
Abstract
This study analyses discordance rates between attainment of therapeutic goals for apolipoprotein B100 (apoB) and both low-density lipoprotein–cholesterol (LDL-C) and non-high-density lipoprotein–cholesterol (non-HDL-C) in a sample of 152 patients with type 2 diabetes and chronic kidney disease from Gran Canaria (Spain), using treatment targets recommended by the American Diabetes Association/American College of Cardiology (ADA/ACC), the European Society of Cardiology/European Atherosclerosis Society (ESC/EAS) and by a Spanish population-based study. Among subjects with LDL-C levels at therapeutic goal, apoB was above target in 16.3% (ADA/ACC), 6.5% (ESC/EAS) and 39.1% (population-based criteria), and among subjects with non-HDL-C levels at therapeutic goal, apoB was above target in 10.5% (ADA/ACC), 1.2% (ESC/EAS) and 29.6% (population-based criteria). These findings show that clinical management would be very differently altered depending on the criteria used to set treatment targets for apoB. Cut-off points derived from population data identify a greater number of subjects suitable for a more intensive lipid-lowering therapy.
Keywords
Introduction
Low-density lipoprotein–cholesterol (LDL-C) has been considered the cornerstone for assessment of cardiovascular risk and the primary therapeutic target of lipid-lowering therapy. However, although LDL is the most atherogenic lipoprotein, some triglyceride-rich lipoproteins, including intermediate-density lipoproteins and chylomicrons remnants, are also involved in the atherosclerotic process. Several large prospective studies have shown that measurements of non-high-density lipoprotein–cholesterol (non-HDL-C) and apolipoprotein B100 (apoB), both of which inform about the levels of the whole of atherogenic lipoproteins, are better predictors of cardiovascular disease than LDL-C.1–5 The Third Report of the National Cholesterol Education Program (NCEP) advocated the use of non-HDL-C as a secondary target of therapy for subjects with elevated triglycerides. 6 Later, a consensus statement endorsed by the American Diabetes Association (ADA) and the American College of Cardiology (ACC) Foundation suggested that, in addition to LDL-C, both non-HDL-C and apoB should be considered for evaluation of cardiovascular risk among subjects with cardiometabolic syndrome. 7 In this statement, LDL-C of 100 mg/dL were considered equivalent to non-HDL-C levels of 130 mg/dL and apoB levels of 90 mg/dL, and LDL-C levels of 70 mg/dL were considered equivalent to non-HDL-C levels of 100 mg/dL and apoB levels of 80 mg/dL. More recently, the guidelines of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS) 8 equated LDL-C levels of 70 mg/dL and non-HDL-C levels of 100 mg/dL to apoB levels of 80 mg/dL, and LDL-C levels of 100 mg/dL and non-HDL-C levels of 130 mg/dL to apoB levels of 100 mg/dL.
However, data from the Third National Health and Nutrition Examination Survey and the Framingham Offspring Study have shown that recommended cut-off points for LDL-C, non-HDL-C and apoB do not correspond to the same percentiles of the general US population. 9 In this regard, other American scientific organizations, namely, the American Association of Clinical Chemistry 10 and the National Lipid Association, 11 have proposed that treatment goals should be set so that the apoB and lipid cut-off points are equivalent in terms of the distribution of values in the general population.
Information on population-equivalent values for LDL-C, non-HDL-C and apoB outside the USA is scant. Recently, Martinez-Hervas et al. 12 estimated cut-off points for apoB and non-HDL-C equivalent to established LDL-C targets in a healthy Spanish population. According to their data, LDL-C goals of 70 and 100 mg/dL would be equivalent to non-HDL-C levels of 100 and 120 mg/dL and apoB levels of 70 and 80 mg/dL.
The aim of this study was to compare the degree of agreement between attainment of treatment targets for apoB and cholesterol variables proposed by the ADA/ACC, the ESC/EAS and Martinez-Hervas et al. in a cohort of patients with type 2 diabetes and high or very high cardiovascular risk from the island of Gran Canaria, Spain. The potential impact of using one or other thresholds on clinical management decisions is discussed.
Methods
Study subjects
The study population was composed of patients with type 2 diabetes who were enrolled in the Caracterización de la Enfermedad Renal Crónica Asociada a Diabetes (CERCA-Diabetes) Study between February 2011 and December 2012. The CERCA-Diabetes Study is an observational survey directed to characterize the population with type 2 diabetes and chronic kidney disease in the south area of the Gran Canaria Island. All new (incident) patients attending the Advanced Chronic Kidney Disease Office of the Hospital Universitario Insular are invited to participate in this study. According to our usual practice, patients are referred to this medical facility when they present chronic kidney disease stages 4 or 5, as defined by the National Kidney Foundation’s Kidney Disease Outcomes and Quality Improvement Initiative (KDOQI). 13 Only individuals with a diagnosis of type 2 diabetes and simultaneous measurements of apoB, total cholesterol, HDL-C and triglycerides were eligible for the present investigation. This study has been approved by the Ethical Committee of the Hospital Universitario Insular, and all subjects signed informed consent before participation. Details of the design of the survey have been described previously. 14
Laboratory measurements
After an overnight fasting, participants provided an urine specimen and underwent blood extraction. Total cholesterol, HDL-C and apoB were measured with an AU2700 chemistry-immuno analyzer (Olympus America, Melville, NY). ApoB determinations were standardized to the World Health Organization–International Federation of Clinical Chemistry (WHO-IFCC) International Reference Materials for apoB (SP3-07). LDL-C was estimated using the Friedewald formula, and non-HDL-C was calculated as the difference between total cholesterol and HDL-C.
Statistical analyses
According to the NCEP 5 and the ESC/EAS, 8 respective therapeutic targets for LDL-C and non-HDL-C were considered at <70 mg/dL and <100 mg/dL for very high-risk patients (those with established cardiovascular disease), and <100 mg/dL and <130 mg/dL for high-risk patients (those without established cardiovascular disease). Concordance between attainment of these targets and ADA/ACC apoB goals was estimated accepting that LDL-C levels of 70 mg/dL and non-HDL-C levels of 100 mg/dL are equivalent to apoB values of 80 mg/dL, and LDL-C levels of 100 mg/dL and non-HDL-C levels of 130 mg/dL are equivalent to apoB values of 90 mg/dL. Similarly, concordance between lipid and apoB goals proposed by the ESC/EAS was calculated accepting that LDL-C levels of 70 mg/dL and non-HDL-C levels of 100 mg/dL are equivalent to apoB values of 80 mg/dL, and LDL-C levels of 100 mg/dL and non-HDL-C levels of 130 mg/dL are equivalent to apoB values of 100 mg/dL. Finally, for concordance analyses between cholesterol goals and apoB goals proposed by Martinez-Hervas et al., 12 therapeutic targets for LDL-C, non-HDL-C and apoB were, respectively, <70 mg/dL, <100 mg/dL and <70 mg/dL for patients with established cardiovascular disease, and <100 mg/dL, <120 mg/dL and <80 mg/dL for patients without established cardiovascular disease.
The kappa test was used to assess the agreement between attainment of cholesterol and apoB targets. Agreement was considered moderate when the κ statistic belonged to the interval 0.41−0.60, good if belonged to the interval 0.61−0.80 and finally very good if κ was greater than 0.8. 15
In order to assess the influence of hypertriglyceridemia on the performance of the three analysed criteria, the study population was categorized according to serum levels of triglycerides (<100 mg/dL, 100–149 mg/dL, 150–199 mg/dL and ≥200 mg/dL), and concordance and discordance rates between attainment of therapeutic goals for apoB and both LDL-C and non-HDL-C were calculated for each group.
Results
The sample was composed of 152 subjects. Due to the nature of the original survey (CERCA-Diabetes Study), 77.9% of participants had chronic kidney disease [glomerular filtration rate (GFR) < 60 mL/min], although none of them had begun renal replacement therapy, and 13.2% had nephrotic proteinuria (equal or greater than 3.0 g/24 h). Most subjects (80.5%) were taking hypolipidemic treatment (59.7% statins monotherapy, 16.9% statins combined with fibrates and/or ezetimibe, and 3.9% fibrates alone or combined with ezetimibe). Table 1 shows a clinical and biochemical profile of the population. LDL-C could not be calculated in three subjects with triglycerides higher than 400 mg/dL. Table 2 shows the proportions of patients achieving clinical targets recommended by the ADA/ACC, the ESC/EAS and Martinez-Hervas et al. Tables 3 to 5 show the percentages of concordance between achievement of cholesterol and apoB goals, in the whole of the sample, by using the cut-off points, respectively, proposed by the three sets of criteria.
Characteristics of the population.
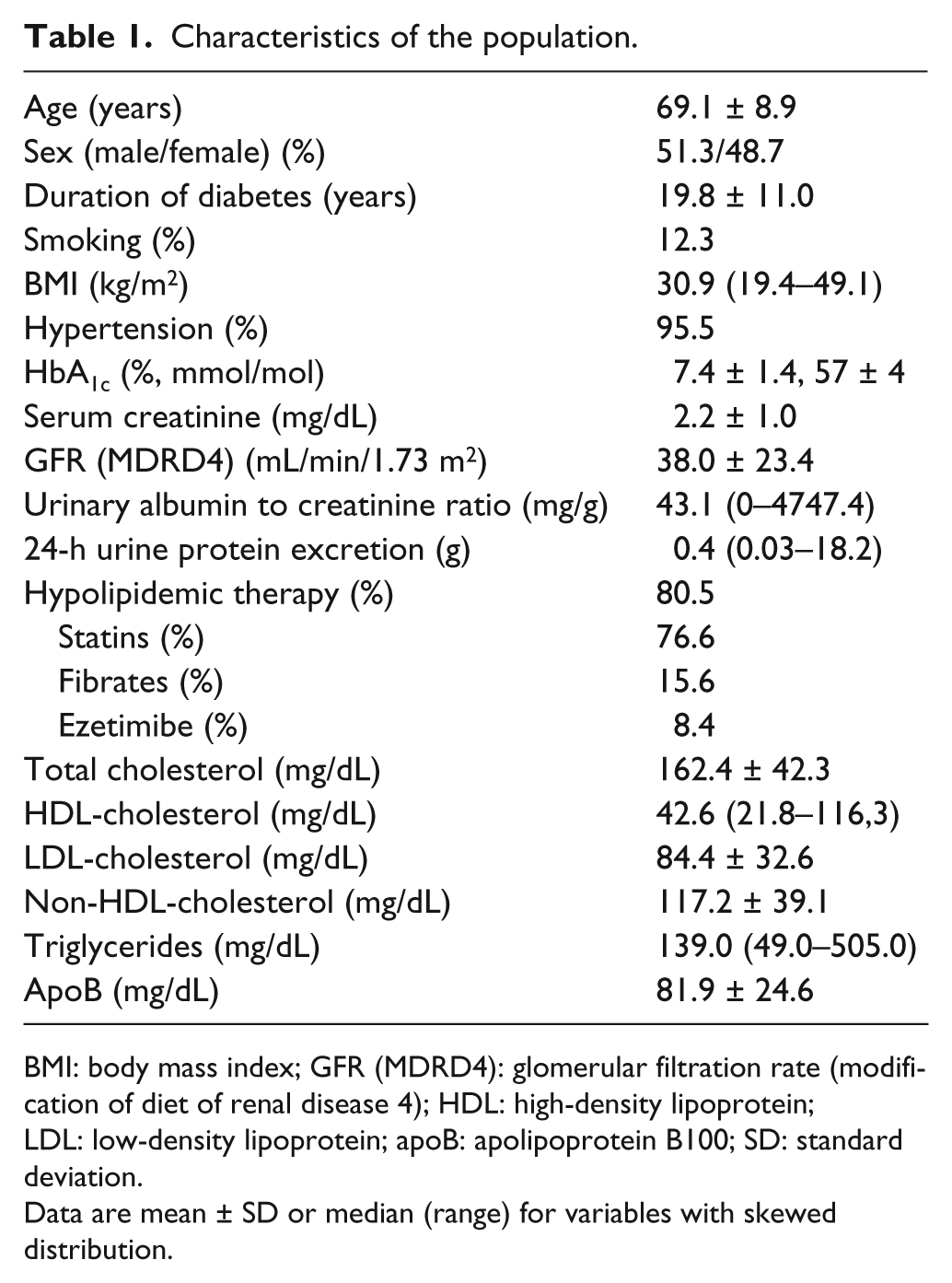
BMI: body mass index; GFR (MDRD4): glomerular filtration rate (modification of diet of renal disease 4); HDL: high-density lipoprotein; LDL: low-density lipoprotein; apoB: apolipoprotein B100; SD: standard deviation.
Data are mean ± SD or median (range) for variables with skewed distribution.
Proportions of patients achieving therapeutic goals according to the three analysed criteria.
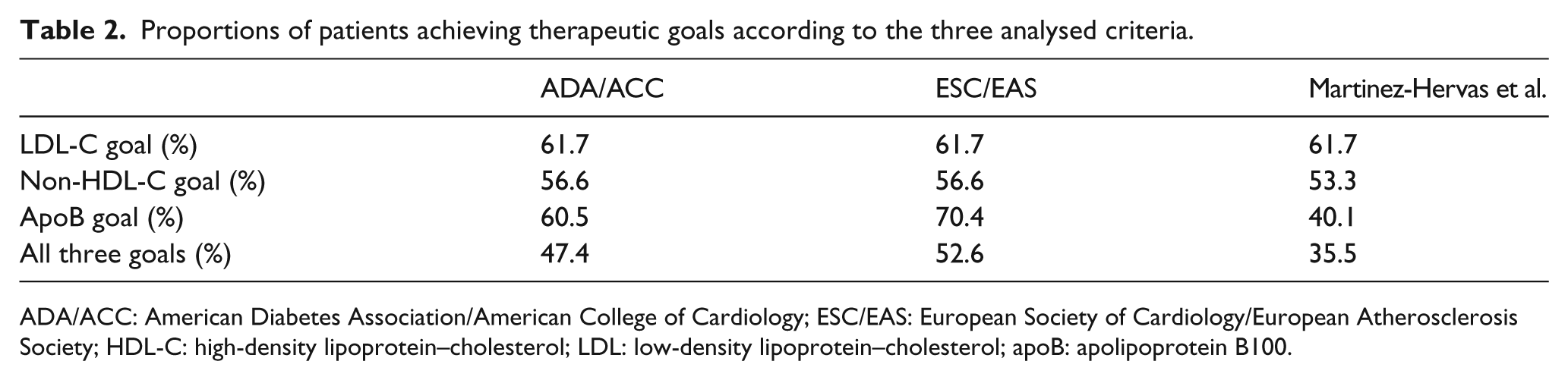
ADA/ACC: American Diabetes Association/American College of Cardiology; ESC/EAS: European Society of Cardiology/European Atherosclerosis Society; HDL-C: high-density lipoprotein–cholesterol; LDL: low-density lipoprotein–cholesterol; apoB: apolipoprotein B100.
Concordance and discordance rates between apoB and cholesterol goals in the whole sample, as defined by the American Diabetes Association/American College of Cardiology Foundation consensus statement.
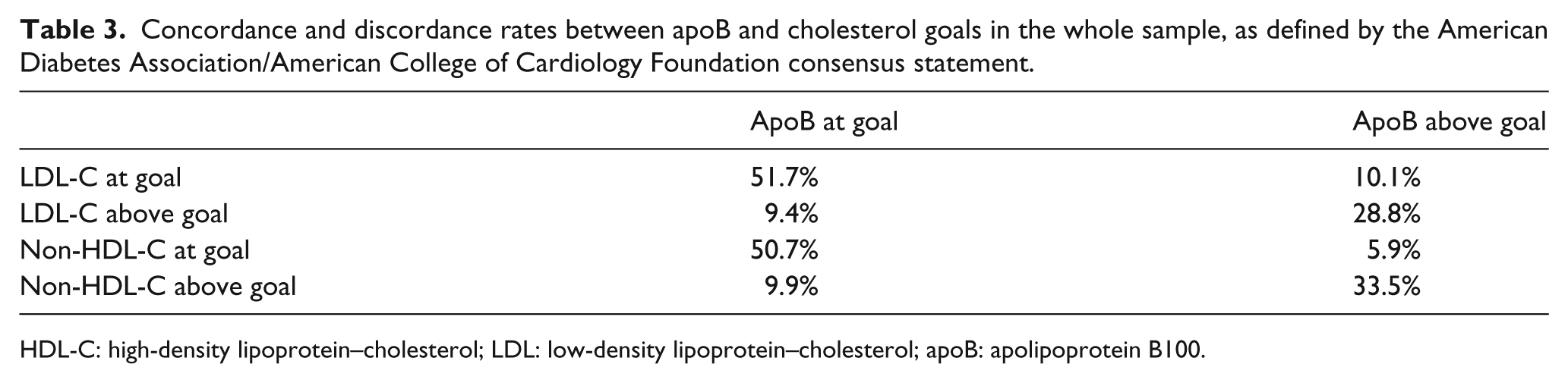
HDL-C: high-density lipoprotein–cholesterol; LDL: low-density lipoprotein–cholesterol; apoB: apolipoprotein B100.
Concordance and discordance rates between apoB and cholesterol goals in the whole sample, as defined by the guidelines of the European Society of Cardiology/European Atherosclerosis Society.
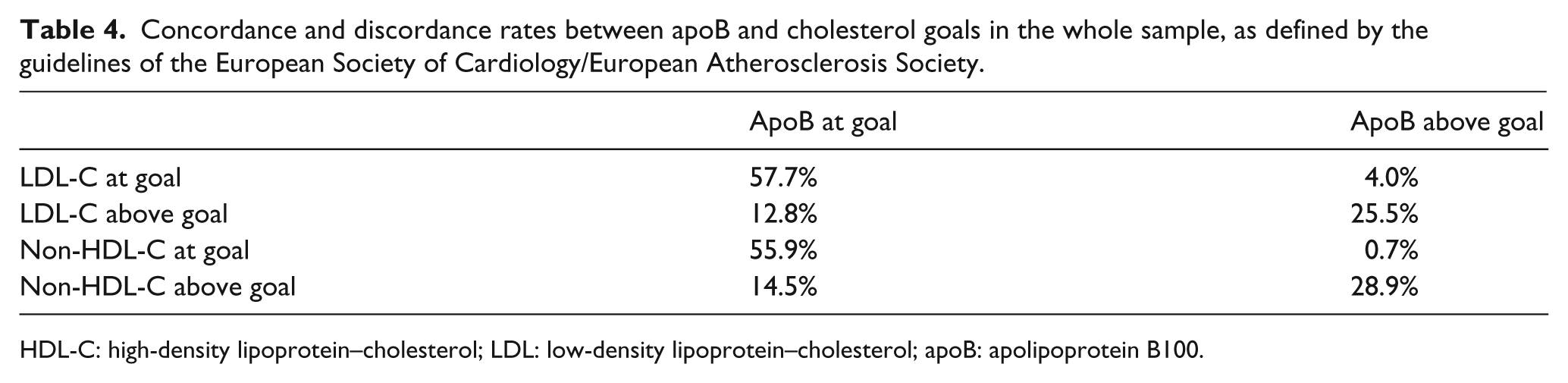
HDL-C: high-density lipoprotein–cholesterol; LDL: low-density lipoprotein–cholesterol; apoB: apolipoprotein B100.
Concordance and discordance rates between apoB and cholesterol goals in the whole sample, as proposed by Martinez-Hervas et al. for Southern European population.
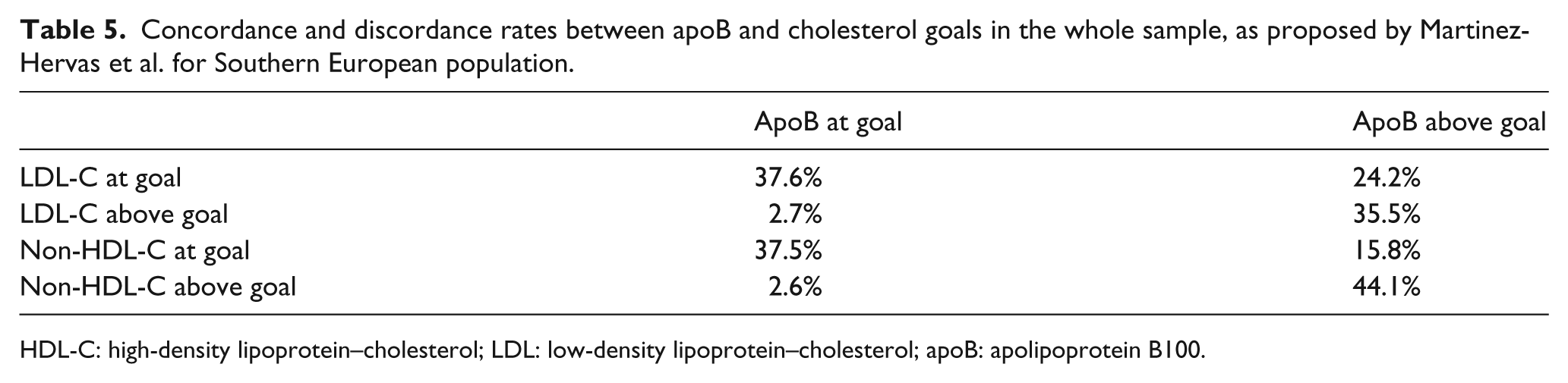
HDL-C: high-density lipoprotein–cholesterol; LDL: low-density lipoprotein–cholesterol; apoB: apolipoprotein B100.
Per the ADA/ACC guidelines, among the 92 subjects with LDL-C levels at therapeutic goal, 15 of them (16.3%) had levels of apoB above target. On the contrary, 14 of the 57 (24.6%) subjects with LDL-C levels above therapeutic goal had apoB levels at goal. Regarding non-HDL-C, only 9 of the 86 subjects (10.5%) with non-HDL-C levels at goal had apoB levels above the equivalent target, whereas among the 66 subjects with non-HDL-C above goal, levels of apoB were within target in 15 cases (22.7%). The kappa test indicated a moderate measure of agreement between LDL-C and apoB (κ = 0.59) and a good measure of agreement between non-HDL-C and apoB (κ = 0.67). On the whole, following the ADA/ACC guidelines, the measurement of apoB would have identified only nine individuals (5.9% of the entire sample) in whom both LDL-C and non-HDL-C were at goal, but apoB was above the recommended cut-off point.
Using the recommendations of the ESC/EAS, which advise a less stringent objective for apoB among patients with high cardiovascular risk (100 mg/dL), the number of subjects with LDL-C levels at therapeutic goal who had increased concentrations of apoB lowered to 6 (6.5%), while 19 of 57 subjects (33.3%) with LDL-C above recommended goal had adequate concentrations of apoB. Remarkably, only 1 of the 86 subjects (1.2%) with non-HDL-C at goal had increased concentrations of apoB according to the ESC/EAS criteria, while 22 of 66 subjects (33.3%) with non-HDL-C above target had apoB at goal. The kappa test showed that the agreement between apoB and both LDL-C and non-HDL-C was good (κ = 0.63 and 0.68, respectively).
According to the proposal by Martinez-Hervas et al. for population from Southern Europe, 36 of the 92 subjects (39.1%) with levels of LDL-C at goal had values of apoB above the recommended therapeutic target, whereas only 4 of 57 subjects (7.0%) with LDL-C levels over goal had apoB levels within target. In the same way, among the 81 participants with measures of non-HDL-C at goal, 24 of them (29.6%) had apoB levels higher than recommended goal. In contrast, only 4 of 71 (5.6%) subjects with non-HDL-C levels above goal had apoB levels at goal. The agreement between attainment of cut-off points for LDL-C and apoB suggested by Martinez-Hervas et al. was moderate (κ = 0.49), while the agreement between attainment of cut-off points for apoB and non-HDL-C was good (κ = 0.64). On the whole, using the proposal by these authors, the measurement of apoB would have identified 23 subjects (15.1% of the whole sample) in whom apoB was above goal, but both LDL-C and non-HDL-C were within recommended targets.
Table 6 shows concordance and discordance rates between apoB and both LDL-C and non-HDL-C across categories of serum triglyceride levels (<100 mg/dL, 100–149 mg/dL, 150–199 mg/dL and ≥200 mg/dL). Most individuals uniquely identified by the criteria of Martinez-Hervas et al. as having above-target apoB along with well-controlled cholesterol levels belonged to the subgroups of subjects with serum triglycerides ranging between 100 and 199 mg/dL.
Concordance and discordance rates between apoB and cholesterol goals, as defined by the three analysed criteria, according to the levels of serum triglycerides of the population.
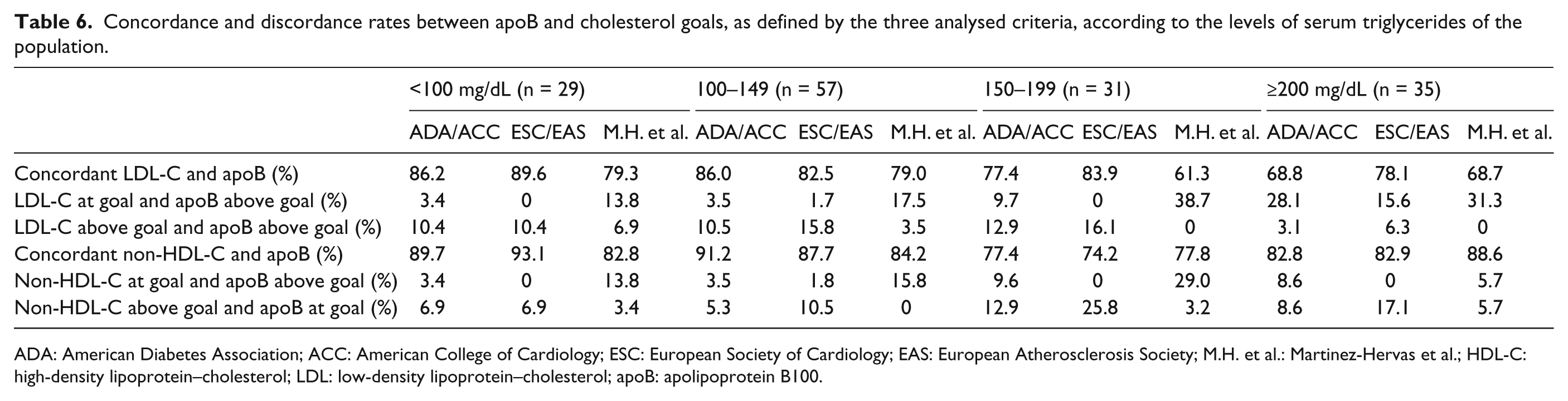
ADA: American Diabetes Association; ACC: American College of Cardiology; ESC: European Society of Cardiology; EAS: European Atherosclerosis Society; M.H. et al.: Martinez-Hervas et al.; HDL-C: high-density lipoprotein–cholesterol; LDL: low-density lipoprotein–cholesterol; apoB: apolipoprotein B100.
Discussion
Lowering LDL-C is the primary objective in the management of dyslipidemia in patients at risk of cardiovascular disease. However, patients who have achieved LDL-C levels below the currently recommended targets may still remain at residual risk. The measure of apoB, a more reliable marker of the number of all potentially atherogenic particles, has been found to be a better predictor of cardiovascular disease than LDL-C,1–6 whereas its possible superiority over non-HDL-C is under discussion.16,17 The advantage of apoB measurement could be particularly relevant in patients treated with statins, in whom several interventional studies have demonstrated that the risk of subsequent coronary events relates more closely to the level of apoB than to the level of LDL-C.18,19 In spite of these evidences, apoB has not gained definite acceptance for routine use in cardiovascular risk assessment, with one of the possible reasons being the lack of universally recognized thresholds for clinical decision-making.
In this study, we have compared the potential clinical utility of three proposals for establishing apoB cut-off points equivalent to those for LDL-C and non-HDL-C in a sample of subjects with type 2 diabetes and chronic kidney disease. Following the guidelines of the ADA/ACC, the percentage of patients achieving recommended levels of apoB was similar to the percentage achieving LDL-C goals, and higher than the percentage achieving non-HDL-C goals. In fact, while only 5.9% of subjects with cholesterol indices within goals had apoB levels above the recommended goal, between 9% and 10% of the participants had apoB at goal despite elevated values of LDL-C and/or non-HDL-C.
In the case of using the guidelines of the ESC/EAS, the results would be more extreme. There was only one individual with both LDL-C and non-HDL above goals in whom the level of apoB was higher than the recommended cut-off. Thus, virtually, all cases in which there was discordance between attainment of cholesterol and apoB goals were due to increased LDL-C and/or non-HDL-C with adequately controlled apoB.
Several experts have suggested that thresholds for apoB and lipid measures should be based on the distributions of their values in the general population. Recently, by studying 1501 clinically healthy subjects between 18 and 80 years of age from the city of Valencia (Spain), Martinez-Hervas et al. 12 proposed equivalent cut-off values for LDL-C, non-HDL-C and apoB for Southern European population. According to their data, an LDL-C concentration of 100 mg/dL would correspond to values of non-HDL-C of 120 mg/dL and apoB of 80 mg/dL, and an LDL-C concentration of 70 mg/dL would correspond to values of non-HDL-C of 100 mg/dL and apoB of 70 mg/dL. Using theses more strict cut-offs for apoB, 39.1% of subjects with LDL-C at goal and 29.6% of subjects with non-HDL-C at goal had increased levels of apoB. On the whole, apoB would have identified 23 individuals (15.1% of the entire sample) suitable for a more intensive lipid-lowering therapy. In contrast, only six subjects (3.9%) had apoB at goal despite elevated values of LDL-C and/or non-HDL-C.
Obviously, this cross-sectional study does not permit to withdraw definitive conclusions regarding which of the three assessed proposals would be more appropriate for risk evaluation and adequacy of treatment in our population. However, the main rationale for the incorporation of apoB to the clinical assessment of subjects with high cardiovascular risk, such as those examined in this study, should be the detection of individuals in whom further intensification of lipid-lowering therapy might be considered. It is well known that due to a marked increase in small LDL particle concentrations, the presence of diabetes and insulin resistance is associated with a greater overall number of LDL particles that is not fully apparent in the conventional lipid panel. 20 Therefore, it should be expected that LDL-C and, to a lesser extension, non-HDL-C could underestimate the total number of atherogenic particles in our population of subjects with type 2 diabetes. Moreover, most participants in our study were taking statin treatment and has been demonstrated that lipid-lowering therapy reduces LDL-C and non-HDL-C to a greater extension than apoB.5,21 Taking into account all these considerations, it is sound to think that the apoB cut-off points proposed by the ADA/ACC and the ESC/EAS consensus, which would identify a minimal proportion of subjects with discordantly high apoB, are too high to be used in our population. Alternatively, using cut-off points proposed by Martinez-Hervas et al., 12 based on corresponding values of LDL-C, non-HDL-C and apoB in terms of population-level, we found that, among subjects with LDL-C and non-HDL-C at goal, 39.1% and 29.6%, respectively, had apoB values above the recommended goal. These percentages probably provide a better reflection of the expected cholesterol depletion of LDL particles in a greater number of subjects with type 2 diabetes.
Interestingly, most subjects in whom apoB was the only measure above goal according to the criteria proposed by Martinez-Hervas et al., but not according to the ADA/ACC or ESC/EAS criteria, had serum triglyceride levels between 100 and 199 mg/dL. This means that the use of adequate cut-off points for apoB could be especially important to detect individuals at residual risk among subjects with normal to borderline high serum triglyceride levels. In this regard, although apoB has been traditionally considered an alternative secondary target of therapy for patients with hypertriglyceridemia, 6 its determination could be also very useful in patients with diabetes and normal levels of triglycerides. In fact, previous data indicate that apoB is better than non-HDL-C for identifying normotriglyceridemic patients with type B LDL phenotype, 22 probably as a consequence that small dense LDL particles begin to predominate once triglyceride levels exceed 100 mg/dL. 23
Finally, it must be noted that rates of discordance that we found with the proposal of Martinez-Hervas et al. were similarly observed applying the ADA/ACC cut-off points in a recent study evaluating a greater pool of lipid determinations performed in subjects with diabetes and hypertriglyceridemia from the United States. 24 This observation indicates that adequate cut-off points for apoB could diverge across different populations.
This study is subjected to several limitations. The size of the sample was small, and the population was mostly composed of old patients with a high prevalence of advanced chronic kidney disease and cardiovascular complications. The measurement of apoB might be very relevant in this kind of subjects with high cardiovascular risk, especially after the demonstration that hypolipidemic treatment is effective to reduce the incidence of major atherosclerotic events in patients with advanced kidney disease. 25 However, chronic renal failure is accompanied by specific alterations of lipoprotein metabolism, including the accumulation of partially catabolized triglyceride-rich apoB-containing lipoproteins. 26 Moreover, 13% of our patients had nephrotic syndrome, a condition typically characterized by marked increases in serum concentrations of cholesterol, triglycerides and apoB. 27 Therefore, it is not possible to know whether our results are translatable to patients with normal kidney function. Finally, another limitation is related to the fact that our patients were receiving different types of lipid-lowering therapy. As stated above, statin treatment does not reduce apoB to the same extension as cholesterol indices,5,21 and we cannot ascertain whether medical treatment affected the concordance rates between apoB and cholesterol targets.
In summary, this study reflects that if apoB was incorporated to routine clinical assessment of patients with type 2 diabetes, clinical decisions could be seriously affected by the choice of the criteria used to set treatment targets. Although prospective studies are needed to extract definitive conclusions, cut-off points based on reference populations seem more appropriate for clinical decision-making.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This study was funded by the Spanish Ministry of Science and Innovation (IP 11 1880).