% CI for screening attendances in 2006 and 2007 for intervention and control practices. Mean 2007 attendance proportions for intervention versus control practices were compared using a t-test, plus a linear mixed effects model to adjust for 2006 attendance proportion.
Results
In the study year (2007), the total number of patients invited to attend for retinopathy screening was 2680, 988 from intervention and 1692 from control practices. In total, 860 (87%) intervention and 1232 (73%) control group patients were attended. Numbers of patients invited and attending screening appointments by practice for study year and preceding year (2006) were highly correlated, r = 0.787, p = 0.0069. In all practices, numbers of patients invited for screening had increased, and in all but one practice, proportions attending also increased. In the study year, there was a statistically significant difference between mean attendance proportions for intervention (0.89) versus control (0.74) practices: difference (95% CI) 0.15 (0.04–0.27), t = 3.03, p = 0.0162. In a linear regression model, this difference remained significant once adjusted for 2006 proportions; difference of least-squares means 0.12 (0.07–0.17), t = 5.75, p = 0.0007.
During the study, 717 (73%) intervention and 1112 (66%) control practice patients attended their first screening appointment. Table 1 shows proportions between intervention and control groups at first and second appointments. Of the patients contacted by Link Workers, 70% attended their second appointment compared to 28% of those not contacted.
Comparison of screening proportions between intervention and control groups.
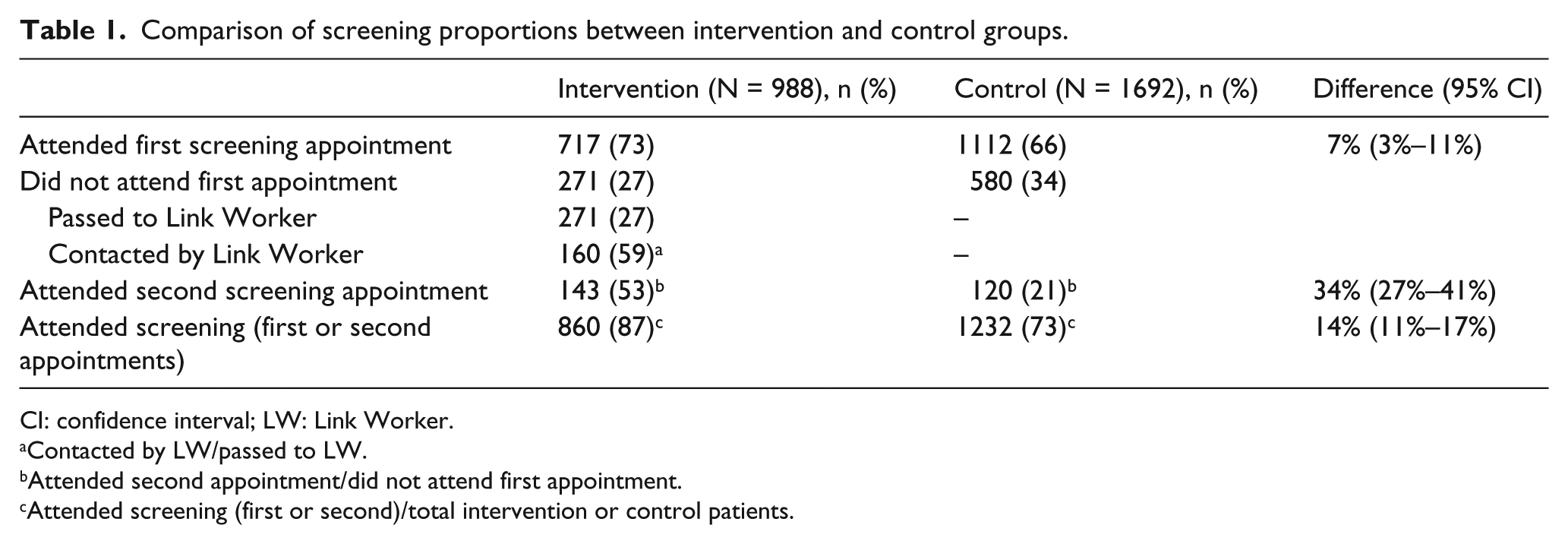
CI: confidence interval; LW: Link Worker.
Contacted by LW/passed to LW.
Attended second appointment/did not attend first appointment.
Attended screening (first or second)/total intervention or control patients.
Of the 111 intervention group patients the Link Workers were unable to contact, there was ‘no reason’ given for 36 (32%) cases, with administration problems accounting for 42 (38%).
Over the year, the total time spent delivering the intervention, including Link Worker and administrative work, was 960 min (16 h), representing approximately 3 h per GP surgery.
Discussion
In this proof-of-concept cluster RCT, we observed a significant effect, with more patients from the Link Worker intervention than those in control practices attending for diabetic retinopathy screening. This difference, around 15% (4%–27%), was statistically significant at the 5% level and remained so after adjustment for the previous year attendance proportion.
Many Clinical Commissioning Groups employ Link Workers; innovative use of this resource in enhancing retinopathy screening uptake could prove cost-effective. A major obstacle in this study was the high level of unrecorded and inaccurate telephone contact details making contacting patients difficult. Such administrative problems have a substantial effect and have been noted by other researchers.8–10 Greater attention to accuracy in this area could be important for retinopathy screening units trying to improve uptake.
Poor retinopathy screening uptake is strongly associated with social deprivation, 11 and the practices in this study were all inner city practices from a relatively deprived area of Coventry. Since social deprivation is associated with poorer health outcomes in general, those who are poor attendees are likely to be the group at the highest risk of diabetic retinopathy and as such are an important group to target. For screening programmes to be successful, innovative methods and efforts to involve these hard-to-reach groups need to be implemented.
Previous initiatives in this area have had mixed results and been time-consuming and expensive, unlike this intervention. One recent study in the United States used a similar intervention with results comparable with ours. 12
The major limitations of the study are related to the design and setting. Our observations are based on a population in one city involving only one screening centre, and our findings may be limited to this population. The results need to be confirmed with a large-scale multi-centre cluster RCT. This study recruited five interventions and five control practices, but there were far more control patients, indicating that randomisation of a small number of practices had led to an imbalance, with control practice sizes larger. In a larger multi-centre study, stratification by practice size could be undertaken to promote balance of number of intervention and control patients.
Further evaluation of the clinical and cost-effectiveness of this Link Worker function is required and there may be opportunity for extension of this concept to other minority ethnic populations in the United Kingdom, including South Asian populations in other regions and other minority ethnic groups where screening uptake is suboptimal. With an increasingly diversified and multi-ethnic population, simple cost-effective methods of enhancing screening attendance and preventing retinal complications and blindness are warranted.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interests.
Ethical approval
Ethical approval for this study was provided by Coventry and Warwickshire Ethics Committee.
Registered trial number: ISRCTN79653731.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.