
Abstract
Hypertension is an extremely common co-morbid condition in diabetes leading to acceleration in micro-vascular and macro-vascular complications. The use of anti-hypertensives in diabetic patients should be considered in the context of preventing the development of complications. Various factors contribute to the pathophysiology of diabetes in hypertension. With the advancements in technology, the understanding of the pathophysiological mechanisms has increased, and this can contribute in providing evidence for beneficial role of certain anti-hypertensives. Many clinical trials have been carried out for use of diuretics, beta blockers, calcium channel blockers, angiotensin-converting enzyme inhibitors and angiotensin receptor blockers. The present review gives an overview of pathophysiological mechanisms of hypertension and diabetes in addition to the details of clinical trials of anti-hypertensives in diabetic patients. This is an attempt to provide some evidences for the clinicians, which may serve as a guide for use of anti-hypertensives in clinical practice.
Introduction
Diabetes mellitus (DM) and hypertension are two of the most common diseases, and the frequency of both diseases increases with the advancing age. 1 Hypertension is an extremely common co-morbid condition in diabetes, affecting approximately 20%–60% of patients with diabetes, depending on obesity, ethnicity and age. 2 Furthermore, the usual finding in long-term survivors of diabetes is the absence of hypertension. 3 Hypertension leads to a two- to threefold increase in major cardiovascular (CV) events in both type 1 and type 2 diabetes. In type 1 diabetes, hypertension may reflect the onset of diabetic nephropathy, 4 while in type 2 diabetes, hypertension is often present as a part of the metabolic syndrome of insulin resistance, including central obesity and dyslipidaemia. 5 Hypertensive diabetic patients are at increased risk of diabetes-specific complication including retinopathy and nephropathy. 6
Despite the benefit of blood pressure (BP) lowering and glycaemic control, rates of detection and control of the conditions have been suboptimal. Since both DM and hypertension are important risk factors for cardiovascular diseases (CVDs),7,8 management of hypertension and DM is therefore essential for the reduction of CV events and mortality. Up to 75% of CVDs in diabetes may be attributable to hypertension, leading to recommendations for more aggressive treatment (i.e. reducing BP to <130/85 mmHg) in persons with coexistent diabetes and hypertension. 9 It has been demonstrated by several trials that in patients with diabetes, reduction of diastolic BP to about 80 mmHg and of systolic BP to about 130 mmHg is accompanied by a further reduction in CV events or diabetes-related micro-vascular complications, in comparison with patients with less stringent BP control.10 –14 Furthermore, in the UK Prospective Diabetes Study (UKPDS) epidemiological study, each 10-mmHg reduction in mean systolic BP was found to be associated with reductions in risk of 12% for any complication related to diabetes, 11% for myocardial infarction (MI) and 13% for micro-vascular complications. 13 BP treatment versus placebo has been effective in reducing complications of diabetes15,16 and has helped to define the optimal level of BP control.11,13,17 An aggressive approach to the diagnosis and treatment of hypertension in patients with diabetes is required in order to substantially reduce the incidence of both macro-vascular and micro-vascular complications. The objective of the current review is to give a brief account of the pathophysiological mechanisms underlying hypertension and diabetes and to familiarize the readers with the choice of anti-hypertensives in diabetic patients with reference to clinical trials being carried out for the same. This is an attempt to provide some evidences for the clinicians, which may serve as a guide for use of anti-hypertensives in clinical practice.
Prevalence
Approximately 50% of people with diabetes are hypertensive, and 35%–75% of complications of diabetes are thought to be due to hypertension.18,19 When hypertension coexists with diabetes, the risk of CVDs is increased by 75%, which further contributes to the overall morbidity and mortality of an already high-risk population.9,20 Extensive epidemiological evidence indicates that diabetic individuals with hypertension have greatly increased risks of CVD, renal insufficiency and diabetic retinopathy.6,21 In both the type 1 diabetic and non-diabetic populations, hypertension is underdiagnosed, 22 and the timing and presentation of hypertension differs between type 1 and type 2 diabetes. In type 1 diabetes, hypertension develops after several years of the disease and usually reflects the development of diabetic nephropathy ultimately affecting ~30% of individuals with type 1 diabetes.4,23 In type 2 diabetes, hypertension may be present at the time of diagnosis or even before the development of hyperglycaemia. 24 Approximately 20%–60% of patients with type 2 diabetes will develop hypertension, depending on age, ethnicity and obesity. In some ethnic groups, diabetic nephropathy may be the primary determinant of hypertension in type 2 diabetes. This has been documented in Pima Indians. 25 About 25%–47% of persons with hypertension have insulin resistance or impaired glucose tolerance. 26 Several confounding factors, present in type 2 diabetes, make the assessment of the prevalence of hypertension attributable to diabetes difficult. Type 2 diabetic patients are older and have a greater degree of adiposity than non-diabetic patients. The clustering of hypertension, glucose intolerance or frank type 2 diabetes, hyperlipidaemia, central obesity and insulin resistance has been documented in several populations. 5 Thus, increased BP in these individuals may represent the ageing or obesity of the population. However, after adjusting for age and weight, the prevalence of hypertension is still 1.5 times higher in diabetic groups. 24 The relationship between diabetic neuropathy and arterial hypertension is less clear. However, some epidemiological studies suggest that hypertension may also be a contributory factor for this condition. 6
Pathophysiology
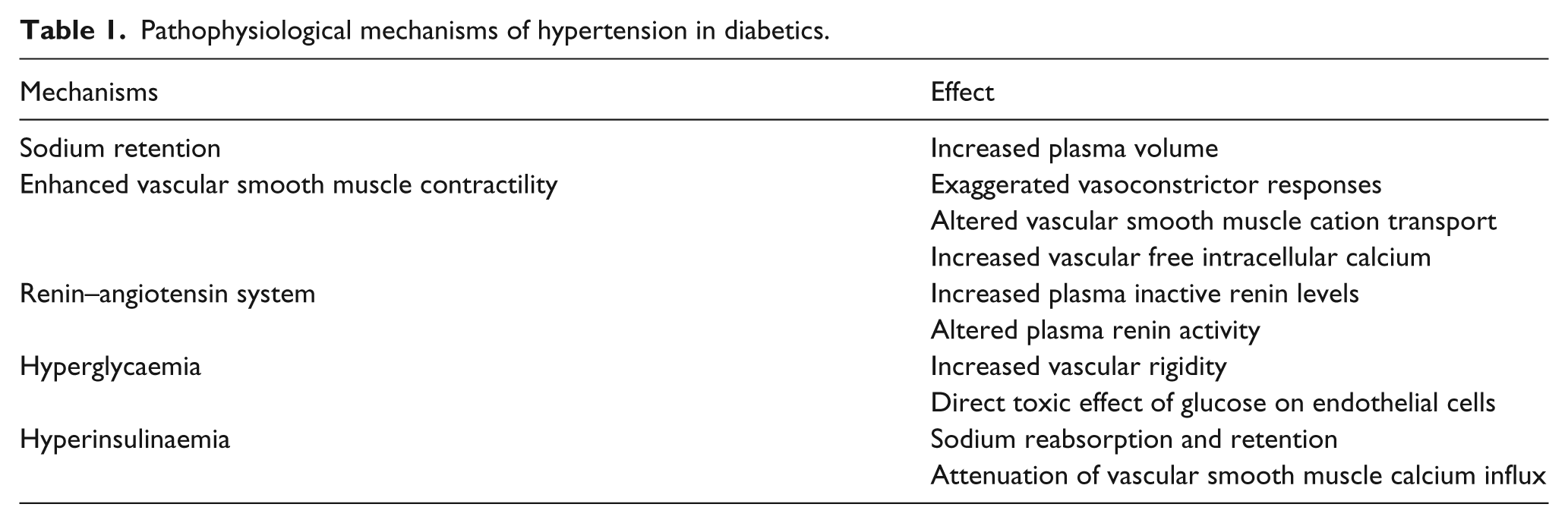
Hypertension in diabetic individuals has certain characteristics similar to hypertension in the elderly persons. 27 In diabetic–hypertensive individuals, premature atherosclerosis probably contributes to premature ageing changes of the vasculature,28,29 which plays a key role in the relatively high prevalence of isolated systolic hypertension and decreased baroreceptor sensitivity in young diabetic individuals. 30 The decreased baroreceptor sensitivity is followed by the development of clinical neurological disease in young diabetic pateints. 30 Decreased baroreceptor reflex sensitivity as well as altered cardiac innervation may partially explain the marked variability of BP.28,30,31 These latter characteristics suggest premature ageing of the CV system in diabetic individuals with coexistent hypertension. 27 In addition to premature vascular ageing and its effect on vascular rigidity and resistance, other factors contribute to the pathophysiology of hypertension in diabetes (Figure 1). Moreover, sodium retention, hyperglycaemia, hyperinsulinaemia (Figure 2), enhanced vascular smooth muscle contractility and renin–angiotensin system are major pathological mechanisms responsible for hypertension in diabetic patients (Table 1).
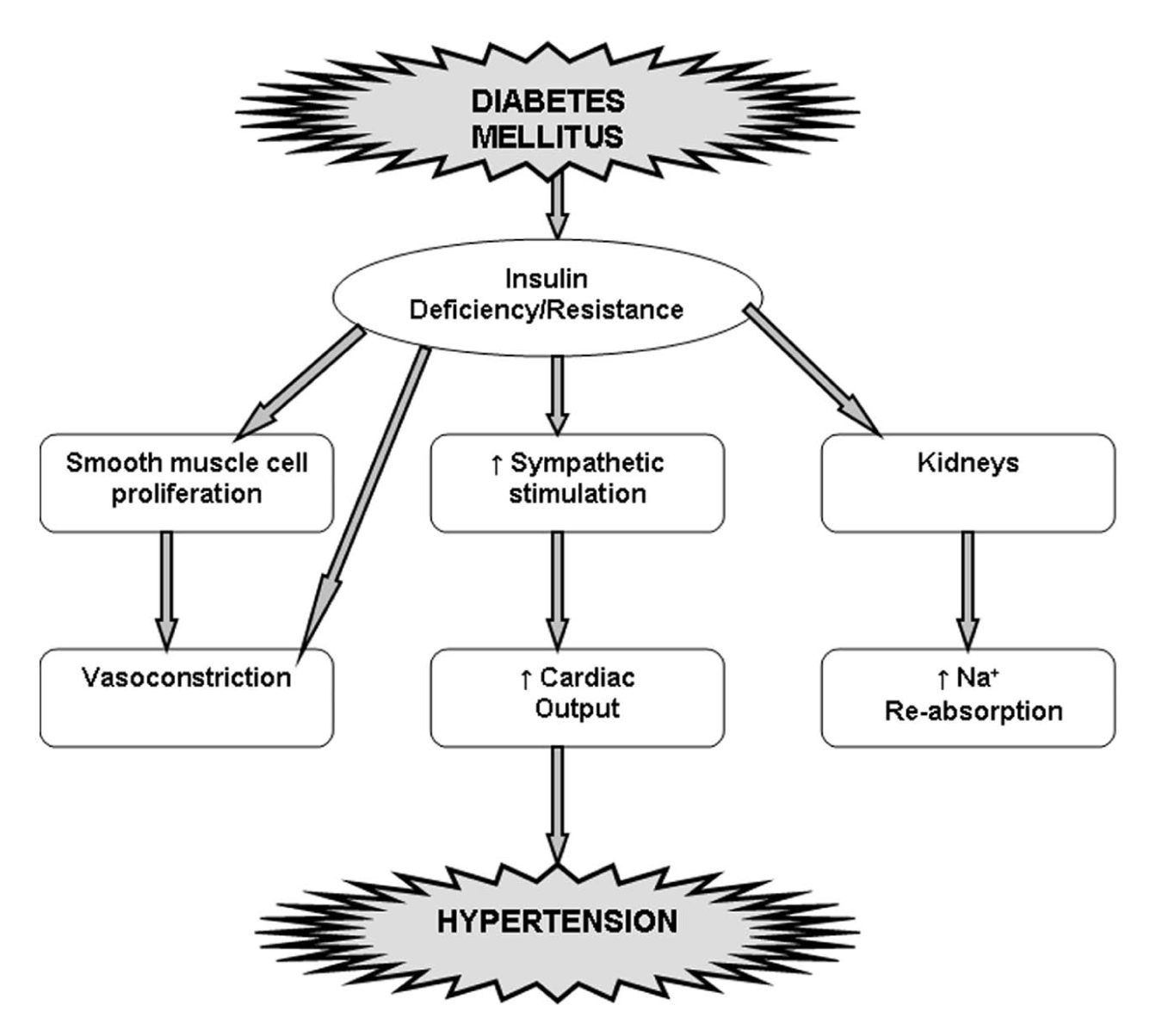
Relationship between diabetes and hypertension.
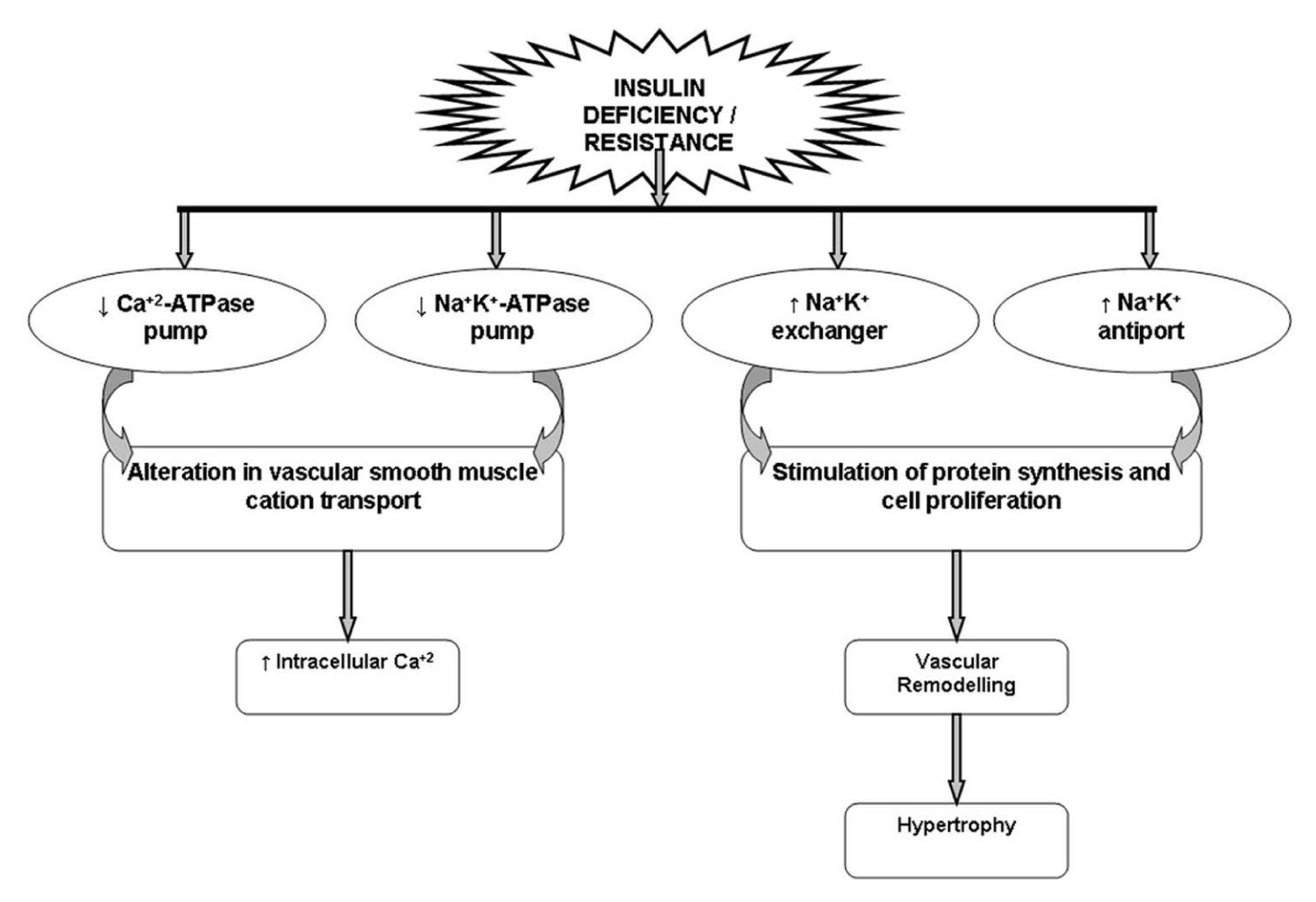
Co-relation between insulin and exchange pumps.
Pathophysiological mechanisms of hypertension in diabetics.
Choice of anti-hypertensives
At the doses available for clinical use, most anti-hypertensives will produce a reduction in systolic or diastolic BP of 5%–10% in patients with mild or moderate hypertension. 2 Most patients require more than one agent to control BP. Several factors are important in selecting anti-hypertensive agents for use in hypertensive patients with diabetes.
Diuretics
Thiazide diuretics
Thiazide diuretics are the first choice of agents in non-diabetic patients, but there has been a tendency to avoid their use in patients with diabetes due to concerns over adverse metabolic effects, despite evidence that these are minimal when lower dose agents are used. 32 Diuretics reduce total body sodium through their natriuretic action and have also been shown to have vasodilatory effects. 33 Evidence from retrospective studies suggests increased CV mortality in diabetic patients receiving diuretics.34,35 These studies were not randomized, and significant baseline differences between patients receiving diuretics and the patients not receiving them may have existed. In addition, these studies were based on data collected in the 1970s when high-dose diuretic treatment was the norm. 2 High-dose diuretics have detrimental effects on serum glucose and HbA1c levels as well as on triglyceride and cholesterol. 19 However, low-dose diuretics are now more commonly prescribed and rarely cause clinically significant problems. Trials based on thiazide therapy, such as Systolic Hypertension in the Elderly Program (SHEP), have shown a substantial benefit in hypertensive patients with diabetes. 36 The Captopril Prevention Project (CAPPP) trial showed a lower incidence of stroke in the conventionally treated group (diuretics and beta blockers) than in the captopril-treated group and no difference in the primary end point of combined MI, stroke and death from CV causes. 37 The results of Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT), comparing chlorthalidone, lisinopril and amlodipine, favoured thiazide diuretics as first-line agents due to their efficacy, safety and low cost (including for the 36% of participants who had diabetes). No significant difference was seen between these three agents in the primary end point of fatal or non-fatal MI, although significantly fewer patients randomized to chlorthalidone developed heart failure. 38 Another arm of the study examining the use of doxazosin was terminated early due to an increase in combined CV disease (mainly heart failure) with respect to diuretic therapy. 39
In diabetic patients receiving thiazides, insulin sensitivity has been measured.33,40,41 Hydrochlorothiazide at a daily dose of 25 mg or bendrofluazide at 1.25 mg daily does not significantly decrease insulin sensitivity. However, bendrofluazide at a daily dose of 5 mg caused a significant reduction of in vivo insulin sensitivity. 33 Low-dose chlorthalidone in combination with atenolol was associated with low insulin sensitivity and increased triglyceride levels. 41 The clinical significance of these metabolic findings is unknown. In diuretic-based therapy, a low-dose thiazide diuretic has been shown to reduce the CV event rate by 34% compared with placebo; the absolute risk reduction was twice as great for diabetic patients versus non-diabetic patients. 15
Non-thiazide diuretics
A significant decrease in total body sodium and mild vasodilation is the anti-hypertensive mechanism of loop diuretics. 42 In the treatment of patients with diabetic nephropathy, furosemide in combination with β-adrenergic blockers was used as the mainstay anti-hypertensive regime in a study reported by Parving et al., 43 and there was a significant reduction in the rate of deterioration of the glomerular filtration rate (GFR) in patients with type 1 diabetes treated with an aggressive anti-hypertensive regimen. The major adverse effects of loop diuretics are hypokalaemia, hyponatraemia and volume depletion. 41 Their use is recommended for patients with decreased renal function (GFR < 60 mL/min).
Adrenergic blockers
Centrally acting agents
These drugs effectively lower BP by decreasing central sympathetic outflow. 41 However, studies on their effects on the progression or development of micro-vascular complications or CVD have not been carried out. Their major side effects are orthostatic hypotension, drowsiness, impotence and dry mouth, and minor side effects are depression and Coombs-positive anaemia (with α-methyldopa). 44 They should be used with caution in patients with CV autonomic neuropathy.
Beta blockers
Beta blockers are competitive inhibitors of the β-adrenergic receptors. Beta blockers have also been avoided due to a theoretical adverse effect on insulin sensitivity and lipid profiles, as well as a detrimental effect on hypoglycaemic awareness. Cardioselective and non-selective beta blockers differ in this regard, and fewer problems are seen with low-dose cardioselective drugs.19,45 Small effects on insulin sensitivity and the lipid profile are rarely relevant in the clinical management of hypertension, but beta blockers are contra-indicated in patients with frequent hypoglycaemia or hypoglycaemic unawareness.
In UKPDS, atenolol was at least as effective as captopril as a first-line agent, 46 but the drug treatment comparison was inadequately powered to provide a definite conclusion, that is, formal ‘equivalence’. No significant differences were seen between the two groups’ lipid profiles. Differences were seen in HbA1c in the first 4 years of follow-up but not in the second 4 years. In the atenolol groups, 81% of patients were receiving an additional oral hypoglycaemic agent after 8 years compared to 71% in the captopril groups. It is notable that the patients randomized to atenolol gained more weight over the follow-up period. Compliance was initially similar between the groups, but over time, fewer patients continued to take atenolol. There was no difference in rates of hypoglycaemia between the groups, and no comment was made on hypoglycaemic awareness. Non-selective β-blockers are associated with decreased counter-regulatory responses to hypoglycaemia, particularly in patients taking insulin. 47 However, it is unknown whether this effect is clinically important; the UKPDS study did not show an increased incidence of hypoglycaemic episodes in the group treated with β-blockers. Following this, several trials were carried out for use of metoprolol and carvedilol in diabetic patients. Carvedilol has more favourable metabolic effects in diabetic patients than traditional β-blockers.48,49 The Carvedilol Or Metoprolol European Trial (COMET) demonstrated that carvedilol at a target dose of 50 mg daily reduced mortality in patients with heart failure compared with metoprolol tartrate at a target dose of 100 mg daily in patients with chronic heart failure.50,51 The subsequent analysis of COMET revealed that treatment with carvedilol is associated with less development of new onset diabetes in patients with heart failure compared with treatment with metoprolol tartrate. 52 The possible mechanism behind this could be that insulin-stimulated endothelial function remained preserved during treatment with carvedilol and blunted during treatment with metoprolol. 53
α-Adrenergic blockers
α-Adrenergic blockers are inhibitors of the α-post-sympathetic adrenergic receptors. 54 α-Blockers have been recommended for the treatment of diabetic hypertension on the basis of their efficacy, lack of adverse effects on glucose or insulin metabolism and neutral or perhaps beneficial effect on the lipid profile. 55 The anti-hypertensive effects of these medications at the doses approved for clinical use are similar to other groups of agents. α-Adrenergic blockers have been associated with improved insulin sensitivity in patients with insulin resistance associated with essential hypertension. 56 A slight decrease in low-density lipoprotein (LDL) cholesterol has been reported with α-adrenergic blockers in small short-term clinical studies, all involving <25 patients per group. 57 The clinical significance of these findings is unclear. Initial doses of these agents, particularly prazosin, 54 have been associated with orthostatic hypotension; therefore, this agent should be used with caution in patients with diabetic autonomic neuropathy. The ALLHAT study had an arm comparing an α-blocker, doxazosin, with a β-blocker, a calcium channel blocker (CCB) and an angiotensin-converting enzyme (ACE) inhibitor versus a diuretic. 58 There are both advantages and disadvantages to the use of central sympatholytic anti-hypertensive agents (e.g. clonidine, guanabenz, methyldopa and guanfacine) in the diabetic patient. Advantages include their lipid-neutral and minimal-to-absent hyperglycaemic effects. However, centrally acting sympatholytic medications may worsen or unmask both orthostatic hypotension and sexual dysfunction in diabetic patients. 59
CCBs
CCBs inhibit calcium influx through membrane-bound voltage-dependent calcium channels, resulting in decreased intracellular calcium levels and vasodilation. 41 The use of CCBs in high-risk groups has been the subject of debate, as some retrospective cohort studies have shown adverse effects on cardiac disease. Initial concerns were raised by studies in non-diabetic populations using short-acting dihydropyridines, which suggested that they may increase the incidence of MI. The main concerns for patients with diabetes came from the Appropriate Blood Pressure Control in Diabetes (ABCD)18,60 trial and Fosinopril versus Amlodipine Cardiovascular Events Randomized Trial (FACET). 61 These were small, underpowered trials with non-CV primary end points. In contrast, large well-designed trials, which have included patients with diabetes, support the use and safety of calcium channel antagonists. ALLHAT showed that amlodipine was not significantly different from chlorthalidone in preventing MI. 38 Supporting evidence comes from the Hypertension Optimal Treatment (HOT) study, which used step-wise therapy based on felodipine. 11 The Systemic hypertension in Europe (SYST-EUR) study also used a regime based on the calcium channel antagonist nitrendipine. This study showed a reduction in stroke and CV events against placebo in older patients with isolated systolic hypertension. A further subanalysis was performed on the subgroup of patients with diabetes (492 of 4695). 16 However, in both HOT and SYST-EUR trials, most patients were also receiving a β-blocker or an ACE inhibitor in order to achieve the goals of therapy. Therefore, it is difficult to judge the effectiveness of monotherapy with these drugs in reducing CV end points. 2 Benefit was again seen in this group, which was at least as great as that shown in SHEP. 36 Swedish Trial in Old Patients (STOP) examined three groups of patients given conventional therapy (diuretic or beta blocker), ACE inhibitor or calcium channel antagonist. 62 It was originally reported that all three agents conferred equal benefit; however, in a post-trial diabetes subgroup analysis (719 of 6614 patients), there were more MIs in the calcium channel group (although there was no difference in mortality). 62 A recent meta-analysis has confirmed a trend for stroke outcomes to be better for CCBs, although in this analysis, they were inferior to other anti-hypertensives in terms of preventing MI. 63 In conclusion, long-acting CCBs appear safe in people with hypertension and diabetes.
ACE inhibitors
ACE inhibitors have been promoted as first-line agents in diabetes since they appear to have actions over and above BP-lowering alone. They have beneficial effects in heart failure and appear to be beneficial in left ventricular hypertrophy (LVH) and in non-diabetic renal disease. Additionally, ACE inhibitors are not thought to affect glucose or lipid levels adversely. Although there are data demonstrating the efficacy of ACE inhibitors in lowering BP, there are as yet few data showing a reduction in CV mortality. Most of the available data are from the Heart Outcomes Prevention Evaluation (HOPE) study. 64 This trial recruited 9541 patients aged over 55 years with a history of coronary artery disease or diabetes and one or more other CV risk factors. It examined ramipril against placebo with a composite primary end point of MI, stroke and death from CV causes. In those randomized to ramipril, the incidence of MI was reduced by 20%, stroke by 32% and death from CV causes by 26%. This was achieved with a mean BP reduction of 3/2 mmHg in a population that was mainly normotensive. Importantly, in this context, 3577 of the patients in the HOPE study had diabetes. This subgroup was deliberately recruited with the intention of having a cohort large enough to look at CV outcomes as well as the progression of diabetes. The results in the subgroup with diabetes were similar to those in the overall study. The benefits observed in association with active treatment in HOPE were calculated by the investigators to be around 3 times greater than those predicted from BP-related risk estimates (from the placebo group of HOPE and other studies). Therefore, they hypothesized that ACE inhibition confers benefits beyond BP-lowering. 65 However, a subsequent substudy, which measured 24-h ambulatory BP, suggested that BP-lowering was indeed the mechanism of end point reduction in patients randomized to ramipril. There were large differences in BP between patients taking placebo and those taking ramipril (especially at nighttime) compared to the small differences in office BP readings reported in the main study. Thus, BP-lowering may explain the benefits seen with ramipril.66,67 The UKPDS–Hypertension in Diabetic Study (UKPDS-HDS) showed similar beneficial effects of the ACE inhibitor captopril and the β-blocker atenolol on diabetes-related mortality and micro-vascular and CV complications in patients with type 2 diabetes.13,66 Similarly, the CAPPP trial compared captopril to conventional anti-hypertensive agents (diuretics and beta blockers) in 11,018 patients with hypertension of whom 572 also had diabetes. The results showed no significant difference in the primary end point of combined MI and stroke (whether fatal or not) and other CV deaths. 37 In the diabetic subgroup, fewer patients randomized to captopril reached the primary end point than those randomized to conventional therapy (relative risk: 0.59, p = 0.018). 68 Further information on the effects of ACE inhibition in stroke disease comes from the PROGRESS (perindopril protection against recurrent stroke) study which examined perindopril-based treatment in hypertensive and normotensive patients with a history of stroke disease. 69 A significant reduction in recurrent stroke was seen in patients given a combination of indapamide and perindopril, although interestingly not in those on perindopril alone. Benefits in terms of mortality and CV events were also seen in the treatment group. BP was 12/5 mmHg lower in the combination group and 5/3 mmHg lower in the perindopril group. This suggests that the effect seen may have been attributable to BP-lowering rather than a specific effect of the agent or class; however, it does provide hard outcome data for ACE inhibition in this context.
Angiotensin receptor blockers
Fewer side effects is the major benefit of angiotensin receptor blockers (ARBs). With the exception of the Losartan Intervention for Endpoint reduction in hypertension (LIFE) study, scant CV morbidity and mortality data are available. 70 This was a double-masked, randomized, parallel-group trial comparing losartan and atenolol in patients with hypertension and LVH, which showed a 25% reduction in stroke, but not in MI, with losartan. A difference in the rate of development of diabetes was also seen between the groups (four additional cases with atenolol per 1000 patient years). A pre-specified diabetes subgroup analysis was published at the same time. 71 A total of 1195 patients with diabetes (both types 1 and 2) were randomized to receive atenolol or losartan and followed up for a mean of 4.7 years. Additional therapy with hydrochlorothiazide was added to achieve BPs of 146/79 (losartan) and 148/79 (atenolol). At the end of the trial, more than 60% of participants were taking more than just the study medication. The primary end point was a composite of CV mortality, stroke and MI and occurred in 103 (18%) patients allocated to losartan and in 139 (23%) allocated to atenolol, giving an adjusted hazard ratio of 0.76, p = 0.031. Confidence intervals were wide, and MI and stroke as individual end points were not significantly reduced, although there were significant reductions in CV (losartan 6%, atenolol 10%) and total mortality (losartan 11%, atenolol 17%). In the absence of other morbidity and mortality data from the ARB class, it is difficult to draw definitive conclusions from this trial, but it seems that losartan has advantages over atenolol for some patients at least. In the Candesartan in Heart Failure: Assessment of Reduction in Mortality and Morbidity (CHARM) study, which involved patients who had symptomatic heart failure and had been hospitalized in the previous 6 months, candesartan, when added to existing therapy with any ACE inhibitor used at variable doses (with less than half the patients receiving full doses), was superior to placebo in reducing death or hospitalization for heart failure. 72 Another study on Valsartan in Acute Myocardial Infarction Trial (VALIANT) established the non-inferiority of valsartan, as compared with captopril, in patients with left ventricular (LV) dysfunction or heart failure after MI since the combination of a full dose of captopril plus valsartan did not significantly reduce the occurrence of the primary outcome. 73 Telmisartan was equivalent to ramipril in patients with vascular disease or high-risk diabetes and was associated with less angioedema. 74 Telmisartan was well tolerated in patients unable to tolerate ACE inhibitors and modestly reduced the risk of the composite outcome of CV death, MI or stroke. 75 A meta-analysis of randomized controlled trials indicates that telmisartan provides a superior BP control over ACE inhibitors (enalapril, ramipril and perindopril) and has fewer drug-related adverse events and better tolerability in hypertensive patients. 76
Combination therapy
Low-dose combination therapy may resolve some of the dilemmas in hypertensive patients with diabetes, although it is not without its problems. In UKPDS, after 9 years of follow-up, 29% of patients in the ‘tight BP control’ group needed three or more therapies to meet target BP. 13 In clinical practice, most hypertensive patients with diabetes will not have their BP controlled on one therapy alone, rendering the argument over the best single agent less relevant. There has been some examination of the most effective therapeutic combinations. Low-dose diuretics are noted to augment the anti-hypertensive effects of other major classes and therefore work well in combinations. 77 They may have a particular role in combination with drugs that block the renin–angiotensin system. CCBs and ACE inhibitors in combination may be beneficial as they have different mechanisms of decreasing BP and have been shown to be effective together. In a small study, dual blockade of the renin–angiotensin system using candesartan and lisinopril [the Candesartan and Lisinopril Microalbuminuria (CALM) study] found that the combination of both agents reduced BP and urinary albumin levels to a greater extent than either medication alone. 78 In general, combination therapy may help to improve compliance, as one drug may antagonize the adverse effects of another. 79 Fixed-dose combinations of many drugs are available and may be appropriate when the patient requires more than one drug, the dosages in the product are appropriate for the patient, and the costs are not greatly increased. A morbidity–mortality double-blind trial, ADVANCE (Action in Diabetes and Vascular disease: PreterAx and DiamicroN MR Controlled Evaluation) study in normotensive or hypertensive patients with type 2 diabetes, used a fixed-dose combination tablet containing perindopril and indapamide. Significant reductions in the relative risk of death from CVD, total coronary events and total renal events were observed. 80 Combination of an ACE inhibitor and an ARB was used in Randomized Evaluation of Strategies for Left Ventricular Dysfunction (RESOLVD) pilot study, which depicted no sustained aldosterone reduction. 81 In heart, the combination of valsartan and spironolactone has been shown to suppress cardiac remodelling, such as myocyte hypertrophy and perivascular fibrosis, in hypertensive rats. 82 In another study, candesartan treatment improves the early stage of LV remodelling in patients with essential hypertension, and the addition of spironolactone during candesartan treatment is clinically efficacious in reducing the LVH, which has been already developed. 83 Furthermore, Naruse et al. 84 have reported that endothelin-1 messenger RNA (mRNA) expression increases after a longer period of candesartan administration in spontaneously hypertensive stroke prone rats but was decreased by co-administration of spironolactone. Exploring further, the combination therapy for long-term studies may be beneficial for hypertensive diabetic patients.
Newer agents
Aliskiren is an orally active renin inhibitor, which became the first drug in its class to receive regulatory approval for the treatment of hypertension. Aliskiren inhibits the first rate-limiting step in the renin–angiotensin–aldosterone system (RAAS) cascade, the conversion of angiotensinogen to angiotensin I and thereby reducing synthesis of all subsequent components of the cascade. 85 Aliskiren Trial in Type 2 Diabetes Using Cardio-Renal Endpoints (ALTITUDE), an international, randomized, double-blind, placebo-controlled, parallel-group trial, was initiated to determine the effect of aliskiren on CV and renal morbidity and mortality compared with placebo when added to conventional treatment (including ACE inhibitor or ARB) in three categories of high-risk patients with type 2 diabetes. Initially, they aimed to randomize 8600 patients with a planned follow-up time of 48 months. 86 However, ALTITUDE trial was stopped prematurely in December 2011 on recommendation of the data monitoring committee after it found an increased occurrence of side effects, and continuation of the study was deemed ‘futile’. Patients in the aliskiren group experienced significantly increased serum potassium of ≥6 mmol/L and reported hypotension. 87 It was further reported that the addition of aliskiren to standard therapy with renin–angiotensin system blockade in patients with type 2 diabetes who are at high risk for CV and renal events is not supported by these data and may even be harmful. 88
Alagebrium (4,5-dimethylthiazolium) is a novel breaker of cross-links in advanced glycation end products (AGEs) and has been studied mainly for its chronic effects on AGEs. 89 A randomized, double-blind, parallel-group trial of assessment of safety and efficacy was initiated for alagebrium in 2007. 90 However, the study was terminated early due to financial constraints. 91 Thus, with new anti-hypertensives coming into the market, there seems still a long way to go for use of the same in diabetes.
Treatment plan
The choice of anti-hypertensives to be used in diabetic patients should not only aim at controlling hypertension but also in preventing/delaying the development of complications. In such patients, initially, the BP should be monitored for 1 month to confirm the presence of hypertension. The confirmed hypertensive diabetic patients should be given the treatment as per the algorithm (Figure 3). Patients having BP between 130/80 mmHg and 140/90 mmHg should be first started with lifestyle modification and monitored regularly. For patients with BP ≥ 140/90 mmHg, the first-line therapy consists of ACE inhibitor or ARBs. ACE inhibitor should be started for type 1 diabetics and ARBs for type 2 diabetics; however, ACE inhibitor should be the choice of agent for patients with micro-albuminuria for both type 1 and type 2 diabetic patients. For patients with micro-albuminuria who are unable to tolerate ACE inhibitors or ARBs, CCBs should be considered. If the BP control is not obtained with the first-line treatment, the doses can be increased, and if BP is not controlled even with increased doses, second-line therapy should be initiated with diuretic, β-blocker or CCB, depending on compelling indication present. Despite this, if BP is not under control, other agents can be added or a specialist should be consulted. Although the algorithm present gives an overview of the anti-hypertensive to be given for diabetic patients, the treatment decisions should be individualized.
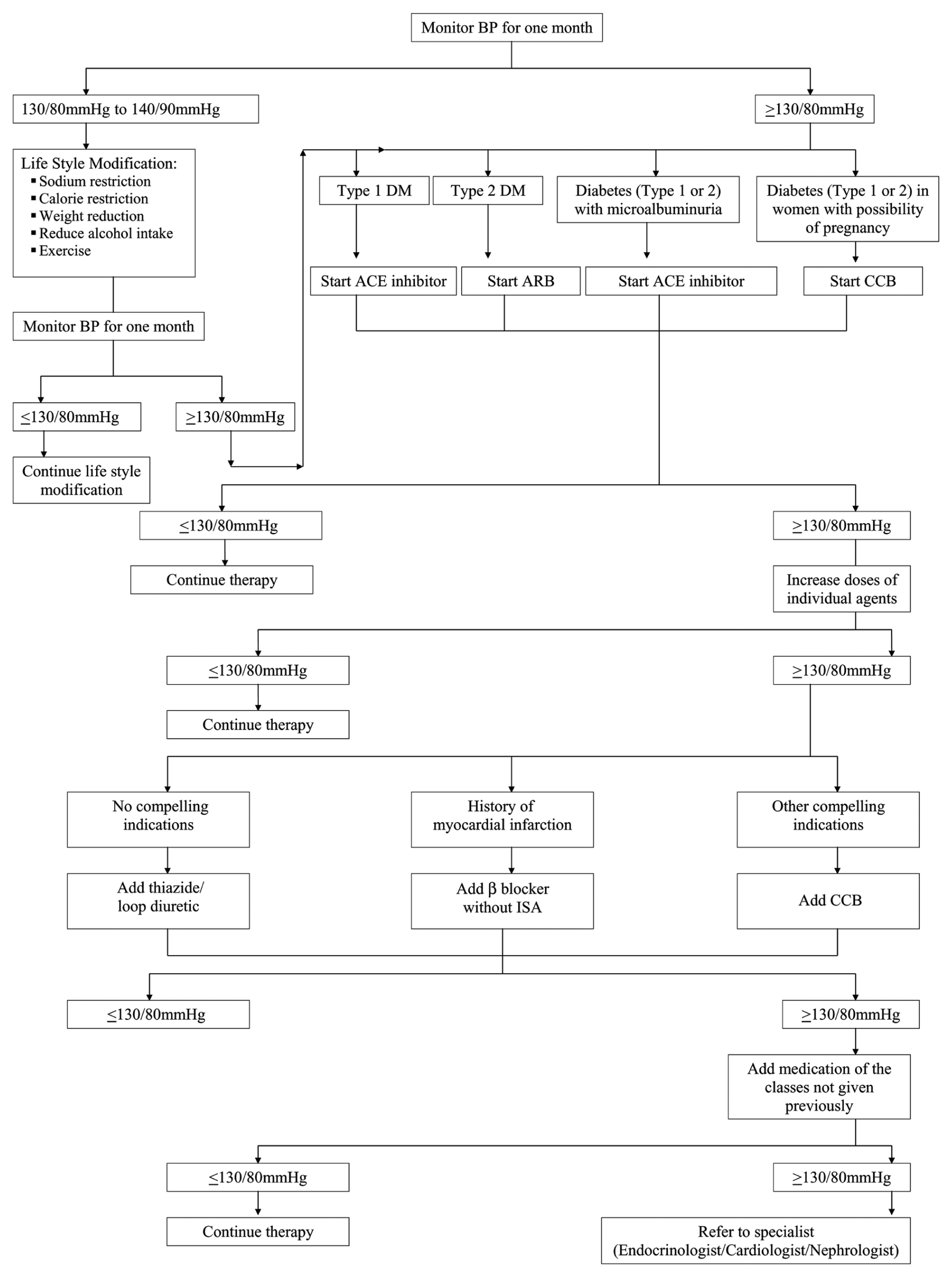
Treatment algorithm for anti-hypertensives in diabetics.
Conclusions
Hypertension patients with diabetes are at considerably greater risk for diabetes-specific complications and an aggressive approach for the diagnosis and treatment is required to substantially reduce the incidence of both macro-vascular and micro-vascular complications. The choice of anti-hypertensives to be used in diabetic patients should not only aim at controlling hypertension but also in preventing/delaying the development of complications. Most of the patients do not respond to single drug, and hence, multiple drugs are required. When more than one anti-hypertensive is given, patient should be closely monitored for major adverse effects. Furthermore, there is a dire need for conducting more long-term clinical trials to substantiate the current literature.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.