
Abstract
Fluoroquinolone antibiotics cause rare, but clinically important, adverse events including hyperglycaemia and hypoglycaemia. The present study focuses on the possible effect of levofloxacin and moxifloxacin on the cardiovascular functions of rats with type I diabetes. Both antibiotics caused bradycardia. Levofloxacin but not moxifloxacin caused hypoglycaemia in diabetic rats and an increase in amplitude of the ST segment revealed by electrocardiogram (ECG) analysis of isolated hearts. In pressurized mesenteric arteries, levofloxacin did not affect the endothelium-derived hyperpolarising factor (EDHF) pathway or its main components, the small-conductance Ca2+ activated potassium (SKCa) and intermediate-conductance Ca2+ activated potassium (IKCa) channels. In moxifloxacin-treated rats, an increase in the EDHF response was observed, which was largely attributed to SKCa-activation. In conclusion, levofloxacin and moxifloxacin use appeared to vary but with no evidence of impairment of the cardiovascular function. However, it is still possible that these antibiotics may produce different effects if there are co-morbidities and therefore their use must be with care.
Introduction
Fluoroquinolones are frequently used for the treatment of uncomplicated and complicated urinary tract infections, bacterial sinusitis, skin and soft tissue infections, respiratory infections and nosocomial- and community-acquired pneumonia.1–3 However, the increasing prescription of these broad-spectrum antibiotics is associated with the emergence of bacterial resistance.3,4 Furthermore, some adverse drug reactions have been related to the use of these drugs and these necessitate careful selection of the fluoroquinolones by health providers, especially in patients with, or at risk of, diseases such as chronic heart failure and diabetes.5,6 These adverse drug reactions include the prolongation of the corrected QT (QTc) interval, torsade de pointes (TdP) (for example with use of sparfloxacin, grepafloxacin, moxifloxacin), and dysglycaemia (e.g. hyperglycaemia with gatifloxacin use in the elderly patients).7–9 Therefore, these fluoroquinolones (except moxifloxacin) were removed from the market.
Both, moxifloxacin and levofloxacin use was also associated with cardiac adverse effects, including prolongation of the QTc interval,10–13 polymorphic ventricular tachycardia, 14 TdP,7,15–17 and dysglycaemia (e.g. hypoglycaemia associated with levofloxacin use).8,18–20
Diabetes can lead to microvascular complications in which endothelial dysfunction plays an important role. 21 Several vasodilators are released by endothelial cells and contribute to the regulation of blood vessel tone. 22 Amongst these is endothelium-derived hyperpolarising factor (EDHF) which is produced by an increase in intracellular Ca2+ concentration ([Ca2+]i) and activation of both small-conductance Ca2+activated potassium (SKCa) and intermediate-conductance Ca2+activated potassium (IKCa) channels in endothelial cells. EDHF activates a number of hyperpolarising membrane constituents in neighbouring smooth muscle cells.23,24 EDHF is of particular importance in small blood vessels which are essential for the regulation of blood pressure. 25
The cardiovascular effects, as well as the effect on blood glucose levels, due to the use of fluoroquinolone antibiotics necessitate an investigation into the effect of these drugs on vascular function, especially in diabetes. The present study aims to investigate the effect of two widely prescribed fluoroquinolones on the EDHF and blood pressure responses in an animal model of type I diabetes.
Methods
Animals
Male albino Wistar rats (220–300 g; n = 32) were maintained in the laboratory animal unit of Aleppo University under standard conditions at 25 ± 2°C with a 12-hour dark–light cycle. They were fed with regular chow and given free access to water. Diabetes was induced by a single intravenous injection of streptozotocin (STZ; 60 mg/kg of body weight, dissolved in citrate buffer, pH 4.5) into the tail vein of animals. For controls, age-matched rats were injected with the same volume of citrate buffer only. Tail blood glucose was measured at weekly intervals using a one-touch glucometer. All experiments were performed after the STZ injection and when blood glucose level was above 350 mg/dl. Four weeks later, once diabetes was induced, rats were divided into three groups: control (STZ-diabetic) rats, rats with intraperitoneal injection of 80 mg/kg/day moxifloxacin, and rats with intraperitoneal injection of 100 mg/kg/day levofloxacin.26,27
These fluoroquinolone antibiotics are widely used for the treatment of several infectious diseases including respiratory tract infection for a period of up to 14 days.28–30 Therefore, STZ-diabetic rats were given intraperitoneal injections of levofloxacin or moxifloxacin daily for 14 days. The blood glucose was measured just before (0 hours), at 30 minutes, 60 minutes and three hours after the injection. Daily blood collection was avoided in order not to stress the animal, thus a blood sample was collected on day 1, 3, 5, 7, 10, and on day 14 when rats were killed and the functional experiments on isolated blood vessels and hearts were performed.
Body weight and biochemical measurements
Body weights were determined in all animal groups (treated and untreated with levofloxacin or moxifloxacin). Glucose levels were measured in samples taken from blood via the tail vein using the glucose oxidase method (BioSed, Italy). Insulin levels were measured using Ultra Sensitive Mouse Insulin ELISA Kit (Crystal Chem., Inc., Illinois, USA) with a microplate reader (Multiskan EX Microplate Photometer, Thermo Scientific, Schwerte, Germany).
Preparation of mesenteric arteries
Rats were anaesthetised with diethyl ether and euthanised by decapitation. Small mesenteric arteries (second order branch; approximate diameter 300–350 μm) were rapidly removed and placed in ice-cold Krebs solution (composition in m
Tail-cuff blood pressure measurements
Arterial blood pressure was measured non-invasively (Volume Pressure Recording; using a CODA 8-channel tail-cuff blood pressure system; Kent Scientific, Torrington, Connecticut, USA). Blood pressure (BP) (systolic, diastolic and mean) and heart rate (HR) measurements were performed after pre-warming the rats on a platform kept at 37°C, supplied with the CODA-8 channel system for 10 minutes. The proximal occlusion cuff constricts the tail artery, while the distal cuff detects changes in tail artery volume when blood flow resumes as the occlusion cuff deflates. Measurements based on the average of three sessions (each consisting of 15 cycles) were used for statistical analysis.
Electrocardiogram (ECG) recording
Control and diabetic rats were anaesthetised with sodium pentobarbitone (50 mg/kg, intraperitoneal), were given heparin (250 IU, intravenous), and were killed by cervical dislocation. Their hearts were rapidly excised and placed immediately into an ice-cold perfusion buffer. These were cannulated through the aorta in a Langendorff system, perfused with oxygenated (95% O2, 5% CO2) Krebs-Henseleit solution (composition in mM: NaCl 118.5, KCl 4.7, CaCl2 1.8, MgSO4 1.2, KH2PO4 1.2, glucose 11.0, NaHCO3 25.0, pH 7.4) at 37°C and allowed to stabilize for 30 minutes after being mounted. The initial perfusion pressure was kept constant at 80 mmHg. NO synthase inhibitor N-nitro-L-arginine (300 µM) and the cyclooxygenase inhibitor indomethacin (10 µM) were added to the perfusate to inhibit NO and prostaglandin synthesis, respectively. The ECG was recorded using an Animal BioAmp amplifier (ADInstruments Ltd, Oxford, UK).
Drugs
All materials were obtained from Sigma-Aldrich, UK except apamin (obtained from Latoxan, USA) and 1-[(2-chlorophenyl) diphenylmethyl]-1H-pyrazole (TRAM-34; obtained from Enzo Life Sciences, UK).
Data analysis
All values are given as mean ± standard error of the mean (SEM). The number of arteries from individual animals is given by n. Data were analysed using analysis of variance (ANOVA) (GraphPad Prism software version 4) followed by a Bonferroni or Newman Keuls post hoc-test, where applicable, and p < 0.05 was considered significant.
Results
Insulin levels, body and heart weights
Insulin levels and body weights were similar in both diabetic control rats and diabetic rats treated with levofloxacin or moxifloxacin. Heart, liver and lung to body weight ratios were comparable between all animal groups (Table 1). We did not observe any other abnormal signs on the antibiotic-treated rats such as weakness or hypothermia.
Insulin levels, body weights, heart/body weight, liver/body weight and lung/body weight ratios both in STZ-diabetic rats and in STZ-diabetic rats treated with levofloxacin and moxifloxacin (n = 30).
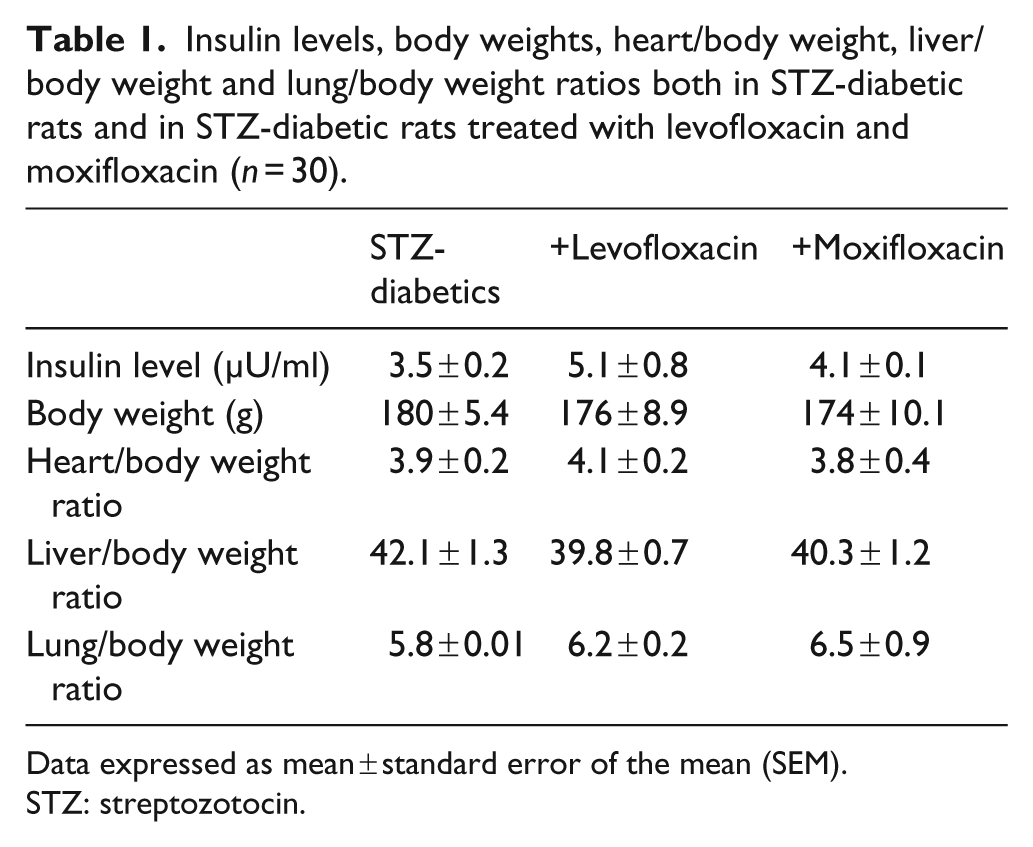
Data expressed as mean ± standard error of the mean (SEM).
STZ: streptozotocin.
Blood glucose levels
Different time points for measurement of blood glucose levels were chosen based on previous studies, which showed changes after 30 minutes (gatifloxacin and levofloxacin-induced hypoglycaemia in mice and rats, respectively)26,31 or after more than two days (hyperglycaemia in humans). 32
No significant changes of circulating glucose levels from those observed in diabetic rats were detected in the moxifloxacin group. In contrast, glucose levels after injection of levofloxacin tended to be lower; a significant reduction in these was observed after three hours and after 14 days (Table 2). It was observed that the blood glucose level tends to return to previous levels (before the injection of the antibiotic) at approximately 10 hours after the injection on days 1, 3 and 5 only.
Levels of blood glucose (in mg/dl) in STZ-diabetic rats treated with levofloxacin and moxifloxacin at different time intervals.
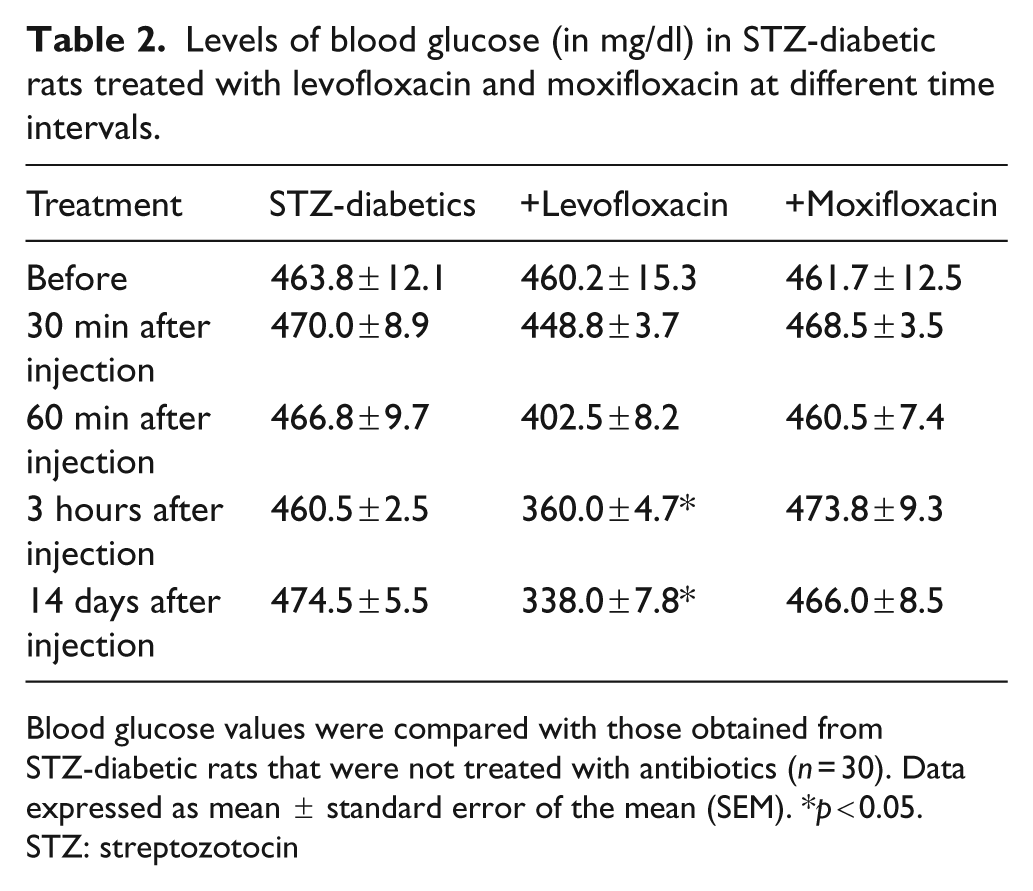
Blood glucose values were compared with those obtained from STZ-diabetic rats that were not treated with antibiotics (n = 30). Data expressed as mean ± standard error of the mean (SEM). *p < 0.05.
STZ: streptozotocin
Heart rate and blood pressure
Significant decreases in HR were observed in STZ-rats treated with levofloxacin or moxifloxacin (Table 3). Diastolic, systolic and mean pressures were not changed following treatment with levofloxacin or moxifloxacin (Table 3).
Heart rate (HR) and blood pressure (BP) in diabetic rats with and without treatment with levofloxacin or moxifloxacin (n = 30).
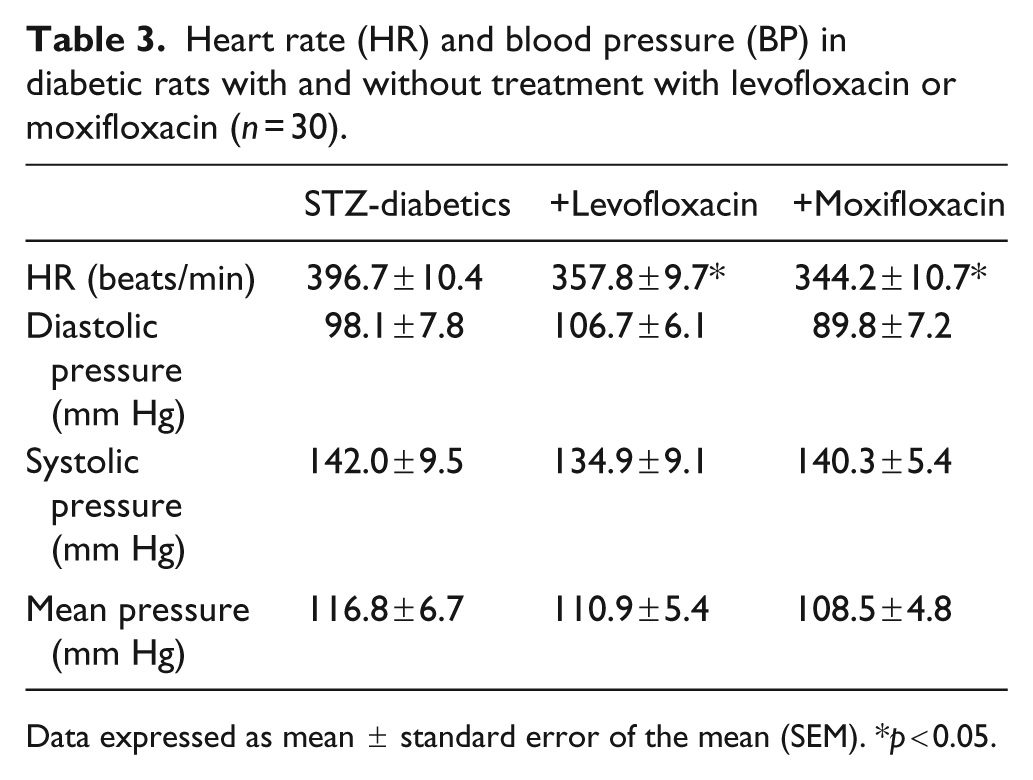
Data expressed as mean ± standard error of the mean (SEM). *p < 0.05.
Acetylcholine (ACh)-mediated EDHF response in mesenteric arteries
The level of relaxation due to 1 µM ACh was reduced in diabetic rats treated with levofloxacin. In contrast, moxifloxacin administration resulted in an approximately two-fold enhanced relaxation level (Figure 1).
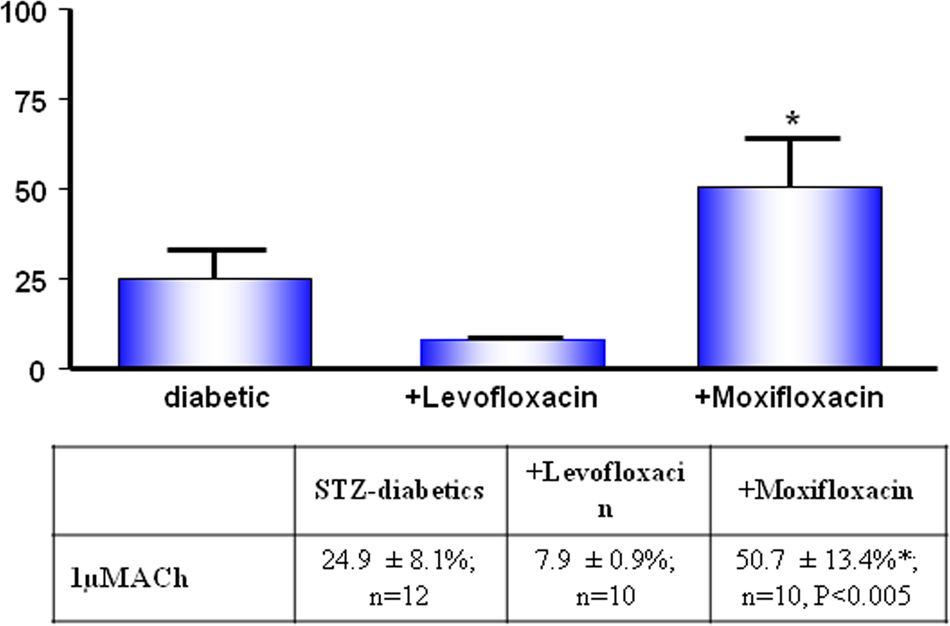
The effect of levofloxacin and moxifloxacin on the acetylcholine (ACh)-mediated relaxation of mesenteric arteries from both treated and untreated STZ-diabetic rats.
Responses to ACh were studied in the presence of either TRAM-34 (to block IKCa channel activity) or apamin (to block SKCa channel activity). In the presence of 1 µM TRAM-34 (SKCa-mediated responses), the relaxation to ACh in levofloxacin-treated diabetic rats was not significantly changed (Figure 2). On the other hand, in moxifloxacin-treated rats, ACh relaxation was increased about six-fold (Figure 3). ACh-induced relaxation mediated by IKCa (in the presence of apamin) was not significantly changed in diabetic arteries from the levofloxacin or the moxifloxacin group.
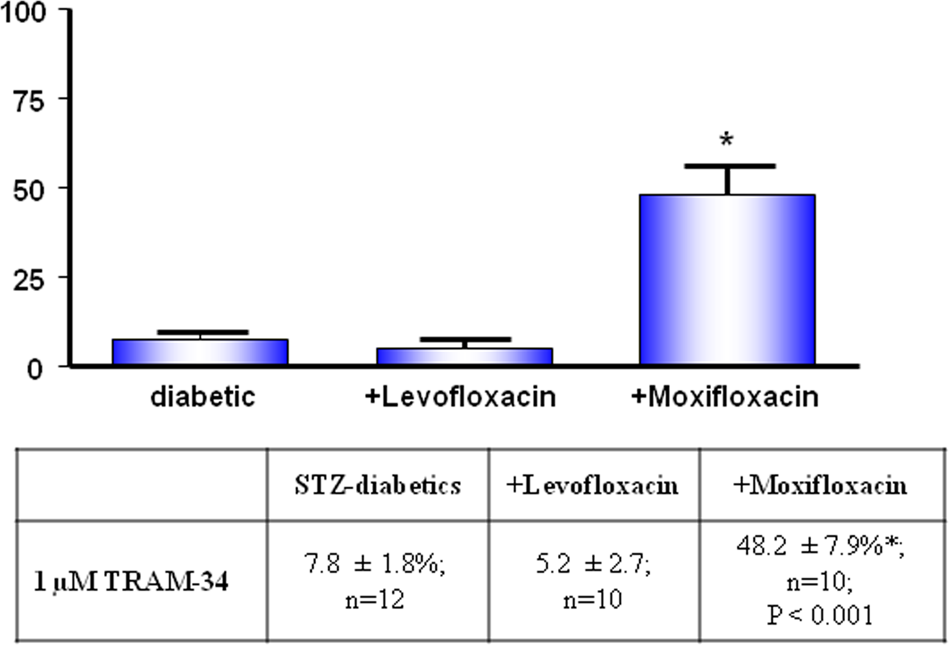
The effect of levofloxacin and moxifloxacin on small-conductance Ca2+ activated potassium (SKCa) channel-mediated relaxation (in the presence of 1 µM TRAM-34) of mesenteric arteries from both treated and untreated STZ-diabetic rats. Data represent mean ± standard error of the mean (SEM).
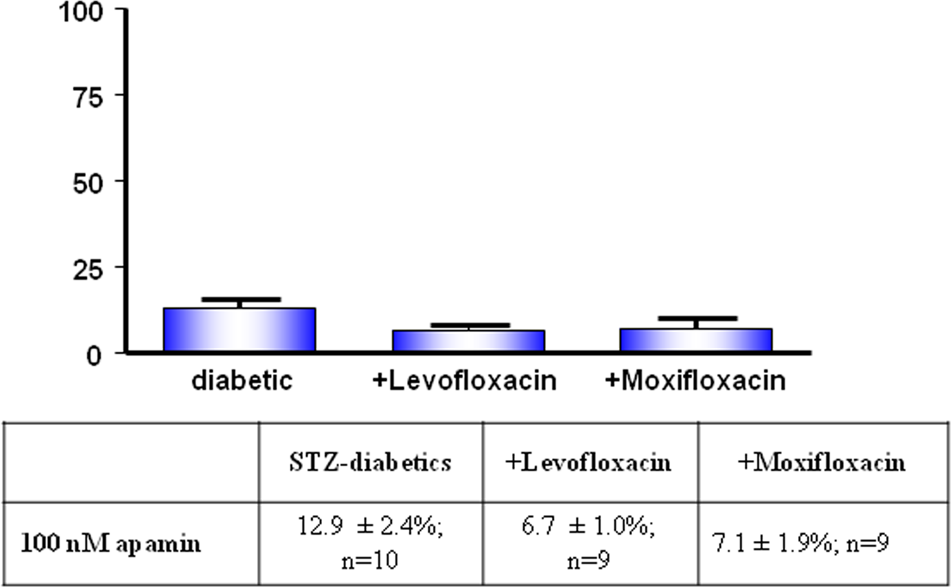
The effect of levofloxacin and moxifloxacin on the intermediate-conductance Ca2+ activated potassium (IKCa) channel-mediated relaxation (in the presence of 100 nM apamin) of mesenteric arteries from both treated and untreated STZ-diabetic rats. Data represent mean ± standard error of the mean (SEM).
ECG parameters of isolated hearts
There was no significant alteration in P duration, PR interval and QRS interval in diabetic rats treated with levofloxacin or moxifloxacin in comparison with control diabetic rats (Table 4). Similarly, QT interval was not significantly changed. However, ST amplitude was increased in levofloxacin-treated rats in comparison with diabetics (Table 4).
Electrocardiogram (ECG) parameters of the hearts obtained from diabetic rats without and following treatment with and levofloxacin or moxifloxacin (n = 6).
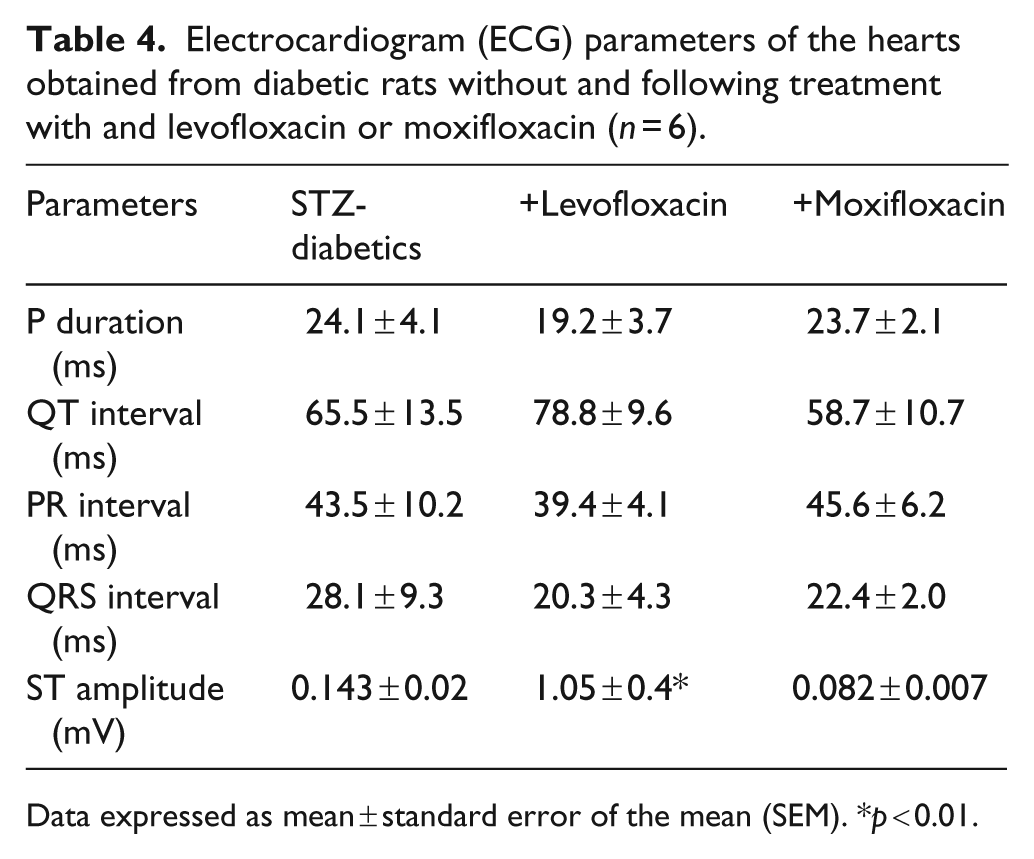
Data expressed as mean ± standard error of the mean (SEM). *p < 0.01.
Discussion
Levofloxacin and moxifloxacin are widely used antibiotics belonging to the third-generation of fluoroquinolones that have an extended spectrum of activity toward Gram-positive
bacteria. 33 They carry some cardiovascular risks such as prolongation of the QTc interval,10,16 of TdP7,15,17 and ventricular fibrillation.12,13 Dysglycaemia has also been associated with the prescription of fluoroquinolones (e.g. hyperglycaemia and hypoglycaemia associated with gatifloxacin and levofloxacin use respectively).8,18–20
Since levofloxacin and moxifloxacin are widely prescribed, the effect of these drugs on vascular function is becoming increasingly important, especially in diabetes, a disease which is strongly connected to cardiovascular complications. Therefore, the present study focused on the effect of these antibiotics on the cardiovascular function of STZ-diabetic rats, an animal model of type I diabetes.
Effects of levofloxacin and moxifloxacin on glucose levels
In the present study, we focused on studying the effect of fluoroquinolone antibiotics on the glucose level in STZ-diabetic rats and not controls (citrate buffer-treated rats; non STZ-rats) for the following reasons:
It was previously shown that levofloxacin administration is not accompanied by any change in plasma glucose levels in fasted or glucose-loaded mice. 31 In addition, moxifloxacin is less likely to affect blood glucose levels than levofloxacin. 26
Fluoroquinolone antibiotics are widely used for the treatment of respiratory tract infections especially in the developing countries where these antibiotics can be obtained, on many occasions, without prescription from pharmacies.28,34 Thus, any possible change in blood glucose and/or vascular function in response to these antibiotics is far more important in diabetic than in normal (healthy, control) individuals.
Upon comparing glucose levels between STZ-diabetic rats and STZ-diabetic rats after treatment with levofloxacin at different time points, a hypoglycaemic effect of levofloxacin was observed after three hours and after 14 days. In contrast, moxifloxacin did not affect the blood glucose levels of STZ-diabetic rats. These results are in agreement with previous studies in which levofloxacin has been shown to be more likely to lower blood glucose levels than moxifloxacin.8,18–20,26,35–37
Since, in the present study, the insulin levels of diabetic rats remained low even after 14 days of treatment, the hypoglycaemic action of levofloxacin is very likely not due to an insulinotropic effect of the drug. Instead, downstream insulin-independent mechanisms (such as enhanced activity of glucose transporters) must be involved.
The administration of moxifloxacin did not affect the diabetic state of the rat. In addition, the reduction in body weight, which accompanies diabetes in STZ-rats, was not affected by either levofloxacin or moxifloxacin. It is also noteworthy that cardiac hypertrophy was not observed in STZ-rats before, or after, treatment with levofloxacin and moxifloxacin.
The effect of levofloxacin and moxifloxacin on heart function
An elevation in the ST segment was observed in diabetic hearts from rats treated with levofloxacin but not with moxifloxacin. This side effect of the drug was not accompanied by dysrhythmia since other ECG parameters remain unchanged. Thus, P duration and PR interval (indicators of the atrioventricular conduction system of the diabetic heart) were not affected by levofloxacin or moxifloxacin treatment. Similarly, the QRS complex remained comparable between diabetic hearts from all treated and untreated rats indicating that the electrical conduction through the ventricles was unchanged.
Both levofloxacin and moxifloxacin treatment appeared to produce bradycardia in diabetic rats, in agreement with a report on gatifloxacin, another member of the fluoroquinolone family. 38 However, this effect was not associated with changes in BP.
The effect of levofloxacin and moxifloxacin on the vascular function
In the present study, EDHF relaxant effect induced via ACh was comparable between diabetic rats with and without treatment with levofloxacin. In contrast, a profound enhancement of the EDHF response was observed in diabetic rats treated with moxifloxacin, indicating that long-term exposure to this antibiotic produced some improvement in the mesenteric artery function. This could be attributed to the ability of moxifloxacin to selectively increase the function of endothelial SKCa channels, a major component of the EDHF pathway. This was based on the finding that in moxifloxacin treated diabetic rats, the SKCa and not IKCa-mediated relaxation of mesenteric arteries was markedly enhanced in comparison with SKCa and IKCa-mediated responses in diabetic rats. Moreover, in moxifloxacin-treated rats the EDHF response induced by ACh seemed to be largely obtained from the opening of SKCa channels.
Although the EDHF response remained unchanged in the diabetic rats treated with levofloxacin, whereas it was improved in the case of treatment with moxifloxacin, the effect of these antibiotics on other vasodilators (such as NO) cannot be excluded and is a matter for future investigation.
Conclusions
In STZ-diabetic rats, the administration of levofloxacin and moxifloxacin showed that:
Levofloxacin appeared to have hypoglycaemic action whereas moxifloxacin is without effect on blood glucose.
Both levofloxacin and moxifloxacin treatment are accompanied by bradycardia.
ECG parameters appeared comparable between diabetic rats and diabetic rats treated with levofloxacin and moxifloxacin with the exception that the former elevated the ST segment.
It seems that moxifloxacin potentiates the EDHF-mediated relaxation of mesenteric arteries, which can be attributed largely to the SKCa channels.
Thus, although these fluoroquinolones did not produce major impairment in the cardiovascular function of STZ-diabetic rats, it is still possible that these antibiotics may produce significant side effects if there are co-morbidities such as heart failure or diabetes. Furthermore, levofloxacin and moxifloxacin may exhibit different effects on the cardiovascular function in type II diabetes and therefore, they still must be used with care especially in long-term therapies.
Footnotes
Acknowledgements
This work was supported by Aleppo University, Syria.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest statement
The authors declare there are no conflicts of interest to disclose.