
Abstract
People with disturbed glucose metabolism are at an increased risk for cardiovascular disease. This risk starts before diabetes, according to present definitions, is established. Early detection of impaired glucose tolerance and target-driven multifactorial management incorporating all risk factors in a broad sense may effectively improve the prognosis for these persons. Management includes early detection of glucose perturbations and preventing or delaying future diabetes among people with impaired glucose tolerance. In people with established diabetes, hypertension, hyperlipidaemia and hyperglycaemia are all important factors to monitor and, if these are above the recommended levels, to treat, first hand with lifestyle-oriented recommendations, although usually supported by pharmacological interventions. Since impaired glucose tolerance and type 2 diabetes mellitus are rapidly increasing in the population, glucose perturbations as the cause of cardiovascular disease manifestations will become more common. Development of macrovascular complications substantially impacts care costs, and proper management of these individuals will therefore not only decrease personal suffering but also clearly impact health care expenditures.
Keywords
Diabetes and myocardial infarction – a serious combination
That diabetes and myocardial infarction represent a serious, in principle deadly, combination was reported on by Bradley and Bryfolge 1956, 1 but not paid much attention to until the 1980s when Rytter et al., 2 Molstad and Nustad 3 and Malmberg and Rydén 4 reported that the combination was common and associated with a very high mortality. The latter authors studied patients admitted to a coronary care unit during 1 year and detected that 24% of the patients had a diagnosis diabetes associated with in-hospital mortality of about 25% and 1-year mortality as high as 53%, while the corresponding proportions for patients without diabetes were 16% and 28%, respectively. In an early attempt to see whether different types of treatment influenced the outcome of these patients, Malmberg et al. made a retrospective analysis of the Gothenburg Metoprolol Trial incorporating 1395 patients, of whom 9% had diabetes. Looking at mortality after 3 months, the pattern of a substantially higher mortality in patients with diabetes compared with those without persisted (12% vs. 8%). A surprising finding was that the beta-blocker, metoprolol, significantly reduced mortality in patients with diabetes to 7.5%, while the impact on those without diabetes was insignificant. 5 This finding was subsequently verified by Kjekshus et al. 6 who examined a large multicentre cohort of 2024 patients, of whom 340 had diabetes. The 1-year mortality for hospital survivors was 17% for those with compared to 10% for those without diabetes, a highly significant finding. Patients with diabetes who were discharged with beta-blocker treatment had a 1-year mortality of 10 compared with 23% for those without beta-blockers. In patients without diabetes, the corresponding mortality was 7% and 13%, respectively. These two reports clearly indicated that the seriously adverse prognosis for patients with diabetes and myocardial infarction could be improved and encouraged further studies of the subject.
An obvious question is, of course, whether it still is of interest to review management of such patients. Unfortunately, the answer is a definite yes. Over the years, there has been successive improvement in the prognosis for patients with acute myocardial infarction – both for those with and without diabetes. The gap to the disadvantage of patients with diabetes is, however, still prevailing. As documented by the Swedish Coronary Care Unit Registry, incorporating data on all hospital admitted Swedish patients below the age of 80 with acute myocardial infarction, 1-year mortality among patients without diabetes in 2007 was about 7%, which is about 50% lower than in those with diabetes (Figure 1), a difference that is about the same in 2010. 7
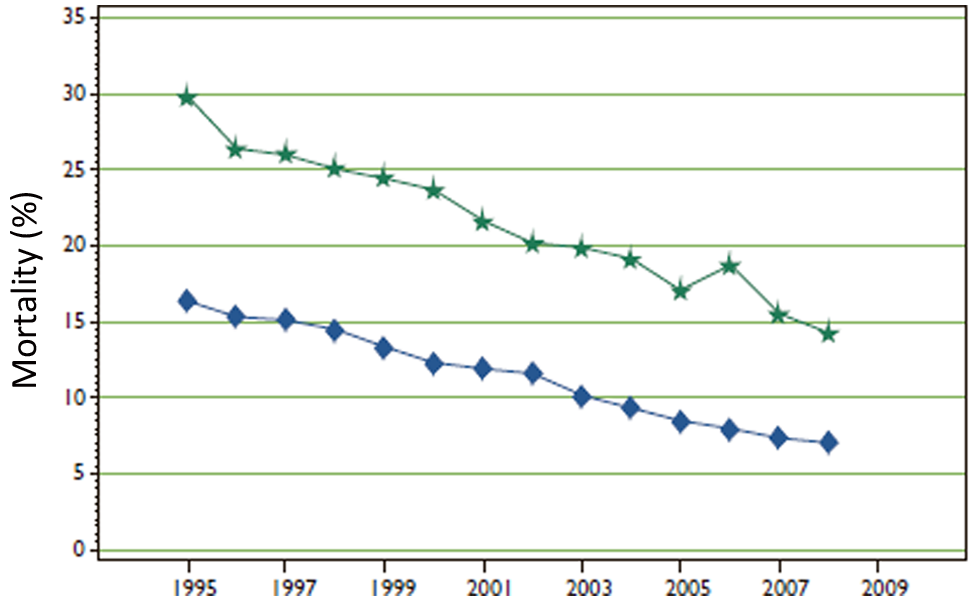
Time trends in one-year mortality by diabetic state among patients with myocardial infarction below the age of 80 years in the Swedish Coronary Care Registry. 4
Looking at a general population, people with diabetes have a higher death rate at a younger age that those without diabetes. The reason is an at least two times higher risk for cardiovascular disease. Among the first epidemiological reports that demonstrated a substantial, two- to four-fold, increased risk of coronary artery disease in patients with diabetes was the Framingham study, with the highest increment of risk associated with diabetes observed in people below the age of 45 years and in women. 8 In a more recent population-based survey from North Carolina, the cause of death for patients with diabetes was due to cardiovascular disease in almost 50% of the cases assessed, with diabetes-related mortality accounting for an additional 15%. 9
Considering the continued poor prognosis in people with the combination of diabetes and myocardial infarction, and the impact of diabetes on the risk for macrovascular complications, the present prediction of a rapid increase in the number of people with diabetes is particularly threatening. The International Diabetes Federation has predicted that the global number of people with diabetes will increase by 54% from 285 million people aged 20–79 years in 2010 to 438 million in 2030. Looking more specifically at the European situation, the number of people with diabetes was estimated to 55.4 in 2010 with a predicted increase to 66.5 million in 2030. In addition, the present number of people with impaired glucose tolerance has been estimated to increase from 66 to 72.2 million, 10 strongly underscoring the great importance of early detection and management of patients with glucose perturbations. The importance of early initiation of proper management of people with diabetes soon after diabetes is diagnosed is underscored in a study by Niskanen et al., 11 who followed a group of patients with newly detected type 2 diabetes and compared them with population-based controls free from diabetes over a period of 15 years. 8 Both total and cardiovascular mortality was substantially higher in the diabetes cohort, with an odds ratio for total mortality of 5.0 among males and 5.2 in females, and with the corresponding odds ratio for cardiovascular mortality of 6.2 and 11.2, respectively. When the patients and controls were investigated after 5, 10 and 15 years, it was apparent that the total and cardiovascular mortality following 5 years was not dramatically higher among patients with diabetes but it increased rapidly after 10 years, and in particular after 15 years. At the latter time, total mortality among males with diabetes was about 40% compared with about 13% among those without diabetes, and with similar proportions and numbers among females. The conclusion is that to have a possibility to counteract the increased mortality, in particular the high cardiovascular mortality, patients have to be treated as soon as the diagnosis is established and the opinion that there may be “mild cases of diabetes” is certainly not true. The position that diabetes should be recognised and treated early gets even stronger support from the 10-year follow-up study of the UKPDS. 12
Glucose perturbations – common in cardiovascular disease
A relation between glucose perturbations and myocardial infarction has been suspected for decades, with increasing appreciation for this association more recently. As reviewed by Opie and Stubbs in 1976, 13 glucosuria and high blood glucose are prevalent in patients with acute myocardial infarction. In their review, they speculated that the probable reason for the observed high glucose was an increased release of glucose due to adrenergic stress during the acute phase of a myocardial infarction, causing temporarily disturbed carbohydrate metabolism with hyperglycaemia related to the severity of the infarction. Subsequent investigations have, however, not verified this as the only reason. Another early observation indicated a continuous relationship between increasing levels of blood glucose and progressive cardiovascular risk starting already at glucose levels considered normal according to presently recommended diagnostic criteria. 14 This assumption got strong support from a recent meta-analysis of 102 studies comprising a dataset of 698,782 individuals with almost 11 years of median follow-up (8.49 million person years at risk), and with 52,765 fatal or non-fatal outcomes. 15 The analyses revealed that patients with a known history of diabetes at baseline had an adjusted hazard ratio of 2.00 (95% CI 1.83–2.19) for non-fatal and fatal coronary heart disease; 2.27 (1.95–2.65) for non-fatal and fatal ischemic stroke; and 1.73 (1.51–1.98) for the aggregate of other vascular deaths. The hazard ratios for coronary heart disease were higher in women than in men, higher for subjects aged 40–59 years compared with those above 70 years, higher in those with the lowest tertile vs. highest tertile of systolic blood pressure and higher for fatal versus non-fatal events. Moreover, there was a relation between fasting glucose and vascular risk already at the level of 5.6 mmol/L. This relation remained even when added to the information derived from several conventional risk factors. Thus, increasing blood glucose values seem to in particularly hit people who by other reasons are at a lower risk.
The relation between glucose abnormalities (impaired glucose tolerance and type 2 diabetes) and acute coronary syndromes (acute myocardial infarction and unstable angina) has attracted interest for decades. Early studies had some limitations which made them less reliable when looking at the true relation between hyperglycemia and acute coronary events. These studies were performed on selected populations with limited numbers of patients investigated with either intravenous or oral glucose tolerance tests (OGTT). The tests, not repeated over time, were performed at a time when diagnostic criteria for diabetes and impaired glucose tolerance were still not defined. With the objective to further explore this relation, the Glucose and Myocardial Infarction (GAMI) study was performed in 181 patients with acute myocardial infarction but without any previously known glucose perturbations. 16 They were all subjected to an OGTT before hospital discharge, i.e. about five days following onset of symptoms. The test revealed that only 33% of this patient population had a completely normal glucose tolerance, while 35% had impaired glucose tolerance and 31% previously undetected type 2 diabetes. These results were subsequently confirmed in the Euro Heart and China Heart Surveys,17,18 recruiting patients both with stable and unstable coronary artery disease. Both studies confirmed that a majority of patients without previously diagnosed glucose perturbations indeed had abnormal glucose metabolism split on newly detected diabetes and impaired glucose tolerance in approximately similar proportions as those revealed by the GAMI trial. The Euro Heart Survey on Diabetes and the Heart recruited 4961 patients with coronary artery disease, at 110 centres in 25 European countries among whom 31% of had known diabetes, 12% newly detected diabetes, 25% impaired glucose tolerance and 3% impaired fasting glucose, leaving only a minority of 29% with normal glucose regulation. 17 A similar pattern has subsequently been shown in patients with cerebro- and peripheral vascular disease. 19 Similar to the GAMI study, the latter investigation compared outcomes in patients with coronary artery disease with healthy age- and sex-matched persons from the population, among whom about 65% had a normal glucose regulation, 24% impaired glucose tolerance and 11% diabetes. This clearly illustrates that diabetes and prediabetes are very common among people with cardiovascular disease, and that an important relation exists between these two conditions. Observations from the Euro Heart Survey on Diabetes and the Heart furthermore demonstrated that a substantial proportion of patients with diabetes and impaired glucose tolerance would have remained undetected without an OGTT. 20 The importance of detecting glucose perturbation is strongly underscored by the fact that patients with normal glucose tolerance have a considerably better outcome during follow-up than those with abnormal glucose metabolism.21,22
To summarise present knowledge, it may be concluded that diabetes and prediabetes are very common among patients with cardiovascular disease; that an OGTT is needed when screening patients with cardiovascular disease for glucose perturbations; and that screening for glucose perturbations in patients with coronary artery disease provides information of importance for patient management. Although acknowledged in present management guidelines for patients with diabetes and cardiovascular disease, 23 and despite an increasing awareness of the importance of glycaemia, there has been a reluctance to diagnose prediabetic conditions in the medical community and the implementation of guideline recommendations is far from being accomplished.
An emerging problem are the recent recommendations by the American Diabetes Association and the World Heart Organisation to use HbA1c as a diagnostic criterion for diabetes.24,25 This may be useful when screening a general population, but in patients at a high risk of glucose perturbations and considering the increased risk of a cardiovascular morbidity and mortality already at a modest increase in plasma glucose, screening by the use of HbA1c, even if it is supplemented by a fasting glucose, is too insensitive. Hage et al. 26 screened 174 patients with acute coronary syndromes, of whom 27 had type 2 diabetes according to OGTT, including only 2 who would have been diagnosed by HbA1c. In this study, fasting glucose failed to detect 63% of patients with type 2 diabetes and HbA1c failed to detect 93%. Similar findings have been reported in patients with acute coronary syndromes selected for further investigation due to elevated admission glucose, 27 and in patients referred for coronary angiography. 28
A changing phenotype in acute coronary care
A population survey of 50-year old men in Gothenburg, Sweden, comparing risk factors prevalent in1963 with those in 2003 reveal interesting changes over time. The proportions of smokers decreased from 56 to 22%, and mean serum cholesterol declined from 6.4 to 5.5 mmol/L, both changes in a favourable direction. However, regular physical activity declined from 32% in 1963 to 24% in 2003, mean body mass index increased from 24.8 to 26.4 kg/m2, mean waist circumference increased from 87 to 95 cm, and the prevalence of diabetes increased from 3.6 to 6.6 % over the study period. 29 These changes indicate that the population in Gothenburg has moved towards a higher prevalence of people with characteristics of the metabolic syndrome.
Bartnik et al. 30 compared patients with myocardial infarction in the absence of known diabetes with age- and sex-matched healthy controls from the population. As can be seen in Figure 2, triglycerides, fasting and post-load glucose and proinsulin levels were considerably higher among the patients compared with controls. HOMA-index, as an expression for insulin resistance, did not differ significantly but was somewhat elevated in both groups. Combining this information with the high prevalence of glucose perturbations in patients with coronary artery disease, one may speculate that there has been a secular trend in the risk factor profile in patients admitted to coronary care units with a change from lean, stressed chain-smoking, chief executives with ST-elevation myocardial infarction towards a higher prevalence of overweight people with the metabolic syndrome, non ST-elevation infarctions, and previously undetected disturbed glucose metabolism. This assumption gains support from a recent report from the United States on population trends in the incidence and outcomes of acute myocardial infarction by Yeh, et al. 31 demonstrating that during the period 1999–2008 there has been an overall decrease in the incidence of myocardial infarction, particularly due to a lower number of ST-elevation infarctions, while non ST-elevation myocardial infarction to some extent has increased. Moreover, the proportion of patients with diabetes increased significantly from 27% in 1999 to 32% in 2008, dyslipidemia increased from 46 to 80% and hypertension from 45 to 76%. Accordingly, modern cardiologists do not only need to know how to handle the effects of coronary atherosclerosis and thrombosis, but also how to diagnose and manage a multiplicity of risk factors–not the least of which are those related to glucometabolic disturbances. Patients have to be managed with insight on the rapidly increasing cardiovascular risk of a combination of risk factors, something that certainly is common among people with glucose perturbations. 32 Attention should also be paid to the fact that although the cardiovascular risk increases with elevated blood pressure or LDL-cholesterol both in patients with and without diabetes, the actual risk at any specified level of these risk factors is many times higher among people with than in those without diabetes. 33
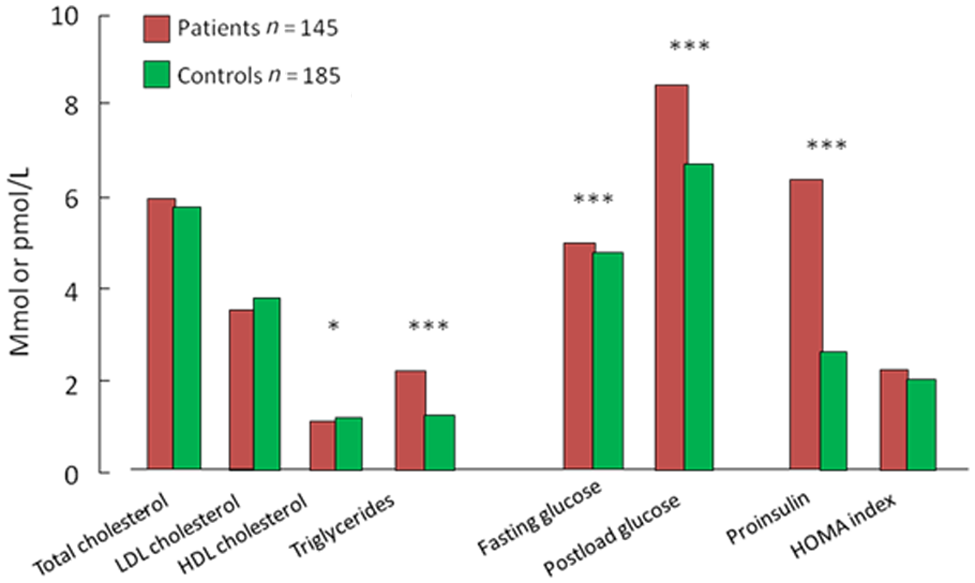
Metabolic variables in the GAMI trial comparing patients with myocardial infarction without known glucose perturbations and age and gender matched healthy controls from the population.
On the importance of multifactorial management
Multifactorial management of patients with coronary artery disease and glucose perturbations includes a number of important elements:
risk factor analysis including exploration of lifestyle-oriented habits, smoking, hypertension and dyslipidemia;
a search for microvascular complications (eyes, kidneys) and autonomic dysfunction;
a look for co-morbidities such as heart failure and arrhythmias;
exercise testing, stress echocardiography or myocardial scintigraphy to diagnose inducible ischemia.
A number of trials convincingly demonstrate that lifestyle-oriented programs based on a modest weight reduction and a moderately heavy physical activity 3 hours/week may effectively prevent or retard the progress from impaired glucose tolerance to overt type 2 diabetes in overweight (BMI 28–30kg/m2) people.34–38 The studies are summarised in Table 1, which reveals that the number of patients needed to treat for preventing or delaying one case of type 2 diabetes is fairly low.
Lifestyle-based studies aiming at the prevention of type 2 diabetes in people with impaired glucose tolerance. 23
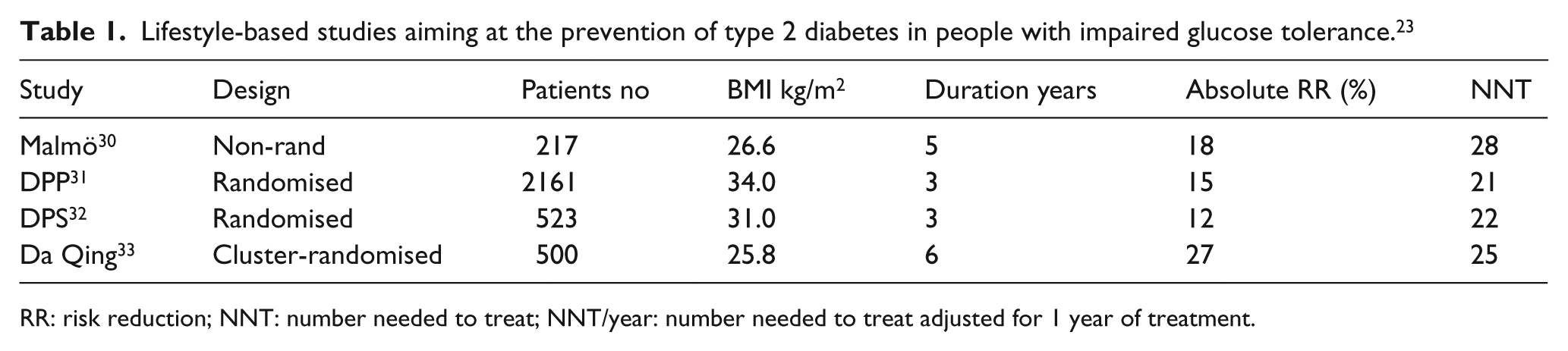
RR: risk reduction; NNT: number needed to treat; NNT/year: number needed to treat adjusted for 1 year of treatment.
Lifestyle modification was compared with metformin in the US Diabetes Prevention Program, 36 in which participants randomised to lifestyle intervention had a goal to reduce body weight by approximately 7% and to exert moderately heavy physical activity ≥ 150 minutes per week. Simple lifestyle advice turned out to be considerably more efficient than metformin treatment. Thus, 7 patients had to participate in the lifestyle counselling program during 3 years to delay or prevent 1 case of type 2 diabetes, which compares favourably with 14 among metformin treated persons. What has been lacking until recently is evidence of the efficacy of such programs in not only preventing type 2 diabetes, but also vascular complications. The first study to indicate that this may be the case was a long-term follow-up of the Malmö Feasibility Study, revealing that all-cause mortality among men in the intervention group was lower than among men who did not participate in a lifestyle program (6.5 vs. 14.0/1000 person years; p = 0.009). This study was, however, not randomised. 39 More recently, a 20-year follow-up of the Chinese Da Qing study disclosed a 17% reduction in cardiovascular mortality among people in the lifestyle group compared with those randomised as controls, which although not statistically significant can be seen as a trend towards benefit. The adjusted incidence of severe retinopathy was 47% lower in the intervention group than the control group (HR 0.53; 95% CI 0.29–0.99; p = 0.048). This was considered to relate to the reduced incidence of diabetes.40,41 Further details regarding long-term benefits from lifestyle intervention may be derived from an excellent review by Tuomilehto et al. 42
A multifactorial management strategy for people with coronary artery disease and glucose perturbations should be target-driven as strongly endorsed by the joint management guidelines issued by the European Society of Cardiology and the European Association of Diabetes, 23 and the presently recommended targets are presented in Table 2.
Treatment targets for patients with diabetes and coronary artery disease according to the European guidelines for managing patients with coronary artery disease and diabetes. 19
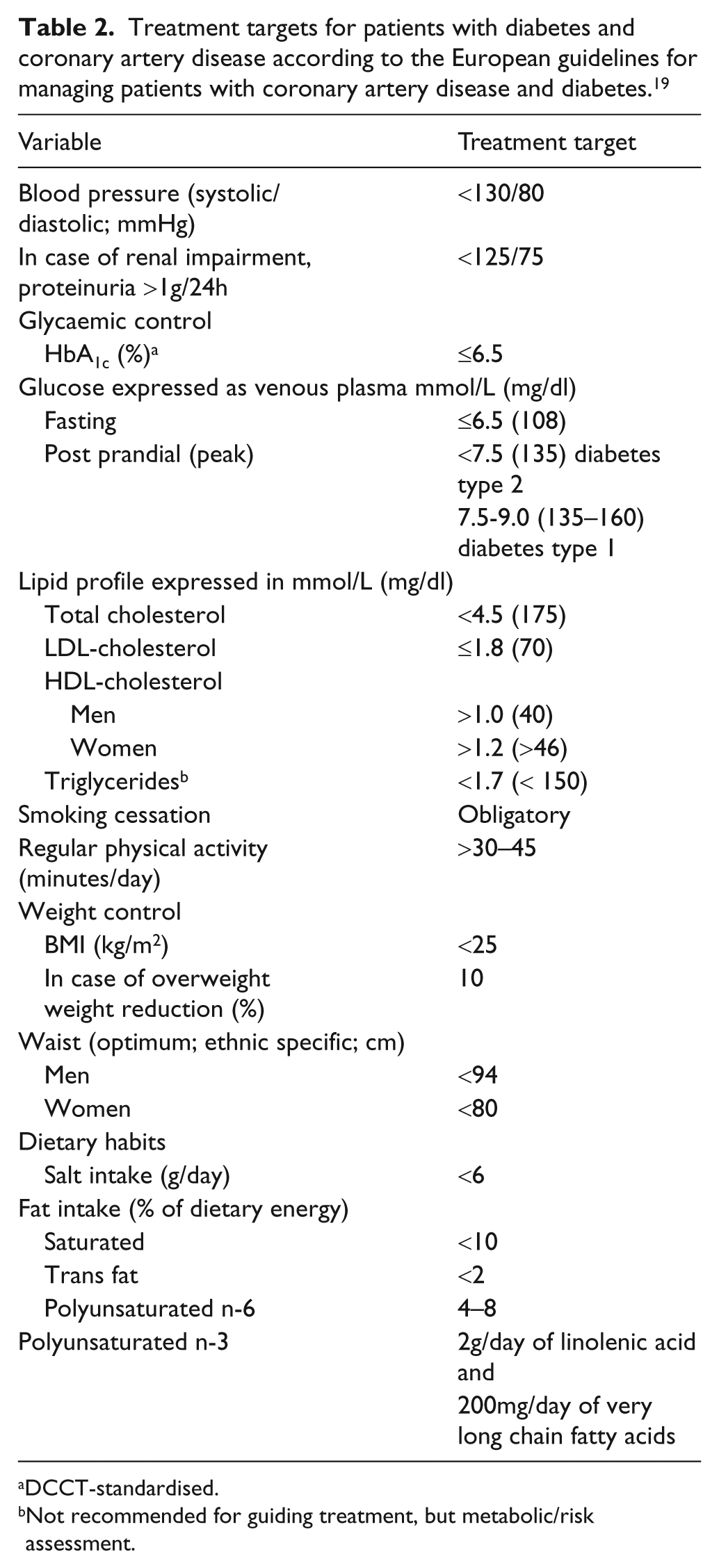
DCCT-standardised.
Not recommended for guiding treatment, but metabolic/risk assessment.
The value of a multifactorial intervention has been clearly demonstrated by the Steno 2 trial that randomised 160 patients with diabetes and microalbuminuria to intensive target-driven therapy or conventional management. 43 Notably all patients in the intensive group received blockers of the renin-angiotensin system and low-dose aspirin, and the overall management was considerably improved among this group despite that treatment targets were not always reached. The outcome after 8 years of follow-up was a 50% reduction in micro- and macrovascular events, and after a pre-planned follow-up 13 years after randomisation, intensively managed patients had a 20% absolute reduction in mortality (HR 0.54, 95% CI 0.32–0.89; p = 0.02). The absolute risk reduction in cardiovascular events was 29%, and a substantial reduction was seen in diabetic nephropathy and progression of retinopathy.44,45 The multifactorial intensive treatment was not only lifesaving but also cost-efficient. 46
Turning to patients with the combination of established coronary artery disease and type 2 diabetes, the Euro Heart Survey on Diabetes and the Heart reported on patients receiving a full package of evidence-based pharmacological therapy (a combination of aspirin, beta-blockade, renin-angiotensin-aldosterone inhibitors, and statins) vs. those who did not receive such a combination. The evidence-based management resulted in a significantly lower total mortality (3.5 vs. 7.7%) and fewer cardiovascular events (11.6 vs. 14.7%) compared with the outcome among patients who did not receive such a full combination of drugs. 47 The same survey revealed that a high proportion of the patients did not reach the present guideline targets (Table 2). Thus, 61% had a total cholesterol and 93% a LDL-cholesterol above target, while 56% had a higher than recommended blood pressure and 32% were above the HbA1c target (Anselmino and Rydén: data on file). Accordingly, there is a great potential for improvement in treatment, but also great hope, for people with coronary artery disease and glucose perturbations just by following guideline recommendations in a better way than presently practiced.
Concluding remarks
Since impaired glucose tolerance and type 2 diabetes mellitus are rapidly increasing in the population, glucose perturbations as the cause of cardiovascular disease manifestations will become more common. Development of macrovascular complications has a substantial impact of care costs. Proper management of these individuals will therefore not only decrease personal suffering but also have a clear impact on health care expenditures.
Footnotes
Funding
This article was supported by a grant from the Swedish Heart- and Lung Foundation.
Conflict of interest
None declared.