
Abstract
The GLP-1 receptor agonist exenatide has been approved for adjunctive treatment of type 2 diabetes. Continuous GLP-1 infusion improves endothelial function in vivo; no evidence about a beneficial effect of exenatide on vascular function has been published. The aim of our observational study was to evaluate whether exenatide would improve brachial artery function evaluated by the flow mediated dilation (FMD) technique, compared with glimepiride, in subjects with type 2 diabetes. FMD time course was assessed by ultrasound, after 5 min forearm ischaemia, at baseline and after 16-week treatment. At the end of the study FMD was significantly higher in subjects who assumed exenatide compared with glimepiride (9.1 ± 3.6 vs. 5.6 ± 1.0, p = 0.01). Even if limited by the small number of studied subjects, who were not matched in the two treatment groups, this research study represents the first FMD evidence suggesting that chronic administration of exenatide improves arterial dilation.
Introduction
The GLP-1 mimetic exenatide, recently approved for the treatment of type 2 diabetes, reduces glycated haemoglobin (HbA1c) and fasting and post-prandial glycaemia.1–3 High-affinity GLP-1 receptors are present in different tissues, and their activation induces pancreatic and extra- pancreatic effects. 4 In addition to lowering blood glucose, native GLP-1 infusion can improve cardiac and endothelial function.5–7 In particular, Nystrom et al. have described a significant increase in flow mediated dilation (FMD) of brachial artery in subjects with type 2 diabetes. FMD is a non-invasive, ultrasound-based technique that provides a bioassay for in vivo endothelial function. 8 Endothelial dysfunction is considered a reliable marker of vascular complications in subjects with type 1 and type 2 diabetes and predictive of future cardiovascular events.9,10
The common FMD technique involves the measurement of brachial artery at baseline and 50–60 s after ischaemia. However, time to peak varies between individuals and is influenced by age, and even training status. 11 In a previous study, we identified for the first time temporally distinct FMD patterns in subjects with type 2 diabetes, in which measures during the standard clinical measurement time point of ~50 s post cuff release were compared with measures at 2 min post release. These comparisons revealed that some subjects have maximal (peak) FMD at 50 s (Early FMD), others have peak FMD at 2 min (Late FMD) and others have no dilation at all (Absent FMD). 12 This finding suggests that FMD should be measured at different times in order to detect a delayed dilation after ischaemia.
So far no data are available about possible beneficial effects of new hypoglycaemic agents like exenatide on FMD. The aim of our study was to investigate whether exenatide would improve brachial artery peak dilation, measured by FMD technique, compared with glimepiride therapy after 16-week treatment. We have evaluated endothelial function extending the time of observation up to 3 min, in order to verify among subjects included in the study whether a delayed response existed either at baseline or after treatment.
In addition to FMD we have also measured the shear rate as a measure of the mechanical force stimulus inducing dilation after ischaemia.
Methods
This is an observational study including 20 subjects with type 2 diabetes consecutively assigned to receive glimepiride or exenatide, following the current guidelines, as add-on therapy to maximal tolerated metformin dosage, in order to improve glycaemic control. The researcher who assigned the treatment was different from the researcher who performed vascular tests. Local Ethical Committee approved the research and all participants gave their consent. Subjects were enrolled among those regularly attending the outpatient clinic. Inclusion criteria were: stable treatment (previous six months) with maximal tolerated metformin dosage, HbA1c > 7.5% and < 10%; age 45–65 years; no contraindication to glimepiride or exenatide treatment, post-menopause for women. Exclusion criteria were any antidiabetic treatment different from metformin, heart failure, severe kidney or liver disease. Subjects were defined as hypertensive if they were assuming anti-hypertensive drugs or if blood pressure levels were >140/90 mmHg. Blood pressure was measured twice, after 10 minutes resting, and the mean value calculated. Subjects were defined as hyperlipidaemic if they were assuming lipid lowering agents or if they had total cholesterol and/or triglycerides higher than 200 mg/dl. The study protocol included three visits (baseline, additional and follow-up visit). At baseline visit venous blood was collected for fasting glucose, glycated haemoglobin (A1c) and lipid (total cholesterol, high density lipoprotein (HDL)-cholesterol, triglycerides) determination. Subjects were asked to fast for 12 hours before blood withdrawal, to abstain from caffeine and tobacco and to not take morning therapy. They were also invited to abstain from intensive physical activity the day before. During the baseline visit the ultrasound study of endothelial function was performed. Afterwards subjects were assigned to receive exenatide or glimepiride. Exenatide starting therapy was 5µg b.i.d., while glimepiride was 4 mg o.d. A one-month visit (additional visit) was scheduled for all subjects to verify the compliance to drug prescription and the occurrence of possible side effects. During this visit exenatide dosage was escalated up to 10 µg b.i.d., while glimepiride dose could be reduced to 2 mg o.d., if subjects reported hypoglycaemic events. Metformin administration remained constant during the observation time in both groups, as well as administration of anti-hypertensive and lipid lowering agents. The third visit (follow-up visit) was scheduled after 16 weeks. During this visit blood was collected for fasting glucose, lipid and A1c determination. Ultrasound study was repeated as well.
Blood lipids and fasting glucose were measured with commercially available kits. HbA1c was determined by high-performance liquid chromatographic method, aligned with DCCT.
The ultrasound study was performed by a single expert sonographer (CI), blinded to treatment assignment. An echo Doppler ATL 5000 HDI Instrument (Advanced Technology Laboratories, Inc.) equipped with a 5–12 MHz high-resolution linear probe and with simultaneous ECG recording was used. Endothelial function was evaluated in the brachial artery visualised in a longitudinal section, on the anterior side of the biceps muscle of the non-dominant arm. To obtain a clear 2D image, the probe was kept perpendicular to the artery ~10 cm above the elbow. After that, the skin was marked and the probe clamped in a probe holder in order to maintain the same position throughout the study. Internal brachial artery diameter (ID), defined as the distance between intima–lumen interface of the near wall and lumen–intima interface of the far wall, and baseline velocity were recorded. A pneumatic cuff, previously placed around the forearm, was then inflated up to 250 mmHg for 5 min to create peripheral ischaemia. Blood velocity was again recorded 1 min before cuff deflation and for 40 s after deflation. 2D ultrasound imaging for diameter measurement was recorded at 50 s, 2 min and 3 min after cuff deflation at the T wave of the cardiac cycle, in order to evaluate the FMD time course. These time points were selected according to our recent study, demonstrating that subjects with type 2 diabetes may exhibit maximal dilation after either 50 s or 2 min. 12
Systolic peak and mean velocity, at baseline and post-ischaemic test, were automatically detected by the instrument, as the mean of two cardiac cycles. Mean velocity represents the time-average peak velocity that is the mean velocity of the highest velocities during the cardiac cycle. Brachial artery ID was measured off-line using dedicated software (Autodesk® Design Review). The software allows the careful measurement of distances between selected points. In detail, images were recorded during the study procedure and transferred onto the computer screen using an external device. ID was measured, for each selected image, in the central centimetre using three different callipers. ID values, shown in the tables, represent the mean of the three callipers. Diameter was measured at baseline and at 50 s, 2 min and 3 min (FMD time course). FMD was expressed as percentage change from baseline and calculated using the following formula: [(post-deflation (50 s, 2, 3 min) ID - baseline ID/baseline ID) ×100]. Peak FMD was defined as the maximal dilation detected among three different measurements.
To evaluate the total amount of the hyperaemic stimulus, the shear rate area under the curve (SR AUC) was calculated. Shear rate, that is the velocity gradient developing in the artery, has been calculated using the following formula: mean blood flow velocity/vessel diameter. Due to the variability in SR after ischaemia among subjects, we also calculated FMD to shear rate ratio (FMD:SR AUC) in order to normalise the FMD for the stimulus.13,14 To measure the reproducibility and precision of the method we have studied 15 subjects twice (data not published). Within method reproducibility, expressed as the percentage of the coefficient of variation [(SD of the paired differences/the overall mean)√2] × 100, was 5.4% for brachial artery diameter, 7.4% for FMD and 24.8% for mean blood velocity. The technical error of measurement, which is the square of root of the measurement error variance, was calculated using the formula: [√(ΣD2/2N)], where D is the difference between measurements and N is the number of individuals. The result was 2.4 for brachial artery diameter, 0.55 for FMD and 0.18 for mean blood velocity.
The statistical analysis was performed using SPSS 11.0 (SPSS, Inc., Chicago, Illinois). Variables, except triglycerides, were normally distributed. Triglycerides were log transformed before applying parametric test. The t test for unpaired data was applied in order to evaluate the differences between exenatide and glimepiride groups. The t test for paired data was applied to evaluate the differences between baseline and follow-up visit in each group. To evaluate the independent contribution of clinical, haemodynamic variables and therapy to peak FMD measured after 16-week treatment, multiple linear regression analysis was performed. Peak-FMD was included as the dependent variable, while the independent variables were age, sex, disease duration, hypertension (or blood pressure), hyperlipidaemia (or blood lipids), treatment, BMI, fasting plasma glucose, HbA1c and SR AUC measured at follow-up visit.
Results
The prevalence of subjects with hyperlipidaemia and hypertension was similar in both groups (hyperlipidaemia: exenatide 50% vs. glimepiride 30%; hypertension: exenatide 50% vs. glimepiride 60%), as well as the prevalence of subjects who were assuming statins (80% in both groups) and renin–angiotensin-system blockers (70% in exenatide group vs. 60% in glimepiride group). No subject had a history of a previous acute cardiovascular event, and no one was a current smoker. Glimepiride was well tolerated throughout the study. Two subjects in the exenatide group experienced transient nausea after starting therapy. At the additional visit exenatide was increased up to 10 µg b.i.d. and glimepiride dosage was confirmed (4 mg). As shown in Table 1, clinical and biochemical variables were not significantly different at baseline between the treatment groups. After 16-week treatment fasting glucose and A1c decreased in both groups, though significantly only in the exenatide group. Body mass index (BMI) and body weight increased in glimepiride group compared with exenatide.
Clinical and biochemical variables at baseline and follow-up in subjects divided according to treatment.
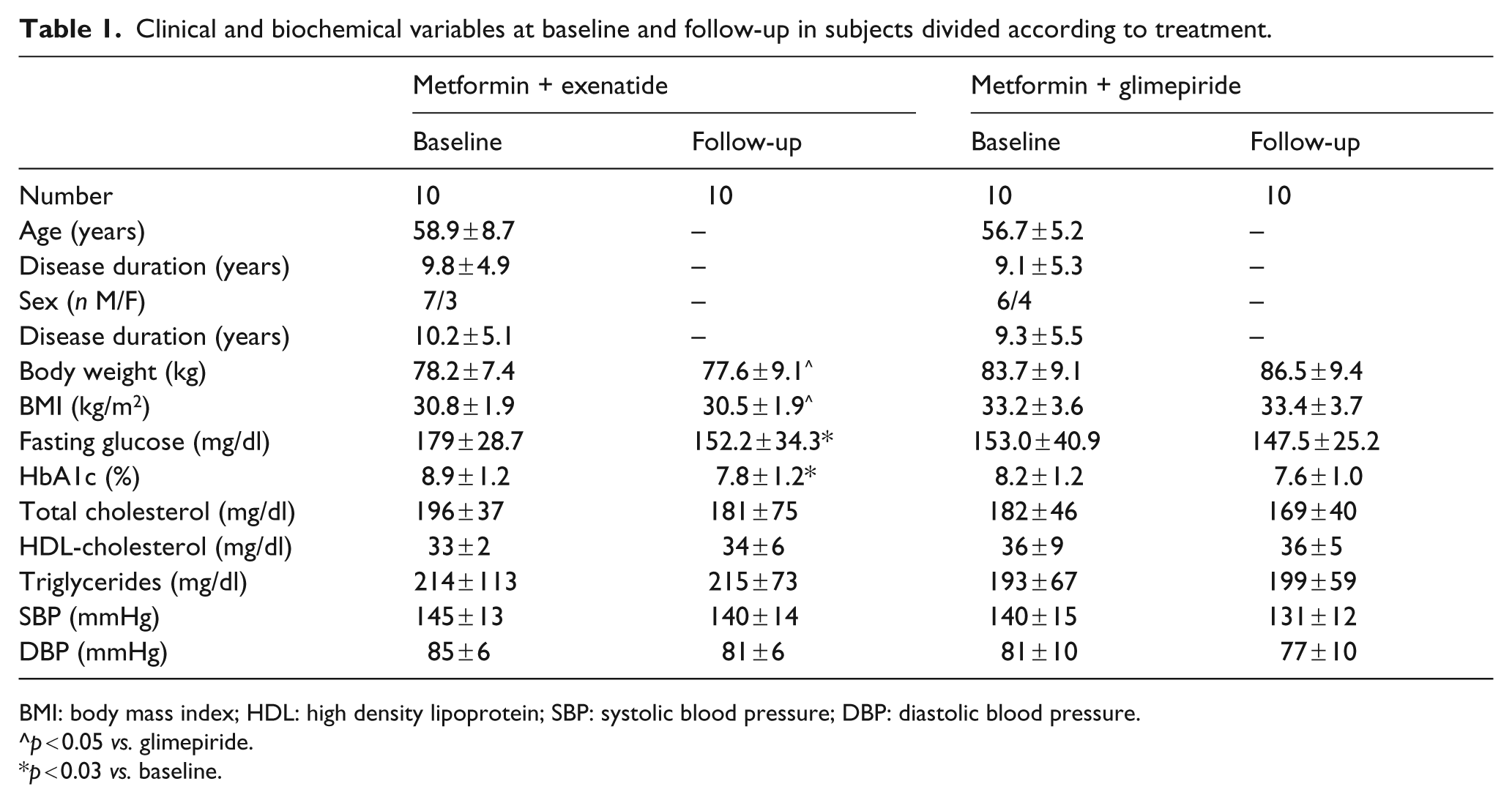
BMI: body mass index; HDL: high density lipoprotein; SBP: systolic blood pressure; DBP: diastolic blood pressure.
p < 0.05 vs. glimepiride.
p < 0.03 vs. baseline.
Table 2 shows the FMD time course in the two groups at baseline and at follow-up visit. At baseline, FMD was not significantly different between the two groups at each observation time, as well as peak-FMD. Baseline brachial artery diameter was 4.1 ± 1.1 mm in the glimepiride group and 4.2 ± 0.7 mm in the exenatide group (p = not significant). At follow-up visit peak-FMD was significantly improved in both groups even if the percentage increase was significantly higher in the exenatide compared with the glimepiride group. As far as time course is concerned, in the exenatide group FMD significantly increased at each observation time (50 s, 2 min and 3 min) after treatment compared with glimepiride group, who showed a significant increase only after 2 min. Due to the difference in metabolic control at baseline, and at the end of study period, we decided to evaluate again FMD in the exenatide and the glimepiride group including, in a further analysis, subjects comparable in sex, age, baseline fasting glucose and HbA1c, and who obtained a comparable fasting glucose and HbA1c at the end of the observation study. Sixteen subjects, eight in each group, met these criteria.
Flow mediated dilation (FMD) time course, peak FMD and shear rate area under the curve (SR AUC) at baseline and follow-up in subjects divided according to treatment.
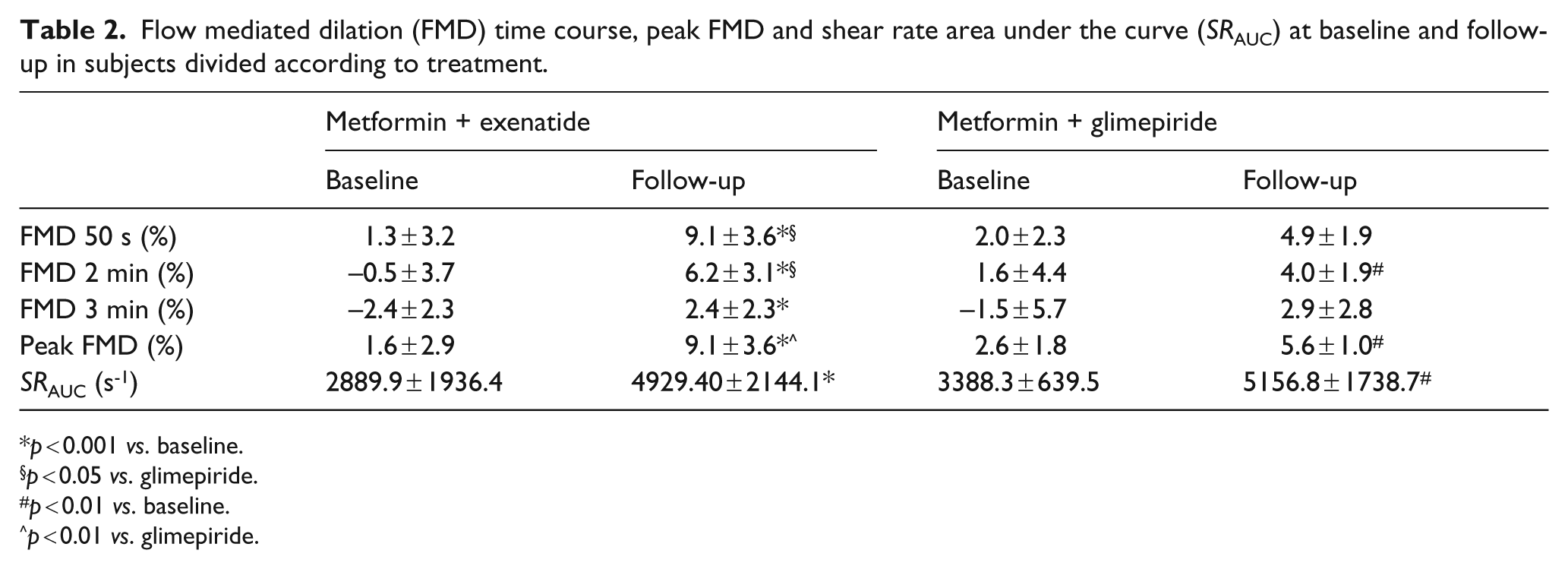
p < 0.001 vs. baseline.
p < 0.05 vs. glimepiride.
p < 0.01 vs. baseline.
p < 0.01 vs. glimepiride.
Fasting plasma glucose decreased by 10% and 14% in the exenatide and glimepiride groups, respectively (p = NS). Baseline values were 172 ± 25.2 mg/dl in the exenatide and 174 ± 35.8 mg/dl in the glimepiride group. HbA1c decreased respectively by 0.7% and 0.9% (p = NS), and baseline and follow-up values were not statistically different (baseline: 8.7% vs. 8.4%; follow-up: 8.0% vs. 7.5%, exenatide and glimepiride, respectively). Peak-FMD significantly improved in both groups after treatment: from 1.8 to 8.1% in the exenatide group, p < 0.0001; from 2.1 to 5.7% in the glimepiride group, p < 0.01. The percentage increase in FMD after 16 weeks was significantly higher in the exenatide compared with the glimepiride group (94 ± 21% vs. 56 ± 38%, p = 0.04). As reported in Table 1, subjects who were suggested to assume glimepiride as add-on therapy showed a significantly higher body weight compared with exenatide after treatment. Therefore we also evaluated, in a separate analysis, peak FMD after treatment including subjects with a comparable body weight before and after treatment. Then we compared 16 subjects, eight in each group. Baseline body weight was 80.2 ± 7.6 and 80.1 ± 8.1 kg in the exenatide group, and 85.0 ± 8.4 and 85.6 ± 8.7 kg in the glimepiride group, before and after treatment, respectively (p = NS). Peak FMD after 16 weeks was 5.5 ± 1.1% in the glimepiride and 8.6 ± 3.6% in the exenatide group (p < 0.05).
The total SR AUC significantly increased after treatment in the exenatide and glimepiride groups, and the mean values were comparable between the two groups.
In order to adjust the FMD for the total amount of the stimulus we calculated the FMD:SR AUC ratio. As displayed in Figure 1, despite a similar value at baseline visit, the FMD:SR AUC ratio was significantly higher at follow-up visit in the exenatide group. Finally, we performed multiple linear regression analyses, aimed to evaluate variables independently associated with peak FMD at follow-up. We designed two different models, one including age, sex, disease duration, exenatide/glimepiride treatment, BMI, fasting plasma glucose, HbA1c, SR AUC, hypertension and hyperlipidaemia as independent variables, and in the other blood pressure and blood lipids have been used instead of hypertension and hyperlipidaemia. In both models exenatide/glimepiride treatment was independently associated with peak FMD. In detail, beta coefficients were respectively 3.8 and 5.3 (p < 0.01). The other variable significantly associated with peak FMD was HbA1c in the second model: −1.8 (p < 0.01).
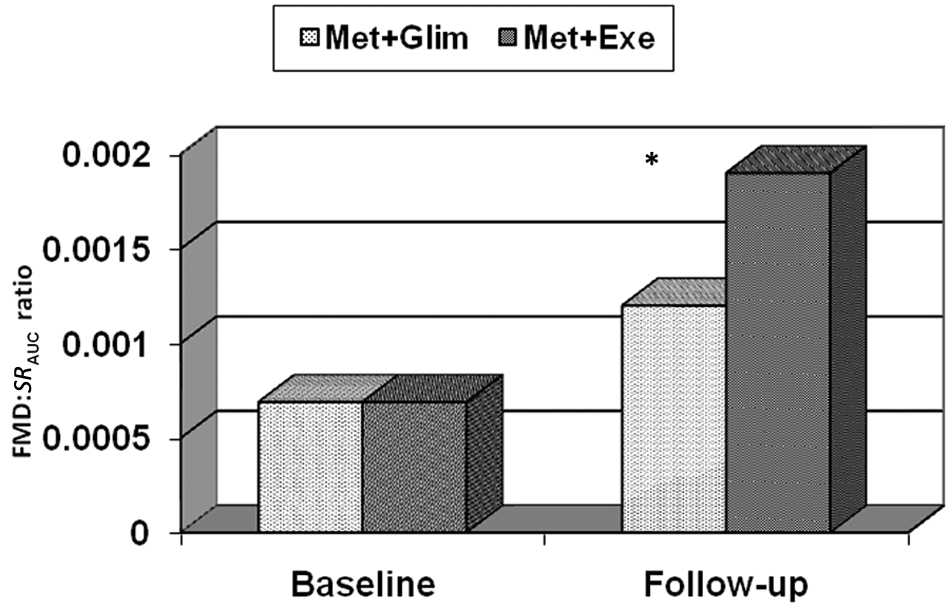
FMD:SR AUC at baseline and follow-up in subjects divided according to treatment.
Discussion
In subjects with type 2 diabetes not achieving an adequate glycaemic control with metformin, treatment with exenatide for 16 weeks induces a significant improvement in brachial artery endothelial function. Beneficial effects of GLP-1 and GLP-1 receptor agonist on cardiovascular risk factors are of great interest. In particular body weight reduction, blood pressure control and blood lipids reduction have been described in clinical trials.15,16 Our study first demonstrates a positive effect induced by exenatide, beyond metabolic control, on endothelial function evaluated by FMD technique, after chronic therapy. This finding confirms the paper by Koska et al., who found an improvement in post-prandial endothelial function, evaluated by peripheral arterial tonometry, after a single dose of exenatide, in individuals with recent onset diabetes or impaired glucose tolerance. 17 The technique used by Koska analyses blood flow in distal finger arterioles after reactive hyperaemia, in other words it evaluates the circulation in distal microvessels, or microcirculation. The FMD technique used in the present study, conversely, estimates directly the function of large conduit artery, through the variation of brachial artery diameter after stimuli, and indirectly evaluates the reactivity of peripheral resistance vessels, through the measurement of shear rate increase after ischaemia. 18
As shown in Table 2 and Figure 1, exenatide improved both arterial dilation and total SR AUC after ischaemia; moreover it significantly improved FMD:SR AUC as well. These results suggest that a pharmacological approach increasing GLP-1 receptor activation may have an effect on both micro- and macro-vessel function. This result is supported by previous in vivo experiment by Nyström et al., who reported the direct beneficial effect of GLP-1 on brachial artery endothelial function evaluated by FMD. 5 Very recently another paper has been published reporting an improvement in endothelial function after four-week treatment with vildagliptin, a Dipeptidyl-Peptidase-4 inhibitor. 19 In this study endothelial function has been evaluated after acetylcholine infusion in brachial artery. Acetylcholine stimulates endothelial muscarinic receptors, thereby activating nitric oxide synthase. This results in the endothelial release of nitric oxide in peripheral vessels with consequent increase in blood flow. The authors comment that the effect induced by vildagliptin may occur directly through the activation of GLP-1 receptor or alternatively by a GLP-1 receptor independent effect of the degradation product of GLP-1. Our results are in line with both these papers. Indeed subjects who were assuming exenatide showed an improvement in peripheral and conduit artery function.
Mechanisms activated by GLP-1 receptor agonist, and improving endothelial function, are definitely different and need to be further studied. A study by Erdogdu et al., performed in cultured human coronary endothelial cells, has demonstrated that the ameliorative action of GLP-1 on endothelial dysfunction is mediated by the activation of eNOS and Akt. 20 In addition to these mechanisms it is likely that the improved control of glucose metabolism has an effect on vascular function. Indeed, looking at the results, in both groups an improvement in glycaemic control occurred, even if the statistical significance was reached only in the exenatide group. Subjects who assumed glimepiride showed an improvement in brachial artery function and shear rate increase as well. The beneficial effect on vascular function in the glimepiride group might be related to alteration in glucose concentration, and possibly in vascular smooth muscle. 21 Shear rate is known to be the stimulus for endothelial release of vasodilatory substances inducing brachial artery dilation. It can be considered as a measure of microvascular reactivity after ischaemia. Recent evidences suggest that the peripheral reactivity associates with cardiovascular risk factors and incident cardiovascular events as well as FMD. Based on our results we could speculate that exenatide influences both peripheral and conduit artery reactivity as indicated by SR AUC increase and percentage increase in peak FMD, while glimepiride benefit is limited to microvessel circulation. 21 A possible additional mechanism induced by exenatide and influencing endothelial function could be the reduction of oxidative stress due to a better control on glycaemic variability. We have recently described how exenatide, compared with glimepiride, improves daily acute hyperglycaemia and indexes of glycaemic variability measured with continuous glucose monitoring. 22 This mechanism is further supported by another recent paper published by Ceriello et al. concerning the protective role of GLP-1 on endothelial function during the meal. 23 In this paper the authors suggest that the beneficial effect of GLP-1 is due to post-meal glycaemic control and the simultaneous improvement in insulin secretion. Reasonably, both these effects might control generation of reactive oxidative species (ROS), mostly in the post-prandial state. An additional benefit on endothelial function mediated by exenatide could be related to the improvement in insulin sensitivity and secretion. Recently it has been demonstrated that even if exenatide and glimepiride warrant a similar improvement of glycaemic control, only exenatide induces a substantial improvement in insulin resistance. 24
The present research has some limitations: the small number of subjects, the lack of a double blind design and the lack of matched groups. Despite these limitations the study suggests a beneficial effect of exenatide on endothelial function, which seems to be independent of blood glucose and body weight modification. Further randomised studies including a larger number of subjects, well matched for baseline metabolic parameters, are needed to confirm this finding. Finally, considering our results, it should be advisable to verify the efficacy of GLP-1 agonist receptor on both peripheral and conduit artery.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None declared.