
Abstract
Construction workers (CW) are at increased risk for a range of chronic diseases. We screened 983 CW for diabetes and cardiometabolic risk. The age range was 18–64 years, with mean age of 36.3 years. Self-reported questionnaires, Finnish diabetes risk score and fasting blood tests were collected at the workplace. The unadjusted prevalence of pre-diabetes and type 2 diabetes mellitus were 3.6% and 1.2%, respectively; 21% of CW had the metabolic syndrome (MetS). The majority were either overweight (48.3%) or obese (21.8%). In a regression model, age remained the strongest predictor of fasting glucose (p < 0.001). Pre-diabetes and diabetes mellitus were significantly associated with presence of the MetS [odds ratio (OR) 5.6; 95% confidence interval (CI): 2.8–11.5, p < 0.001 and OR 5.5; 95% CI: 1.6–18.7, p = 0.006, respectively]. Subjects engaged in greater physical activity outside of work had lower body mass index (26.9 vs. 28.8 kg/m2, p = 0.03), waist circumference (95.8 vs. 98.1 cm, p = 0.03) and fasting serum triglycerides (1.1 vs. 1.4 mmol/L, p = 0.03) compared to those who were sedentary. Despite their youth and a physically demanding occupation, CW are at risk of cardiometabolic diseases. This risk increases with age and the MetS. Screening tools may be useful to identify those who are at risk.
Introduction
The prevalence of type 2 diabetes (T2DM) has been increasing dramatically as a result of obesity, ageing and urbanisation. 1,2 T2DM and pre-diabetes (PreDM) are currently being diagnosed at an earlier age throughout the world. 3,4 Lack of physical activity and unhealthy diet have been implicated as factors contributing to the development of obesity, diabetes and cardiovascular disease (CVD). 5,6 Thus, young and middle-aged people in their active working years are at increased risk of diabetes and its related complications, with major implications both for work productivity and for overall public health and public finances.
Recent studies have examined habitual physical activity and its relationship to the risk of diabetes mellitus (DM). Physical inactivity is a recognised risk factor for insulin resistance, 7,8 an important precursor to T2DM. On the other hand, CVD mortality among patients with T2DM is significantly reduced by moderate or high levels of physical activity and physical fitness. 9 –11 In addition, the risk of coronary heart disease and cardiovascular mortality is lower in those with greater leisure-time physical activity. 12,13 Observational studies have shown that mortality is also lower in individuals who are more physically active at work. 14 Body mass index (BMI), blood pressure and circulating concentrations of inflammatory markers are all known to be favourably affected by exercise and physical activity. 15,16
Studies in construction workers (CW) from several countries have reported a high prevalence of CVD risk factors. 17 –19 In Ireland, up to now, cardiovascular or diabetes risk has not been formally prospectively studied in the construction industry. However, Brenner et al. 20 reported in 2000 that CVD constituted nearly one-third of conditions leading to early retirement on the grounds of disability among Irish CW. Other studies in the industry have also confirmed the detrimental effect of conditions such as obesity, hypertension and hypercholesterolaemia on the frequency of illness-related absences. 21,22
The aim of this study was to investigate the prevalence of undiagnosed T2DM, PreDM and the metabolic syndrome (MetS), as well as associated risk factors and predictors among Irish CW.
Research design and methods
CW employed at 34 different construction sites mostly in the greater Dublin area were invited by the Construction Workers Health Trust (CWHT) to participate in a health screening programme. The screening programme started in August 2006 and ended in July 2008. Ethical approval was obtained from the Joint Research and Ethics Committee, Adelaide, and Meath Hospital, Dublin. A total of 983 male construction workers volunteered to participate in this study. All participants provided written informed consent prior to any study procedures. A team of four practice nurses from CWHT underwent formal instruction and specific training in the procedures for this study.
Demographic data, anthropometric measurements and blood samples were obtained by study nurses at the health care centres provided at construction worksites. Standardised lifestyle and health questionnaires and the Finnish diabetes risk score (FINDRISC) were collected for each participant (see Appendix 1). Self-reported alcohol intake, smoking and physical activity at work and outside of work hours were estimated from the questionnaires. Although questions related to physical activity were self-reported and have not yet been validated, its use was only for the purpose of ranking physical activity at work and leisure-time activity. FINDRISC is a diabetes risk score that has been utilised in several European population cohorts as a screening tool to identify those at risk of developing T2DM. 23 –25 The risk scores vary from 0 to 20, and various studies have assessed the predictive value of different score thresholds. 23,26
Body weight and height were measured in participants wearing light clothing without shoes. BMI was calculated as weight in kilograms divided by the square of height in metres. Waist circumference was measured at the level of the umbilicus. Hip circumference was measured at the level of the anterior superior iliac crest. Blood pressure was measured in the sitting position after a 10-min rest period using appropriately sized sphygmomanometer cuffs (Omron M7). Following an overnight fast, fasting venous blood samples and capillary glucose measurements (for on-site analysis) were obtained simultaneously. Venous blood samples were stored in fluoride oxalate tubes and placed in ice-filled containers. These were then sent by courier drivers from the collection site to the clinical research unit within 1–2 h of collection for immediate separation and analysis.
The MetS was defined according to the International Diabetes Federation criteria. 27 Data and clinical information pertaining to the FINDRISC, lifestyle and health questionnaires were entered into an encrypted database by the study clinicians. The results of fasting plasma glucose, lipid profile and blood pressure measurements were mailed to each study subject. Information regarding lifestyle advice or follow-up with their primary care physician was included in each letter by the study clinicians. Subjects with impaired fasting glucose [IFG, defined from the American Diabetes Association (ADA) criteria of fasting glucose value ≥5.6] were contacted by the study clinicians and returned on a separate morning, fasting, to undergo a 2-h oral glucose tolerance test (OGTT). Based on the results, subjects were classified as having impaired glucose tolerance (IGT) if the 2-h postprandial glucose (2-h PG) value was between 7.8 and 11.0 mmol/L or DM if the fasting plasma glucose value was ≥7.0 mmol/L or 2-h PG value ≥11.1 mmol/L following the OGTT.
Laboratory analyses
Plasma glucose was measured using a glucose oxidase method (Bio Merieux Kit/Hitachi Modular). Plasma total cholesterol and triglycerides were measured using enzymatic methods (Human Liquicolor Kits/Hitachi Modular). Plasma high-density lipoprotein (HDL) cholesterol and low-density lipoprotein (LDL) cholesterol were measured directly with enzymatic methods (Randox Direct Kits/Hitachi Modular). Capillary glucose was measured on-site using HemoCue® (Quest Diagnostics Inc.) glucose analyser.
Statistical analysis
The demographic characteristics of study participants are presented as mean ± standard deviation (SD) or as numbers and percentages, where appropriate. Independent-sample t-tests were used to compare means for normally distributed variables (i.e. weight, BMI, waist circumference, waist:hip ratio, systolic blood pressure, diastolic blood pressure, total cholesterol and LDL cholesterol) and Mann–Whitney tests for non-normally distributed variables. Spearman’s rank order test was used to assess correlation. Multiple logistic regression analysis was used to identify predictors and to calculate odds ratios (ORs) and confidence intervals (CIs). Linear regression analysis was used to calculate Beta coefficients and identify predictors for continuous variables. All statistical analyses were performed using SPSS (SAS, v13). Statistical significance was set at p < 0.05.
Results
A total of 983 participants between the ages of 17–64 were screened. The majority were Irish nationals (89.2%). Table 1 outlines the baseline characteristics of the whole cohort and of the two age categories (less than 40 years and more than 40 years old).
Baseline characteristics of the whole CW cohort and of the two age categories (those less than 40 years and more than 40 years old).
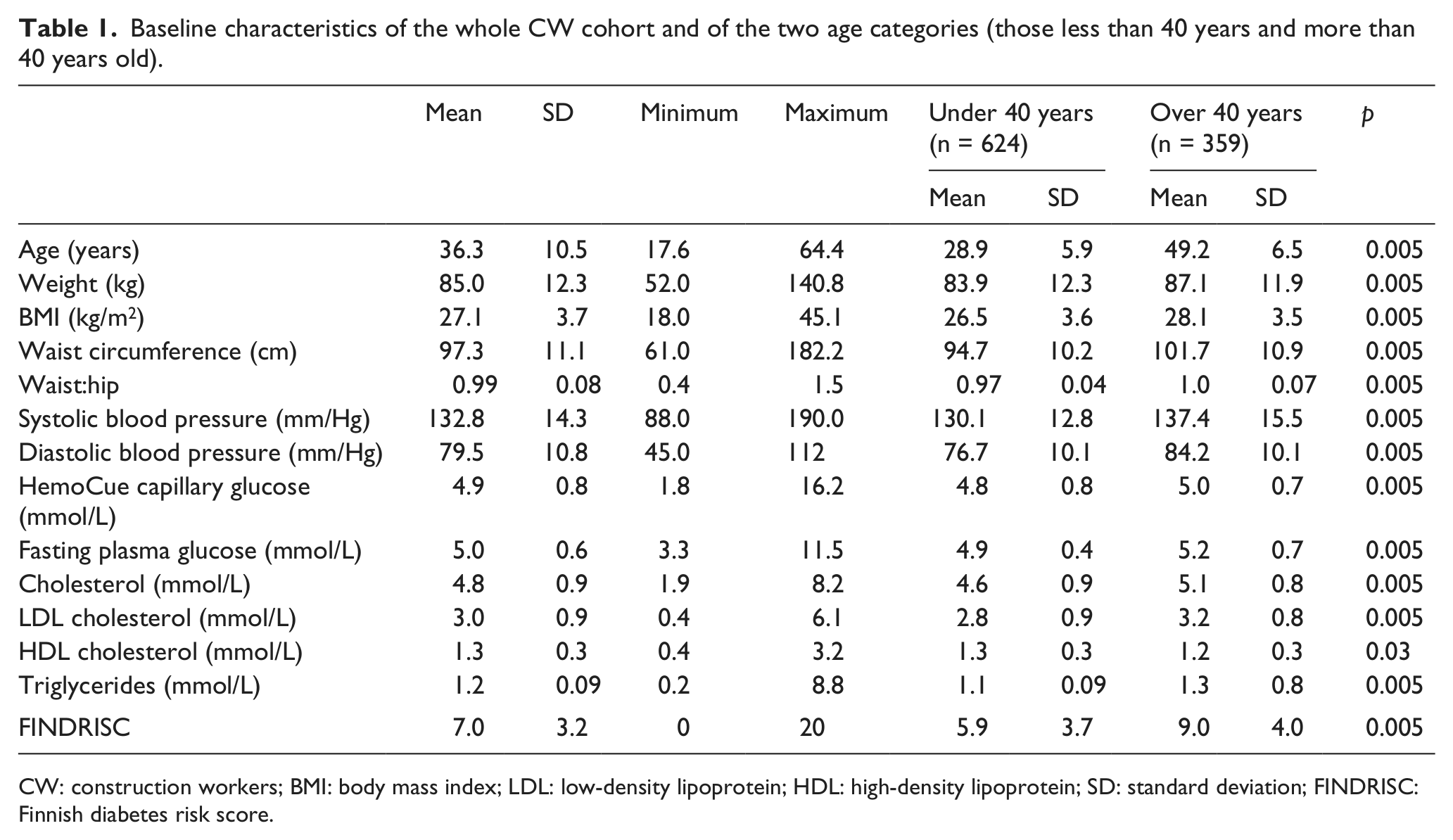
CW: construction workers; BMI: body mass index; LDL: low-density lipoprotein; HDL: high-density lipoprotein; SD: standard deviation; FINDRISC: Finnish diabetes risk score.
Prevalence of diabetes, PreDM and the MetS
The unadjusted prevalence of previously undiagnosed T2DM in the whole cohort was 1.2%, while 3.6% were diagnosed with PreDM (60% IFG and 40% IGT). Both PreDM and T2DM were more prevalent in those above 40 years of age (Figure 1). MetS was found in 21% of the cohort.
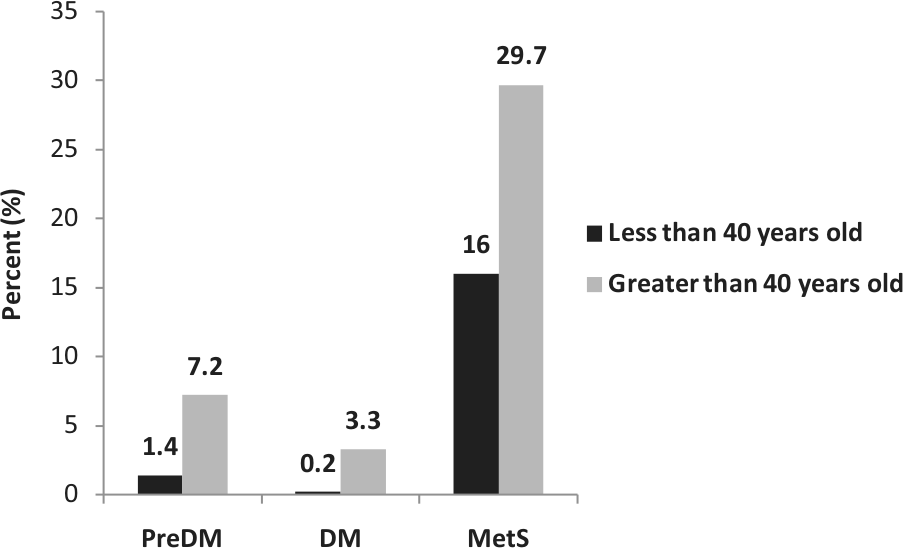
Prevalence of PreDM, DM and the MetS.
Risk factors and predictors
The majority of CW screened were either overweight (48.3%) or obese (21.8%). Forty-two per cent had blood pressure measurements in the hypertensive range (≥140/90 mm/Hg), and of these, only 3.6% were on treatment for hypertension. In all, 60% had elevated waist circumference, 41.3% were hypercholesterolaemic (>5.0 mmol/L) and 46.6% had elevated LDL cholesterol (>3.0 mmol/L) (see Figure 2).
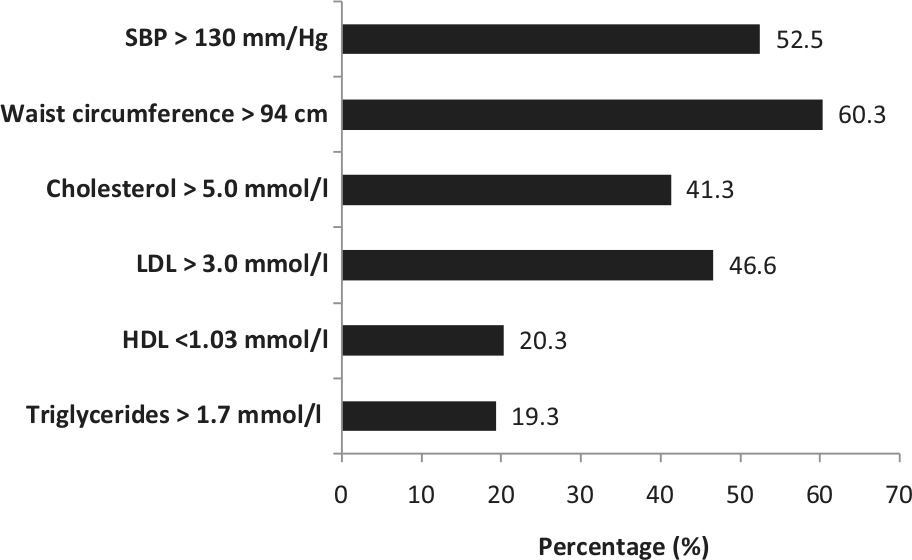
Prevalence of components of the MetS according to the International Diabetes Federation Criteria.
Capillary fasting glucose measurements by HemoCue correlated moderately with fasting venous blood glucose measurements (r = 0.51, p = 0.005, see Figure 3). Multivariate regression analysis revealed that FINDRISCs (OR 1.2; 95% CI: 1.1–1.4, p = 0.031) and HemoCue capillary glucose levels greater than 7 mmol/L (OR 3.4; 95% CI: 1.9–5.9, p = 0.005) at screening significantly increased the risk of both PreDM and DM. CW with both PreDM and DM were older than those with normal glucose tolerance (47.5 ± 9.2 vs. 35.7 ± 11.2 years, p < 0.001). PreDM and DM were also significantly associated with the presence of the MetS (OR 5.6; 95% CI: 2.8–11.5, p < 0.001 and OR 5.5; 95% CI: 1.6–18.7, p = 0.006, respectively).
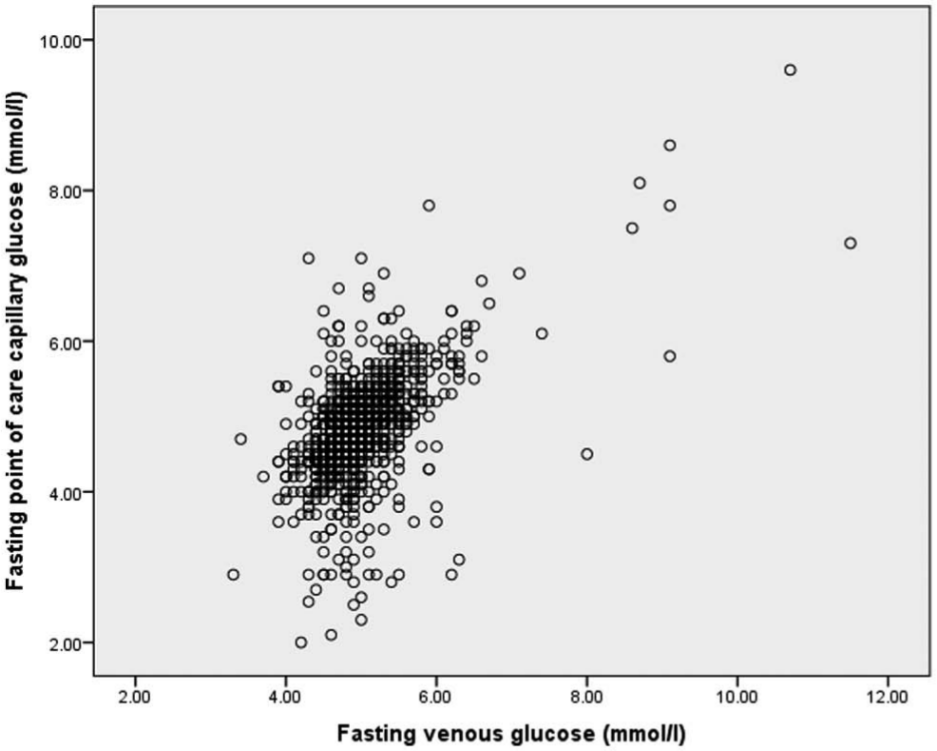
Scatterplot graph illustrating the correlation between fasting capillary glucose and venous glucose levels (r = 0.51, p = 0.005).
Significant correlation was found between fasting plasma glucose and age (r = 0.35, p < 0.001). Significant relationships were also found between fasting plasma glucose levels and components of the MetS, such as systolic blood pressure (r = 0.18, p < 0.001), waist circumference (r = 0.31, p < 0.001), cholesterol (r = 0.2, p < 0.001), LDL (r = 0.18, p < 0.001), HDL (r = −0.1, p = 0.012) and triglycerides (r = 0.23, p < 0.001). Entering age and components of the MetS into a regression model revealed that age remained the strongest predictor of fasting plasma glucose (Beta coefficient = 0.25, p < 0.001), followed by waist circumference (Beta coefficient = 0.13, p < 0.001) and systolic blood pressure (Beta coefficient = 0.064, p = 0.05).
Physical activity questionnaires
Details on physical activity at work and outside of the workplace were analysed from the lifestyle questionnaire (see Appendix 1). For example, to the question ‘How much hard physical work is required on your job?’, participants who answered ‘A great deal’ were deemed to be physically active at work and those who answered ‘None’ were deemed to be sedentary at work. No significant differences were found in the clinical or biochemical measurements between these two groups. Self-reported physical activity outside of the workplace was determined from the question ‘How often do you exercise or play sports for at least 20 minutes?’ Compared with those (about 25% of subjects) who reported to be physically active outside the workplace (more than three to four times per week), those who reported to be less physically active (not more than twice a week, 30% of subjects) had a higher BMI (p = 0.03), waist circumference (p = 0.03), plasma triglyceride concentration (p = 0.03) and higher scores on the FINDRISC (p = 0.008) (see Table 2).
Leisure-time activity – based on analysis of lifestyle questionnaire; ‘How often do you exercise or play sports for at least 20 minutes?’.
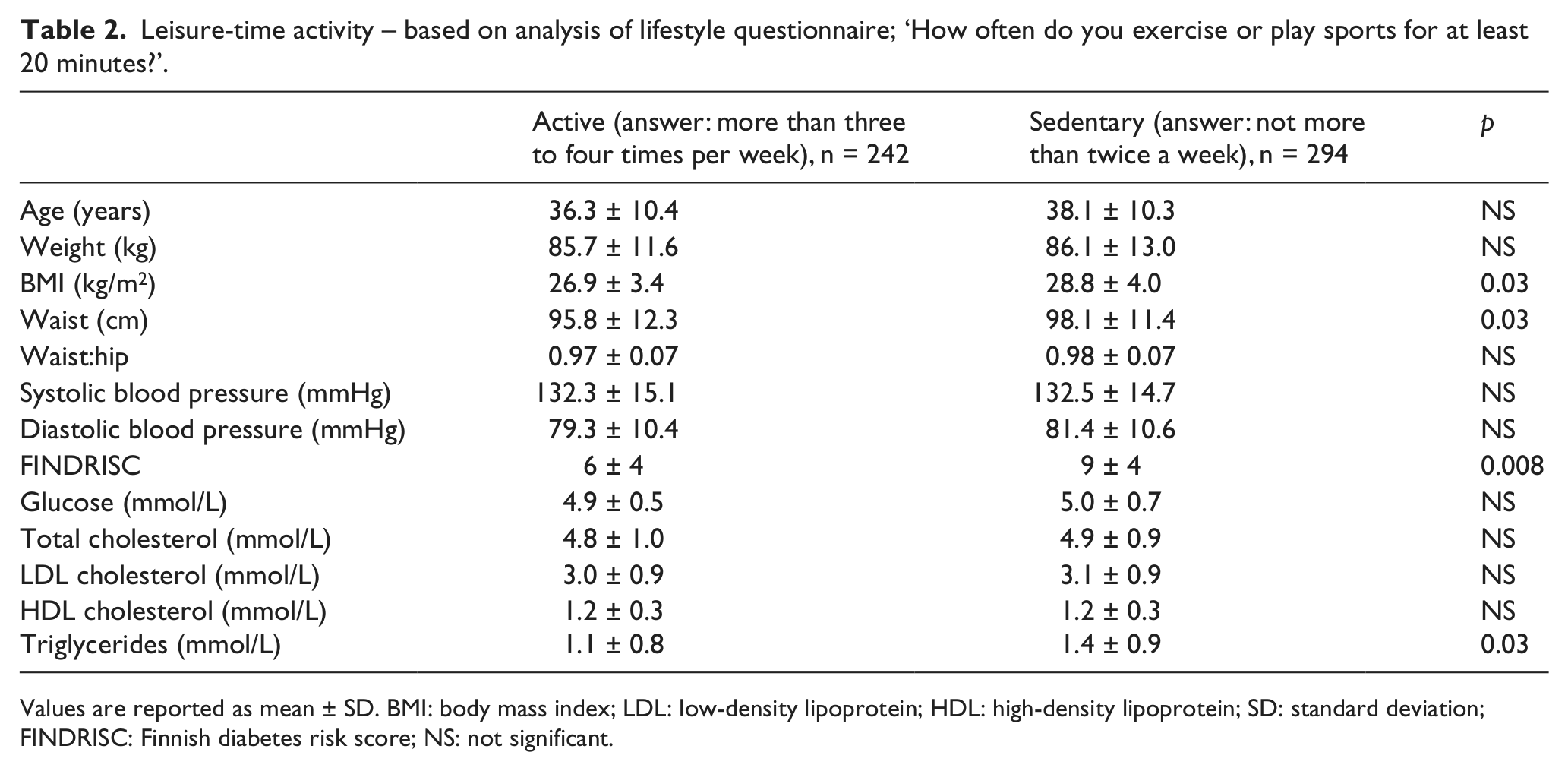
Values are reported as mean ± SD. BMI: body mass index; LDL: low-density lipoprotein; HDL: high-density lipoprotein; SD: standard deviation; FINDRISC: Finnish diabetes risk score; NS: not significant.
Discussion
To date, there have been no reports of the prevalence of diabetes or cardiometabolic disease risk factors within the construction industry in Ireland. In 2011, the construction sector accounted for 10.4% of total employment in men in Ireland, compared to the European Union (EU) average of 8%. 28,29 The CW cohort provides an important perspective on the health and associated cardiovascular co-morbidities in the working group population of Ireland.
Overall, 983 CW participated in this pilot programme to screen for DM and cardiometabolic risk factors. The age-adjusted prevalence of T2DM is similar to the estimated national rate of T2DM for males in Ireland. 30,31 Because it was not possible to conduct 2-h OGTT at construction sites on a large scale, only fasting venous blood samples were obtained. Participants were invited to have a 2-h OGTT only if their fasting plasma glucose values were greater than 5.6 mmol/L. The DECODE study reported that nearly a third of subjects with DM diagnosed using the 2-h OGTT would have been missed if fasting glucose alone was used for diagnosis. 32 Therefore, the likelihood that a number of subjects with an elevated 2-h post OGTT glucose but normal fasting plasma glucose may have been missed could not be outruled, thereby potentially underestimating the true prevalence of T2DM in this cohort.
We explored the clinical feasibility of utilising a point-of-care (POC) device (HemoCue) in our screening programme at construction sites. The accuracy and reliability of POC testing are important considerations in this context of on-site screening. The accuracy of HemoCue in comparison to plasma glucose as reference has been reported in both healthy subjects and patients with diverse pathologies. 33,34 However, only a moderate correlation between HemoCue and plasma glucose was found in our study. Factors that may have influenced this POC glucose analysis include device-related (i.e. system performance), environmental (i.e. on-site temperature and humidity) or operator-related factors (i.e. quality control performance and sample volume). 35 –37 To minimise the latter, practise nurses in our study were trained and competent in the use of the HemoCue. Although the benefit of POC testing is the immediate analytical information it provides, our study indicates that confirmation by laboratory glucose analysis on venous plasma should remain the standard on which clinical decisions are made.
In this study, higher FINDRISCs were significantly associated with PreDM and DM. A 5-year prospective study by Lindström and Tuomilehto 23 reported that a score value of ≥9 had the optimal sensitivity and specificity to identify individuals at high risk for drug-treated diabetes in a Finnish cohort. Risk score values have also been validated in other European countries. 24,26 A follow-up longitudinal study of the CW cohort is currently needed to determine the appropriate threshold FINDRISC for future risk prediction. This will further validate the FINDRISC as a non-invasive screening tool for asymptomatic individuals at high risk for T2DM in Ireland.
The prevalence of obesity in our cohort was similar to that of the background population (22%, in the age group between 30 and 44 years old), as reported in the 2007 Irish Survey of Lifestyle, Attitudes and Nutrition (SLAN). 38 This is despite the perception that CW have a physically demanding occupation. Obesity is increasingly recognised as being associated with poor health and occupational practices. 39 This may be related to long hours of sedentary and high stressed work, compounded by poor health choices such as increased alcohol intake, smoking and lack of healthy dietary options in the workplace. Reducing employee obesity through active intervention programmes at work has been shown to be effective at improving cardiovascular risk factors. 40 These intervention programmes help create awareness among employees regarding healthy diet, the risks associated with cigarette smoking and alcohol consumption and the need for regular physical activity to prevent obesity and CVD.
The CW cohort was found to have a high prevalence of the adverse components of the MetS such as hypertension, dyslipidaemia and elevated waist circumference. Physical activity is known to be protective against the MetS and CVD risk factors. 41,42 In this study, when self-reported physical activity at work was assessed, no significant differences were found in the cardiometabolic risk of those who reported to be physically active at work and those who were sedentary. Interestingly, however, differences in cardiometabolic risk were observed when groups reporting different degrees of leisure-time physical activity were compared. A potential explanation may be that either the physical activity performed during working hours by the CW cohort did not meet the level needed for cardiovascular fitness, which is important for improving cardiometabolic status, or participants over- or underestimated physical activity at their workplace due to the inherently physical nature of their work. A follow-up study is needed to objectively assess for cardiovascular fitness and its effect on cardiometabolic parameters in this cohort.
Conclusion
This distinctive young cohort of the Irish workforce presents a pattern of high risk for cardiometabolic disease. The perception that CW have a physically demanding occupation, hence negating the need for additional leisure-time physical activity, was not borne out by our study, given similar levels of obesity and age-adjusted diabetes prevalence to Irish males in general. Further studies are needed to identify the underlying causes of the adverse risk profile in these construction workers and to raise public health awareness in the cohort and their families. The FINDRISC may serve as a useful tool to screen for those who are at increased risk of developing DM, and a longitudinal study is needed to establish the relevant threshold FINDRISC for this population. POC testing with HemoCue in a screening programme offers some practical advantages but requires a confirmatory laboratory test before a diagnostic or clinical decision can be made. The findings from this study support the need for lifestyle and health awareness programmes at work for employees within the Irish construction industry.
Footnotes
Appendix 1. Self-reported lifestyle questionnaire
Acknowledgements
The authors thank all the subjects who participated, and the team of practice nurses who conducted the on-site screening.
Conflict of interest
The authors declare that they have no conflicts of interest.
Funding
This project was supported by grants from the Diabetes Education and Research Fund (at the Metabolic Research Unit, St James’s Hospital and Trinity College Dublin) and the Construction Workers Health Trust, Ireland.