
Abstract

An 87-year-old male was admitted with a 2-week history of fever, chills and burning micturition. He had comorbidities, including diabetes mellitus, coronary artery disease (postangioplasty) and hypertension, for which he was on multiple medications, including dual antiplatelet therapy. He was diagnosed with a urinary tract infection and treated with antibiotics. Additionally, the patient had severe anaemia (Hb 6.4 g/dL) secondary to iron deficiency and underwent upper gastrointestinal (GI) endoscopy.
Upper GI endoscopy revealed whitish, slough-like membranes covering most of the midesophagus, with underlying normal mucosa (Figure 1). He also had a hiatus hernia and normal gastric mucosa. Biopsies were taken from the esophageal mucosa for histopathological examination, which revealed superficial fragments of stratified squamous epithelium with intraepithelial neutrophilic and sparse lymphocytic infiltrates, focal intraepithelial microabscesses, intercellular edema and surface parakeratosis (Figure 2). On the basis of these endoscopic and histopathological findings, the patient was diagnosed with esophagitis dissecans superficialis (EDS). He was subsequently started on oral proton pump inhibitor therapy.
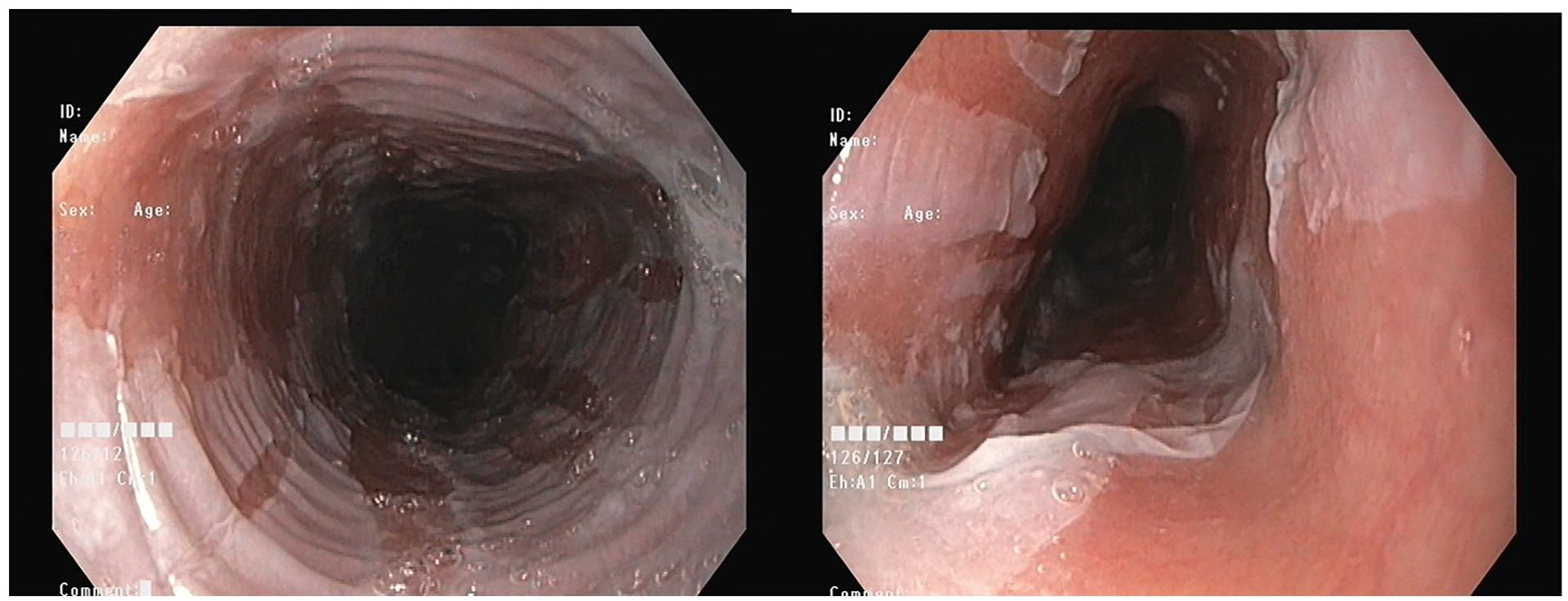
Endoscopy showing esophageal mucosa covered by whitish membranes.
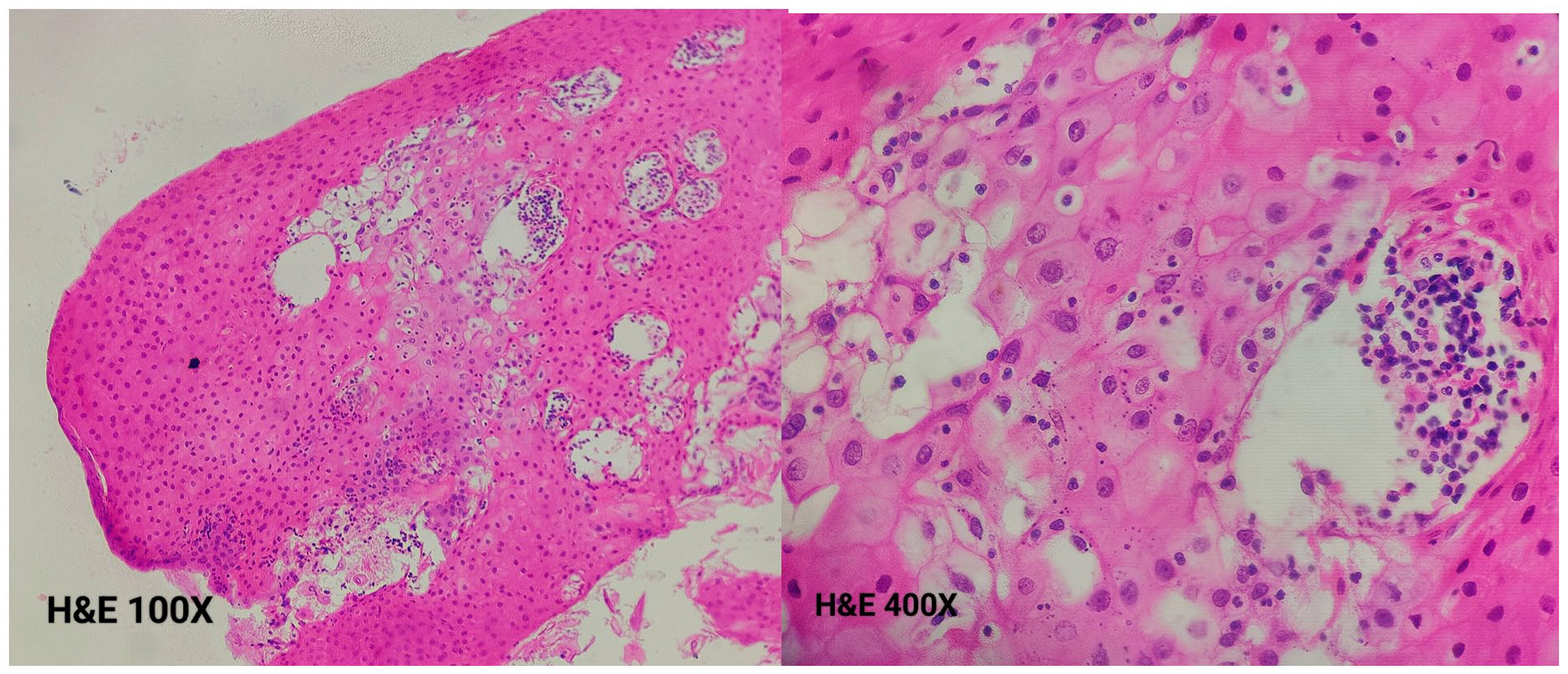
Histopathology section revealing intraepithelial infiltrates composed predominantly of neutrophils, focal intraepithelial microabscesses, intercellular edema and surface parakeratosis.
EDS is a desquamative, benign condition of the esophagus that is diagnosed on the basis of endoscopic findings. 1 It is typically an infrequent, incidental finding that is often missed or misdiagnosed during endoscopy. Additionally, histopathological findings are frequently overlooked due to contamination of the samples. 2 Although no identifiable cause is found in most cases, EDS is known to be associated with mucosal irritants, including medications, smoking, alcohol and bullous skin conditions.
Footnotes
Acknowledgements
None.
Author contributions
F Mohammed edited the manuscript and revised the manuscript for intellectual content. B Musunuri and S Shetty wrote and revised the manuscript for intellectual content. M Murali and Geetha V provided the histological images and evaluation. All the authors approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Informed consent was obtained for this case report.
Guarantor
B Musunuri.