
Abstract
Introduction
The world prevalence of diabetes mellitus (DM) is predicted to increase to 439 million adults by 2030. 1 Cardiovascular complications account for the majority of deaths in patients with DM. Despite recent advances in medical therapy for acute coronary syndromes, patients with DM continue to have substantially worse clinical outcomes after acute myocardial infarction (AMI) than patients without these metabolic abnormalities. 2–7
Evidence for reduced mortality following administration of fibrinolytic therapy for ST-segment elevation myocardial infarction (STEMI) is compelling. However, thrombus in patients with DM may be resistant to lysis, 8 potentially limiting the efficacy of this strategy in this group of patients. It is well known that DM is associated with impaired outcomes following STEMI treated with fibrinolysis. 9 Primary percutaneous coronary intervention (PPCI) offers advantages over fibrinolysis in achieving coronary reperfusion. 10 Recognition that PPCI is associated with improved clinical outcomes compared with fibrinolysis has led to the recommendation that PPCI is offered as the preferred reperfusion strategy for patients with STEMI. 11–13 Despite these clinical advantages, several reports suggest that outcomes remain sub-optimal in patients with DM treated with PPCI compared with those without diabetes. 9,13–16 Interpretation of these studies, however, is limited by their small size or the fact that they pre-dated routine stent implantation, high-pressure stent deployment, utilisation of drug-eluting stents and the administration of intensive dual oral anti-platelet therapy.
Here we set out to determine whether DM remains associated with higher mortality after STEMI in a large group of ‘real-world’ patients treated in the contemporary PPCI era.
Research design and methods
We carried out a retrospective analysis of a registry of all patients undergoing PPCI for STEMI at Leeds General Infirmary, United Kingdom (catchment population of ~3.2 million) between March 2005 and September 2009. STEMI was diagnosed as chest pain consistent with myocardial ischaemia for 20 min or more associated with ST-segment elevation of ≥1 mm in two or more adjacent limb leads, or ≥2 mm in two or more adjacent precordial leads, or presumed new left bundle branch block, on a standard 12-lead electrocardiogram. 15 Initial diagnosis of STEMI was made by ambulance crews or emergency department physicians. PPCI was offered as the default reperfusion strategy to patients with STEMI presenting within 12 h of the onset of symptoms. Patients receiving initial assessment in a peripheral hospital were defined as indirect admissions to the intervention centre; the remaining patients were deemed to have been directly admitted.
All patients received pre-procedural loading doses of aspirin (300 mg) and clopidogrel (300–600 mg). Procedural decisions, including device selection and adjunctive pharmacotherapy, were made at the discretion of the physician performing PPCI. During the study period patients underwent balloon angioplasty with stenting (bare-metal or drug-eluting stents), direct stenting, or thrombus aspiration prior to stenting. An anticoagulation strategy of either bivalirudin or weight-adjusted unfractionated heparin in combination with a glycoprotein IIbIIIa antagonist was used at the operator’s discretion.
Blood tests were performed at the time of admission to the intervention centre. Admission hyperglycaemia was defined as admission plasma glucose ≥11.0 mmol/L regardless of diabetes status. Patients were classified as having DM if they had a history of DM, regardless of glycaemic status at admission. 14 This is because some patients presenting with hyperglycaemia may not go on to fulfil the diagnostic criteria for DM when assessed after stabilisation. Data were collected regarding smoking status, history of cerebrovascular disease and history of peripheral arterial disease. A coronary vessel was considered diseased when it contained at least one lesion with >70% diameter stenosis by visual assessment. Coronary perfusion was graded according to the classification system of the Thrombolysis in Myocardial Infarction (TIMI) trial. 16 Door-to-balloon time was defined as the interval from arrival at the first hospital door (district general hospital or tertiary interventional centre) to the time of first balloon inflation or first use of a thrombectomy device. 17 Symptom-to-balloon time was taken from the patient’s first self-reported experience of symptoms suggestive of myocardial ischemia. Call and door times were abstracted from the ambulance transfer report. Balloon time was taken from the catheterisation laboratory technician’s report. Data were collected on a case record form and subsequently entered into a computerised database.
Statistical methods
Categorical data are displayed as percentage (number) and compared using Pearson χ2 tests. Normally distributed continuous data are displayed as mean (standard error of the mean) and compared with Student’s t-tests, whereas non-parametric data are displayed as median (inter-quartile range) and compared using Mann–Whitney tests. Log-rank tests were used to compare group mortality, and Cox-regression analysis was used to perform multivariable analysis. Partial residuals were used to check assumptions of proportional hazards. Potential confounders were included in multivariable models on the basis of clinical relevance and inter-group differences. Landmark analysis was used to define the persistence of mortality differences between groups beyond 30 days post-PPCI. All analyses were performed with SPSS version 12 (SPSS Inc., Chicago, IL, USA). Statistical significance was defined as p<0.05.
Results
Baseline characteristics of patients with and without DM are presented in Table 1. During the study period 2586 patients underwent PPCI for STEMI; 310 (12%) patients had a history of DM. Follow-up data were available for a median 661 (406–970) days; within the entire cohort this equated to 5,144 patient-years. Patients with DM were older (64.5 [0.7] vs. 62.3 [0.3] years; p=0.006) and less often male (67.1% vs. 72.9%; p=0.033) or smokers (28.9% vs. 48.3%; p<0.001). Hypertension (55.1% vs. 28.6%; p<0.001), cerebrovascular disease (7.3% vs. 3.1%; p<0.001) and peripheral arterial disease (4.6% vs. 1.9%; p=0.002) were all more common among patients with DM. In addition, more patients with DM had a history of previous myocardial infarction (26.3% vs. 13.5%; p<0.001) or coronary artery bypass graft surgery (5.3% vs. 2.7%; p=0.016). Coronary artery disease more frequently involved all three major epicardial arteries in patients with DM (33.8% vs. 20.2%; p<0.001). Cardiogenic shock at presentation was not significantly different in patients with DM (4.2% vs. 2.8%; p=0.16).
Baseline characteristics of patients with and without diabetes
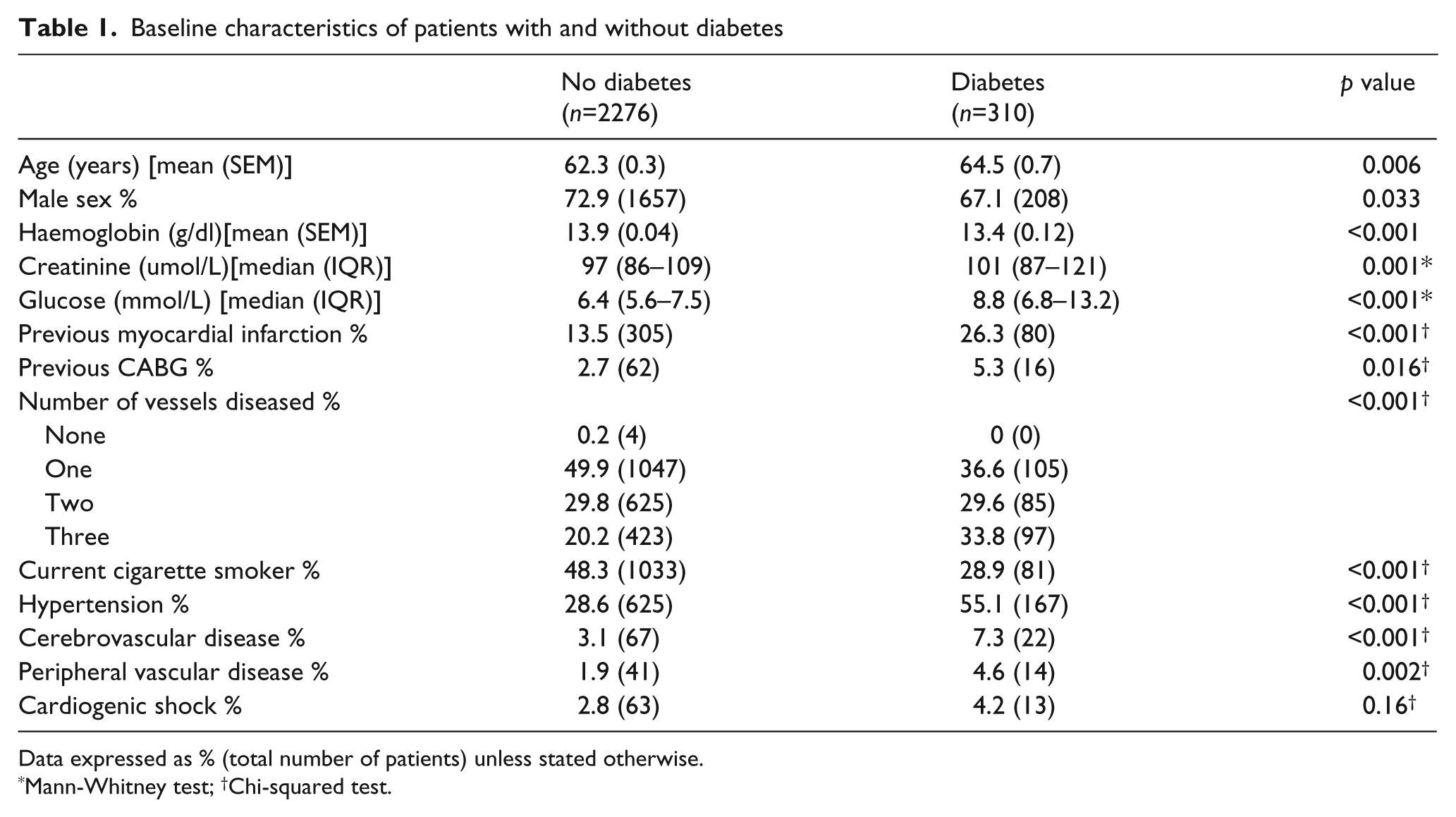
Data expressed as % (total number of patients) unless stated otherwise.
Mann-Whitney test; †Chi-squared test.
Procedural characteristics are summarised in Table 2. More drug-eluting stents were deployed in patients with DM (% of stents that are DES 40.6% vs. 31.7%; p=0.003). However, there were no significant differences in the use of intra-aortic balloon pump counter-pulsation, glycoprotein IIb/IIIa antagonists, bivalirudin, aspiration thrombectomy devices or radial artery access route between the two groups. Patients with DM had higher infarct-related artery TIMI flow grade at baseline, though post-procedurally TIMI flow grade was lower in patients with DM (p=0.031). More patients with DM required inter-hospital transfer for PPCI (48.3% vs. 38.3%; p=0.002) rather than being admitted direct to the interventional centre. Furthermore, symptom-to-balloon time (249 [169–407] vs. 211 [152–338] min; p<0.001) and door-to-balloon time (105 [56–166] vs. 86 [51–139] min; p=0.002) were longer in patients with diabetes. Door-to-balloon time was not influenced by the presence of peripheral arterial disease (89 [63–122] vs. 89 [51–141] min; p=0.63).
Procedural characteristics of patients with and without diabetes
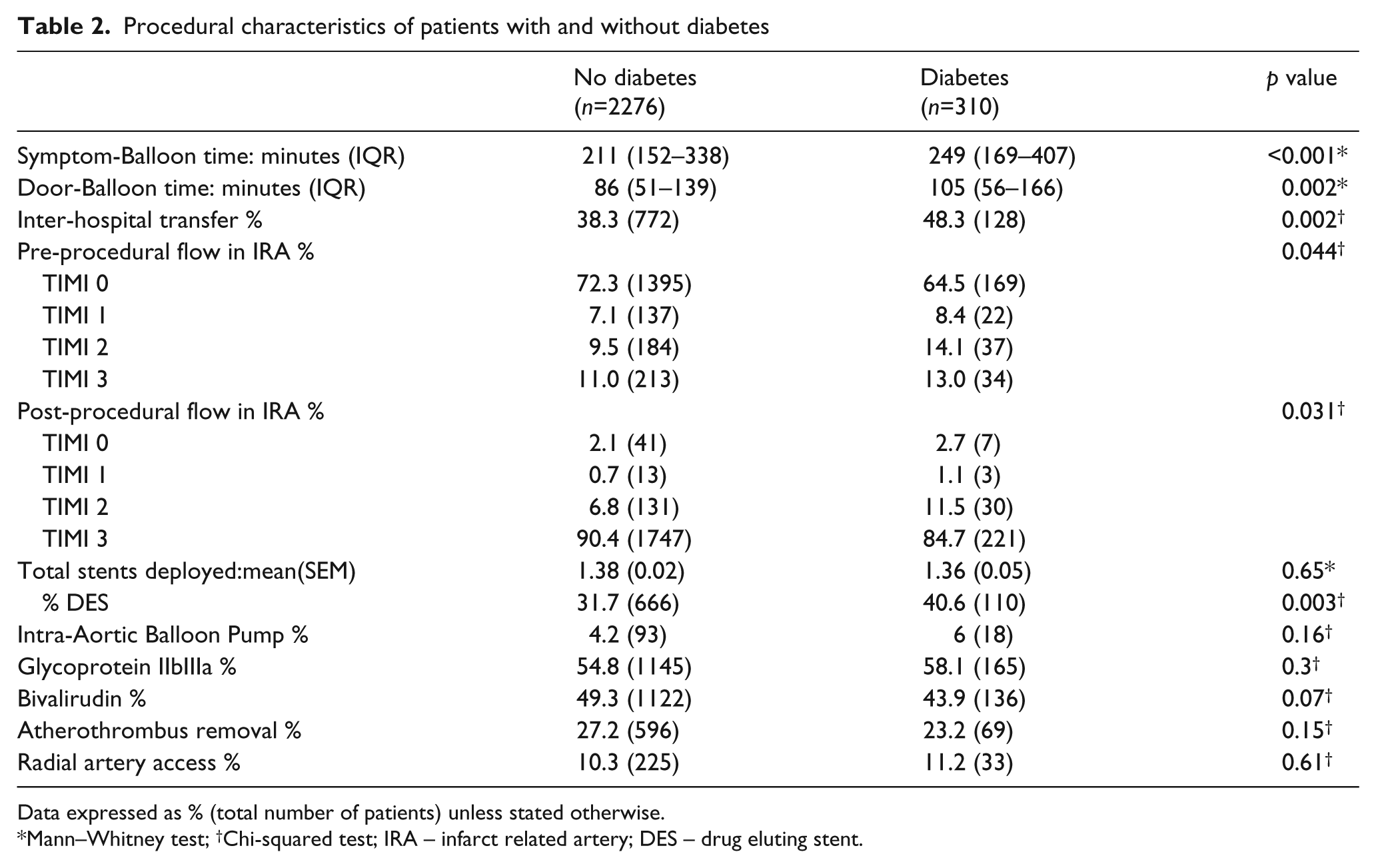
Data expressed as % (total number of patients) unless stated otherwise.
Mann–Whitney test; †Chi-squared test; IRA – infarct related artery; DES – drug eluting stent.
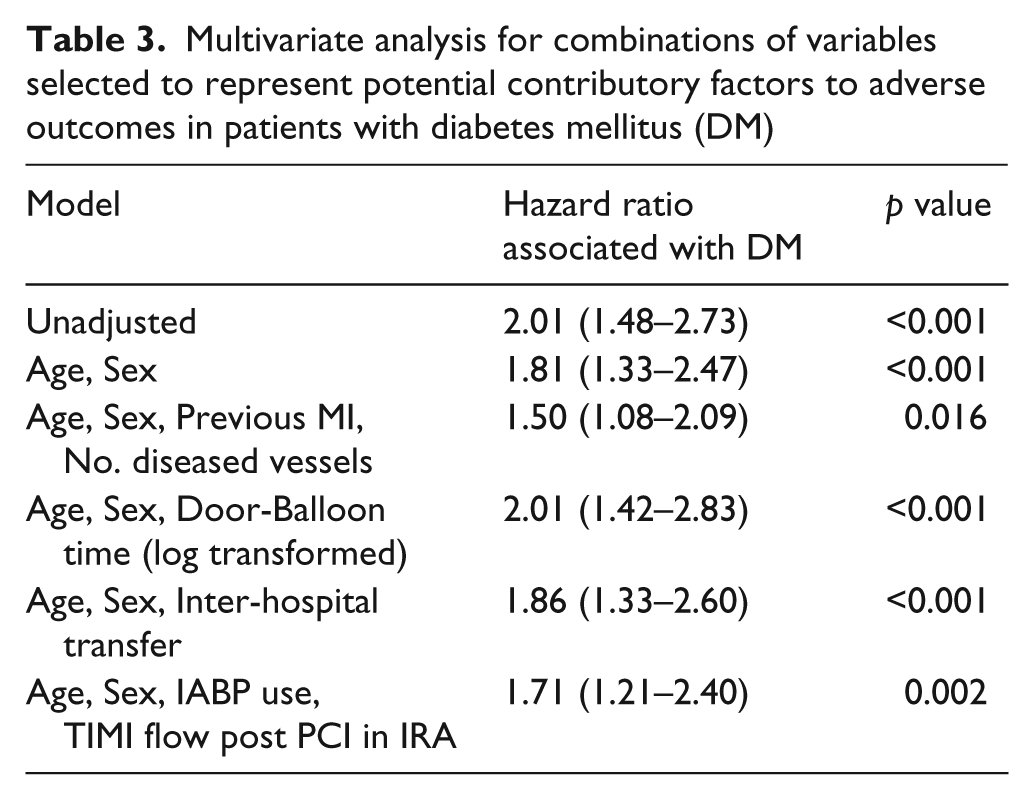
Kaplan–Meier all-cause mortality curves for patients with and without DM are shown in Figure 1a. Absolute all-cause mortality at 30 days (7.4% vs. 3.8%; p=0.0025) and mortality risk at 1 year (13.9% [43] vs. 6.5% [149]; p<0.0001) were significantly higher in patients with DM. Landmark mortality curves beyond 30 days after PPCI (Figure 1b) show ongoing divergence, confirming DM was associated with greater mortality beyond the ‘short-term’ post-MI phase (Log-rank p=0.0008). Admission hyperglycaemia was associated with increased mortality in the whole cohort (hazard ratio [HR] 1.11 (1.07–1.16); p<0.001); however, there was no interaction between DM status and glucose in predicting mortality (p=0.21). After multivariable adjustment for combinations of variables selected to represent potential contributory factors to adverse outcomes in patients with DM, diabetes remained independently associated with an increased mortality hazard (Table 3).
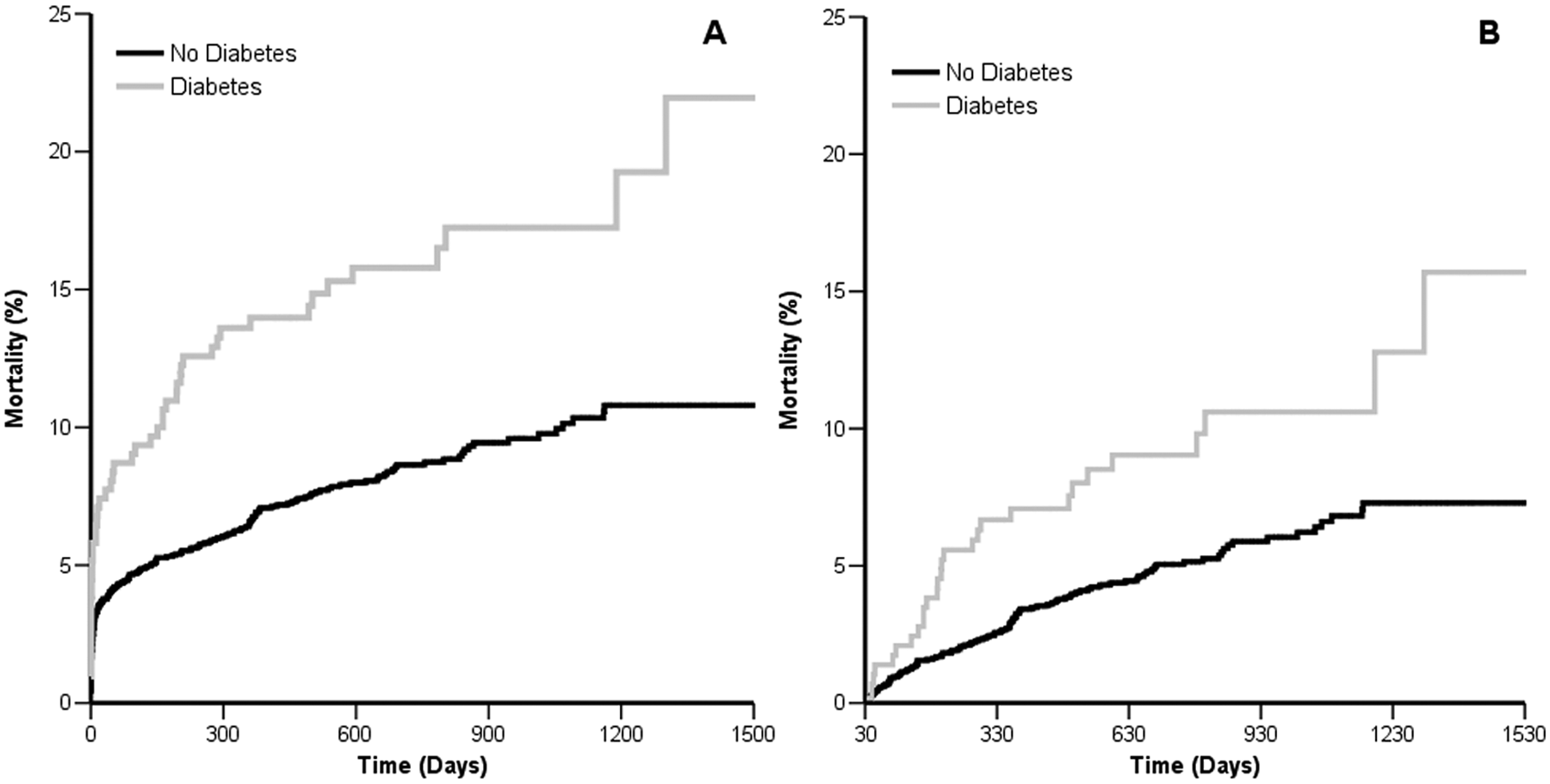
A. Kaplan–Meier mortality curves for patients with and without diabetes. B. Landmark Kaplan–Meier mortality curves for patients with and without diabetes beyond day 30 post-primary percutaneous coronary intervention.
Multivariate analysis for combinations of variables selected to represent potential contributory factors to adverse outcomes in patients with diabetes mellitus (DM)
Discussion
In this large ‘real-world’ registry of contemporary PPCI, we found that all-cause mortality following STEMI was approximately two-fold higher in patients with a history of DM compared with those without. Although inferences regarding causation cannot be drawn from registry data, our findings confirm that survival remains sub-optimal despite recent advances in management of STEMI and provide a number of potential insights into possible explanatory factors for the mortality risk conferred by DM. Our findings of greater co-morbidity, presence of more advanced coronary disease, poorer post-procedural coronary reperfusion, longer door-to-balloon times and more inter-hospital transfer in patients with DM are of particular relevance.
The mortality risk conferred by DM in our study is in keeping with previous reports of outcomes following PPCI for STEMI stratified according to DM status. 14,18,19 Our study builds on these observations by demonstrating an enduring survival disadvantage attributable to DM in a larger group of unselected patients managed using contemporary PPCI techniques including routine high-pressure stent deployment, drug-eluting stents, thrombus aspiration and dual oral anti-platelet therapy. These findings are of considerable global public health significance since the prevalence of diabetes is expected to double by the year 2030. 1 In contrast to other studies in which admission hyperglycaemia was associated with increased mortality independent of DM status, 14,20 in the current study there was no interaction between DM status and admission glucose concentration in predicting death.
DM is associated with increased mortality and morbidity following fibrinolysis for STEMI. 9 Several factors may account for the poorer outcomes associated with DM in a fibrinolysis-based reperfusion strategy. Patients with DM are less likely to receive fibrinolytic therapy, 21 and often receive it later than non-diabetic patients. 9 Fibrinolytic agents also have reduced efficacy in patients with impaired glucose tolerance. 9 For the majority of patients, PPCI has become established as the reperfusion modality of choice due to its superior clinical outcomes and lower mortality. 13 Despite this, the success of PPCI in patients with DM may be impaired by similar limitations to fibrinolytic therapy. The Second Danish Trial in Acute Myocardial Infarction (DANAMI-2) reported that DM reduces the beneficial effect of PPCI on long-term risk of clinical re-infarction. 22 In line with our observations, Ishihara et al. reported that admission hyperglycaemia and diabetes were both associated with poorer outcomes following PPCI. 14
Our findings provide a number of potential insights into the mechanistic basis for the survival disadvantage attributable to DM following PPCI. Firstly, we found that patients with DM more frequently had multi-vessel coronary artery disease and a history of previous myocardial infarction compared with patients without DM. Although we did not collect data on the presence of chronic coronary occlusions in this study, it has recently been demonstrated that multi-vessel coronary disease with chronic occlusion of a non-infarct-related artery is a strong independent predictor of mortality in patients with DM undergoing PPCI. 23 As we previously reported in a non-PPCI population, the adverse effect of DM on survival following myocardial infarction appears to be greatest in patients with a history of previous infarction. 4
Secondly, the lower post-procedural TIMI flow grade in patients with DM may jeopardise myocardial salvage and contribute to subsequent mortality. A number of factors which compromise coronary reperfusion could contribute to the lower TIMI flow in patients with DM, including increased platelet aggregation, enhanced thrombogenicity, underlying endothelial dysfunction and diminished flow reserve in these patients. 24 Although not specifically addressed in our study, diminished microvascular perfusion after PPCI may also contribute to adverse outcomes in patients with DM. 25,26
Thirdly, we have demonstrated that patients with DM more often required inter-hospital transfer and had significantly prolonged symptom and door-to-balloon times in comparison with patients without DM. Clinical assessment at a remote emergency department followed by inter-hospital transportation is time consuming and, as we have previously reported, may significantly increase door-to-balloon times. 17 Within our region, the maximum distance for inter-hospital transfer is approximately 22 miles, and so it likely that in geographically larger catchment areas the presence of DM may have a greater impact on door-balloon time. Although we can only speculate on reasons for more frequent inter-hospital transfers and delays to reperfusion, atypical presenting symptoms are common in patients with DM and may lead to a delay in diagnosis or may prompt an emergency ambulance crew to proceed to the nearest hospital rather than transferring the patient direct to the interventional centre. 27 It is tempting to speculate that by encouraging a lower threshold for transferring patients with DM and suspected STEMI directly to the interventional centre, symptom- and door-to-balloon times, and possibly outcomes, could be improved for patients with confirmed STEMI. Certainly, a shorter door-to-balloon time is associated with lower mortality, 28 particularly in high-risk patients 29 or those with recent symptom onset, 30 although this has not been specifically investigated in patients with DM.
While observational studies such as this provide important information on clinical outcomes in patients in a real-world setting, potential limitations should be acknowledged. Since DM was defined on the basis of self-reported history, it is possible that patients with undiagnosed DM, a common phenomenon in patients with AMI, 31 were included in our non-DM group. However the prevalence of DM in our study is consistent with that in a large randomised trial of PPCI, 16 and any misclassification of DM in our series would tend to diminish the true difference between groups and underestimate any effect of DM. Only patients surviving to arrival at the cardiac catheter laboratory and undergoing PPCI are included in our analysis; it is difficult to systematically account for patients who die before receiving medical assistance. Therefore, this analysis should only be interpreted in the context of patients who receive PPCI, rather that those who may be eligible for PPCI. Data relating to other potentially relevant variables including left ventricular ejection fraction, usual medication, insulin prescription, location of infarction, DM duration and glycaemic control would have been useful in multivariable analysis but were not routinely collected in our database. Finally, in our study DM remained associated with increased mortality after multivariate adjustment for age, sex, previous MI, prolonged door-to-balloon time and extent of coronary disease. Thus, while the factors discussed above may contribute to poorer outcomes, other DM-related factors are clearly important and require further study.
In summary, our study of a large unselected group of patients with STEMI confirms that DM remains associated with increased mortality despite contemporary treatment with PPCI, and highlights differences in patient and procedural characteristics associated with DM. While many of the factors potentially contributing to increased mortality are non-modifiable in the emergency setting, our findings raise the possibility that strategies to diagnose STEMI early in patients with DM and adopting a low-threshold for direct admission to an interventional centre for assessment may improve clinical outcomes and survival in these high-risk individuals.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
None declared.