
Abstract
Purpose:
To evaluate the association between spousal diabetes status and the prevalence of diabetic retinopathy in Chinese patients with type 2 diabetes.
Methods:
A cross-sectional community-based study was performed in 1510 patients with type 2 diabetes in Shanghai, China. Non-mydriatic digital fundus photography was used to detect diabetic retinopathy. Spousal diabetes status was assessed using a standardised interview questionnaire.
Results:
The prevalence of diabetic retinopathy was significantly lower in patients who had diabetic spouses, compared with those who did not (20.2% vs 29.1%, p ⩽ 0.01). The fully adjusted odds ratio for diabetic retinopathy in those had diabetic spouses was decreased by 36% (odds ratio = 0.64, 95% confidence interval = 0.42–1.00, p = 0.048). The negative correlation between spousal diabetes status and diabetic retinopathy was presented in patients with the duration of diabetes ⩾ 10 years, those with HbA1c ⩾ 7% and those not using lipid-lowering drugs (odds ratio = 0.31, 95% confidence interval = 0.13–0.74, p = 0.0082; odds ratio = 0.50, 95% confidence interval = 0.27–0.94, p = 0.031; odds ratio = 0.58, 95% confidence interval = 0.37–0.92, p = 0.021, respectively).
Conclusion:
We demonstrated that spousal diabetes was associated with a lower diabetic retinopathy prevalence in Chinese patients with type 2 diabetes.
Background
Diabetic retinopathy (DR), the most common microvascular complication, is the leading cause of vision loss and blindness in diabetic patients. Current research has demonstrated that intensive management of blood glucose, lipid profiles and blood pressure cannot completely prevent DR. 1
Sharing similar socioeconomic status and lifestyle with diabetic patients, spouses were prone to have a higher prevalence of diabetes. 2 In addition, interactions with spouses may directly affect antidiabetic therapeutic compliance. 3 Therefore, it is reasonable to speculate that spousal involvement might influence the prevalence of diabetes complications, via changing the lifestyle factors and medicine treatment in patients with diabetes. However, the epidemiological studies about the connection between spousal diabetes status and diabetes complications were not available. Therefore, the community-based study aimed to evaluate whether spousal diabetes status was associated with the prevalence of DR in Chinese patients with type 2 diabetes.
Subjects and methods
Study design
This cross-sectional survey was a community-based study consisting of type 2 diabetic patients from the Diabetic Health Record Systems at Pujiang Town, Minhang District, Shanghai, China. The details of the diabetes health management programme of Minhang District have been described. 4 The study was approved by the institutional review board of the Renji hospital, School of Medicine, Shanghai Jiao Tong University. Informed consent was obtained from each patient.
From December 2016 to April 2017, 1994 patients (63.8 ± 7.3 years old) participated in the study. The exclusion criteria were as follows: (1) those with type 1 diabetes or who were uncertain about the type of diabetes (n = 53); (2) those with uncompleted questionnaires or who refused to answer the question about spousal diabetes status (n = 301) and (3) those without a complete fundus photography examination (n = 130).
A half-day examination went through interviews and anthropometric measurements. We used the questionnaires to access the information about living situation and dosage of medications. Educational attainment was classified as primary education (junior high school and below) and higher education (high school or secondary school or above). The patients were asked, ‘Who do you live together with now’, if the answer was ‘living with my spouse’, they were asked ‘whether does your spouse have diabetes’. Patients who lived with spouses and the spouses reported a history of diabetes were grouped as those with diabetic spouses. Blood samples were collected before and after a meal of 100 g of steamed bread for patients fasted for at least 8 h. Urine samples were obtained from all of the patients.
Digital non-mydriatic fundus photography and image
High-quality fundus photographs centred on the macula of both sides were taken by a trained technologist using a Canon CR-2AF camera. The presence of DR was identified by an experienced ophthalmologist according to the criteria of the International Clinical Diabetic Retinopathy Disease Severity Scale.
Statistical analyses
Statistical analyses were carried out with SAS version 9.3 (SAS Institute, Inc., Cary, NC). Continuous variables were presented as the mean ± standard deviation or median (interquartile range).
Comparison of the baseline characteristics according to spousal diabetes status was completed using Student’s t-tests for continuous variables and χ2 tests or Fisher’s exact test for categorical variables. Simple correlation (Spearman rank correlation) and multiple stepwise logistic regression models were used to identify the factors independently associated with the prevalence of DR.
Multivariable-adjusted logistic regression models were used to evaluate the odds ratio (OR) for DR according to spousal diabetes status. Age, sex, current smoker, current drinker, use of hypoglycaemic drugs, use of antihypertensive drugs, use of lipid-lowering drugs, duration of diabetes, body mass index (BMI), systolic blood pressure (SBP), diastolic blood pressure (DBP), fasting plasma glucose (FPG), postprandial plasma glucose (PPG), HbA1c, triglyceride (TG), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C) and urine albumin-to-creatinine ratio (UACR) were included. We investigated whether the relationship varied with specific characteristics, including age (<65 or ⩾65 years), sex (male or female), obesity (yes or no), duration of diabetes (<10 years or ⩾10 years), HbA1c (<7% or ⩾7%), use of antihypertensive drugs (yes or no) and use of lipid-lowering drugs (yes or no). P-values for interaction were calculated using the coefficient of the cross-product interaction term added to the model. Two-sided p-values < 0.05 were considered statistically significant.
Results
In total, 1510 type 2 diabetic patients were included, with a mean age of 63.8 ± 7.3 years and a median diabetes duration of 8.5 years (4.6–11.6 years). The prevalence of DR in patients with diabetes was 28.1%. The prevalence of diabetic spouses was 11.5%.
The prevalence of DR was significantly lower in diabetic patients who had diabetic spouses, compared with those who did not (20.2% vs 29.1%, p ⩽ 0.01). We found that diabetic history of spouses was negatively associated with the odds of DR [OR = 0.64, 95% confidence interval (CI) = 0.41–0.98, p = 0.040], in addition to age, duration of diabetes, SBP, PPG, HbA1c and use of antihyperglycaemic drugs (Table 1). The odds of DR was decreased by 39% in an unadjusted model in patients with diabetic spouses (OR = 0.61, 95% CI = 0.42–0.92, p = 0.016). After adjustments for age, sex, current smoker, current drinker, use of hypoglycaemic drugs, use of antihypertensive drugs and lipid-lowering drugs, duration of diabetes, BMI, SBP, DBP, FPG, PPG, HbA1c, TG, TC, LDL-C, HDL-C and UACR, the association remained (OR = 0.64, 95% CI = 0.42–1.00, p = 0.048).
Pearson’s correlation and multiple stepwise logistic regression analysis of risk factors associated with prevalent DR.
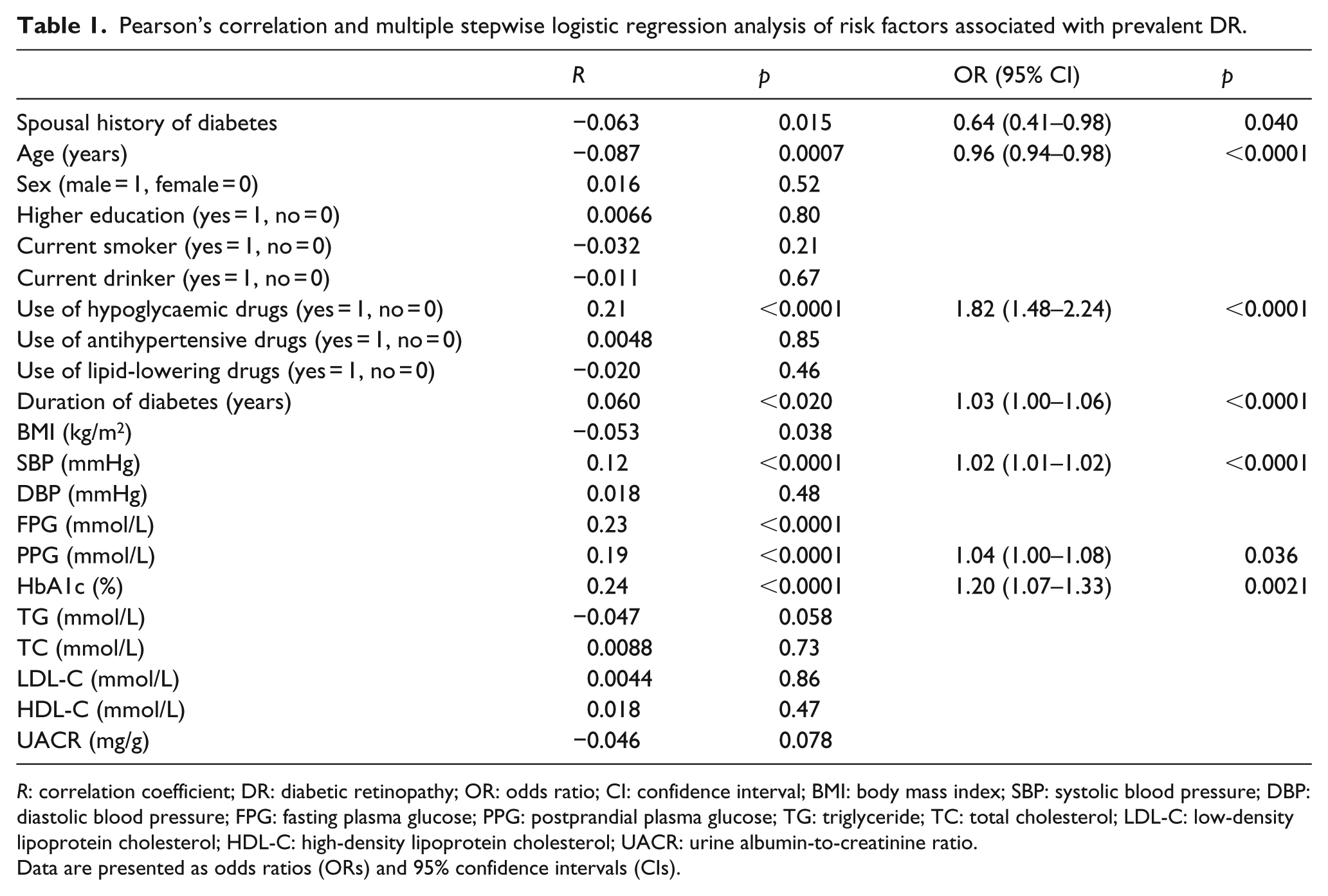
R: correlation coefficient; DR: diabetic retinopathy; OR: odds ratio; CI: confidence interval; BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; FPG: fasting plasma glucose; PPG: postprandial plasma glucose; TG: triglyceride; TC: total cholesterol; LDL-C: low-density lipoprotein cholesterol; HDL-C: high-density lipoprotein cholesterol; UACR: urine albumin-to-creatinine ratio.
Data are presented as odds ratios (ORs) and 95% confidence intervals (CIs).
In the subgroup analyses, there were no significant associations between spousal diabetes status and the risk of prevalent DR in patients with the duration of diabetes < 10 years, those with HbA1c < 7% or those using lipid-lowering drugs. However, the negative correlation between spousal diabetes status and DR was presented in patients with the duration of diabetes ⩾ 10 years, those with HbA1c ⩾ 7% and those not using lipid-lowering drugs (OR = 0.31, 95% CI = 0.13–0.74, p = 0.0082; OR = 0.50, 95% CI = 0.27–0.94, p = 0.031; OR = 0.58, 95% CI = 0.37–0.92, p = 0.021, respectively).
Discussion
In this cross-sectional study, we found that spousal diabetes history was associated with a lower DR prevalence in Chinese patients with type 2 diabetes. The association was independent of traditional risk factors, such as blood glucose levels, lipid profiles and control of blood pressure.
Spouses’ engagement contributed to better compliance with the treatment and glycaemic management in patients with diabetes. 5 A reasonable explanation might be spouses who could share the same responsibility, 6 rather than diabetic subjects who took responsibility alone. However, conflicting results have been presented. For example, spousal overprotection or diet-related pressure could lead to worse compliance for type 2 diabetic patients. 3 Therefore, future studies are required to explore the proper patterns of spouse involvement in type 2 diabetes management.
In the subgroup analyses, the associations between spousal diabetes status and the risk factors of DR were significant in the high-risk population. The positive spousal support might result in the better control of DR risk factors. Nevertheless, there is another possibility that the limited sample of DR in the low-risk population might affect the statistical power.
Serum lipids levels were reported to be associated with the prevalence of DR. 7 For example, plasma LDL-C was related to the presence of retinal hard exudates in the Atherosclerosis Risk in Communities (ARIC) study. 8 Fenofibrate treatment in type 2 diabetes reduced the requirement for laser treatment of DR. 9 Controversially, Yun et al. 10 found that there were no associations between serum lipids and DR among all stages of type 2 patients. We confirmed in the community-based study that the prevalence of DR was not associated with the plasma levels of TG, TC, HDL-C and LDL-C. The finding suggested that the relationship between lipids and retinopathy needs to be further investigated in future.
The limitations of the study must be mentioned. Firstly, it was a cross-sectional study. The association between the spousal diabetes status and the presence of DR might not be interpreted as causal. Secondly, the spousal diabetes might be under-reported, due to the high undiagnosed proportion and low awareness of type 2 diabetes in China. 11 Thirdly, although a wide spectrum of covariates was included in the adjustments, some residual or undetected confounding factors, such as dietary patterns, rating of psychological distress due to diabetes and marriage duration, could not be completely ruled out.
In summary, spousal diabetes is associated with a lower DR prevalence in Chinese patients with type 2 diabetes. Positive support from diabetic spouses might induce a collaborative management of risk factors and lower prevalence of DR in patients with type 2 diabetes. The pattern of the collaboration should be specified in the future studies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Natural Science Foundation of China (Grant No. 81670728), the Major Chronic Non-communicable Disease Prevention and Control Research, National Key R&D Program of China (Grant Nos 2016YFC1305600 and 2016YFC1305602), Research Fund of Shanghai Municipal Health and Family Planning Commission (Grant No. 201740054), the Incubating Program for Clinical Research and Innovation of Renji Hospital, School of Medicine, Shanghai Jiao Tong University (Grant No. PYZY16-020) and the Cultivating Funds of South Campus, Renji Hospital, School of Medicine, Shanghai Jiao Tong University (Grant Nos 2016PWZH01 and 2017PYQA05).