
Abstract
We examined 11 pediatric patients with eosinophilic esophagitis with a tardy diagnosis. The symptoms were initially thought to be related to other diseases, leading to the use of inadequate therapeutic approaches. The patients were between 3 and 17 years old (mean 7.8 ± 3.8 years), and 8 of the patients were male. Common symptoms included abdominal pain, regurgitation, difficulty in gaining weight, vomiting, dysphagia, and coughing. The mean age for the onset of symptoms was 4.3 ± 2.9 years. Endoscopic findings included normal mucosa in five (45%) patients, thickening of the mucosa with longitudinal grooves in three (27%), erosive esophagitis in two (18%), and a whitish stippling in one (9%) patient. Treatment included the use of a topical corticosteroid for 10 patients. In eight (73%) cases, the treatment made the symptoms disappear. Ten patients underwent histopathological management after treatment, with a decrease in the number of eosinophils.
Introduction
Eosinophilic esophagitis (EoE), also known as allergic esophagitis and primary eosinophilic or idiopathic eosinophilic esophagitis, 1 is an inflammatory disease of the esophagus that affects children and adults. The disease was first described in children in 1995. 2 The increased incidence of EoE in recent years has been explained either by a real increase in its prevalence caused by the global rise in allergic diseases or by better knowledge of the disease's existence, as represented by the performance of a greater number of upper gastrointestinal endoscopies (UGE) and esophageal biopsies. 3 Currently, there are no symptoms, changes to the objective examination, serum biomarkers, or pathognomonic endoscopic findings for this disease. Thus, other causes of esophageal eosinophilia must be excluded, including gastroesophageal reflux disease (GERD), eosinophilic gastritis (EG), intestinal parasites, persistent vomiting, inflammatory bowel disease, and immune or tumor pathology.
An endoscopic esophageal biopsy is essential for establishing a diagnosis.4–7 The lack of knowledge regarding EoE-affected children and adults has delayed diagnosis and treatment. Given this context, the aim of this study was to present a series of 11 pediatric cases of EoE in northeastern Brazil and clinical features that delay diagnosis and treatment.
Methods
The present investigation was an observational and descriptive study of 11 pediatric patients who were diagnosed with EoE and treated at a Teaching Hospital in Fortaleza in northeastern Brazil.
The patients were selected from a group of 100 children who underwent an endoscopy to investigate symptoms related to the upper digestive tract. Biopsies of the esophagus, antrum, and duodenum were obtained by routine pediatric endoscopy procedures.
A diagnosis of EoE was obtained through the histological study of biopsies of the distal esophagus, which were stained with hematoxylin and eosin and reviewed by a single pathologist. The biopsies were considered to be diagnostic when exhibiting more than 15 eosinophils per high power field in the area of greater concentration without concomitant eosinophilic infiltration in the antrum and/or duodenum.4–7
Variables examined included gender, age at diagnosis of EoE, age at the onset of symptoms, clinical complaints, initial clinical diagnoses, tests performed, treatments prior to the histopathological diagnosis of EoE, endoscopic diagnoses, histopathological diagnoses, treatment after histopathological diagnosis, and treatment outcome.
The patients’ caregivers were informed about the purpose of the research and consented to their children's participation in the study. The study was approved by the Research Ethics Committee of the Faculdade Christus and was registered under the number 116.351.
Results
Eleven patients were included in the study (Table 1); eight were male. The subjects’ ages ranged from 3 to 17 years. The mean age of the children was 7.8 ± 3.8 years and at the onset of symptoms was 4.3 ± 2.9 years. The average duration between the onset of symptoms and diagnosis was 3.5 ± 3.8 years.
Individual description of the eosinophilic esophagitis cases according to gender, age at diagnosis, clinical complaint, age at the onset of symptoms, and clinical diagnosis.

The most common symptoms were abdominal pain in nine (82%) patients, regurgitation ≥2× per day for more than three weeks in five (45%) patients, difficulty in gaining weight in five (45%) patients, vomiting in five (45%) patients, dysphagia in four (36%) patients, and coughing in three (27%) patients. The patients of pre-school age at the onset of symptoms experienced the following main clinical manifestations: abdominal pain in five (45%) patients, regurgitation ≥2× per day for more than three weeks in four (36%) patients, and vomiting in three (27%) patients.
Specific IgE concentration for foods was assessed in five (45%) patients and was positive for α-lactalbumin and β-lactalbumin (Class I) in four (36%) patients.
The main clinical diagnoses before the diagnosis of EoE were gastroesophageal reflux disease in nine (82%) patients, food allergy in eight (73%) patients, and gastritis in six (55%) patients.
Endoscopic findings included normal mucosae in five (45%) patients, signs of mucosal thickening with longitudinal shearing in three (27%) patients (Fig. 1), erosive esophagitis in two (18%) patients, and a white patchy exudate in one (9%) patient (Table 2).

Esophageal mucosa showing signs of thickening, with longitudinal shearing (patient 2).

Esophageal mucosa esophageal after 8 weeks of treatment with fluticasone propionate (Patient 2).
Histopathological examination revealed that all patients in this series presented more than 30 (ie, ranging from 30 to 80) eosinophils per field (Fig. 3), which was higher than the diagnostic criterion of >15 eosinophils/high-power field.

Esophageal mucosa with basal layer hyperplasia, mild exocytosis of lymphocytes, and eosinophils marked with eosinophilic cluster formation (arrow). Hematoxylin and eosin (200×).
The treatment after the histopathological diagnosis of EoE included the use of a topical corticosteroid in ten (91%) patients and dietary restrictions in eight (73%) patients. Eight (73%) patients presented effective responses to treatment, which was characterized by the resolution of symptoms. Two (18%) patients reported persistent complaints of nausea. One patient (9%) reported persistent abdominal pain and dysphagia (Table 2). Although ten patients received topical corticosteroids for eight weeks, none reported complications such as bleeding or candidiasis.
Ten patients underwent endoscopic and histological reassessment two months after beginning treatment, which revealed a reduction in the number of eosinophils to ≤15 eosinophils per field and endoscopic resolution of the initial lesion. (Figure 2) (Table 2).
Individual description of the treatments, tests, and outcomes of the eosinophilic esophagitis cases.

Discussion
We examined the late diagnosis of eosinophilic esophagitis in 11 pediatric patients, taken from a larger group of 100, whose symptoms had been attributed to other diseases, such as food allergies, gastroesophageal reflux disease, and gastritis. These incorrect diagnoses had resulted in the adoption of inappropriate treatments and the persistence of symptoms, affecting the patients’ quality of life. Previous epidemiological studies of EoE and this case series show that pediatric cases are susceptible to non-timely diagnosis. An incidence of 1/10,000 has been reported, 7 and it is estimated that 6.8% of patients with esophagitis have EoE. 4
The sample analyzed was in accordance with the literature, which describes males as the most affected group at a ratio of 3:1 to 4:1; additionally, no association exists between EoE and racial or ethnic background. 8 There is evidence that EoE occurs in families and that most patients have a personal and/or family history of other allergic manifestations (eg, respiratory, cutaneous, and/or food allergies). 9
In the patients studied, the onset of symptoms occurred, on average, at the age of four years, with the diagnostic peak at age seven. This differs from ages of diagnoses in previous studies, which describe EoE as affecting more children of school age, frequently between 5 and 10 years, although there are case reports involving younger children. 10,11
In this group of patients, symptoms were frequently considered typical of gastroesophageal dysfunction (ie, abdominal pain, regurgitation, difficulty gaining weight, dysphagia, and vomiting), which most likely caused clinical suspicion and an initial diagnosis of diseases such as food allergies, gastroesophageal reflux disease, and gastritis.
The patients underwent empirical treatment based on the clinical diagnoses (priorto the UGE with biopsy) using medications such as H2 antihistamine, proton pump inhibitors, and gastric motility stimulators, but without a satisfactory outcome.
Increased serum total IgE and skin patch and positive RAST can be found in 40%–73% of patients,12,13 which is similar to the results observed in this study (45%). Peripheral eosinophilia and total IgE levels are informative parameters. 8
On average, patients were referred to undergo the first UGE with biopsy only three years after the onset of their symptoms and treatment attempts without satisfactory clinical responses (Table 2).14,15
In most publications, the time interval measured between the onset of symptoms and diagnosis was reportedly an average of 4.3 years, ranging between one and 13 years. 16 Although the elapsed time for diagnosis was on average lower than that described in literature, it is important to note that the disease was present in patients for 3 or 4 years before being diagnosed.
UGE is the only accurate diagnostic method for EoE. Despite descriptions of the specific aspects of endoscopy, greater than 34% of children with EoE have a normal esophagus. 17 In this study, 45% of endoscopies were normal. Although various manifestations have been reported for endoscopic study, the most characteristic manifestation is “corrugated esophagus” or “concentric rings of mucosa”, as well as longitudinal stenosis of the internal diameter. White patchy exudates with the loss of the normal vascular patterns of the esophagus may indicate areas of eosinophilic infiltration. Vertical lines in the esophagus and friable mucosa, called “crepe paper mucosa”, are also suggestive of EoE. 12
Typically, the esophageal mucosa contains no eosinophils; therefore, the presence of more than 15 eosinophils per high-power field, which was observed in this sample, is considered a marker of EoE. In reflux esophagitis, the usual number of eosinophils is approximately one (or, at most, ten eosinophils) per high-power field.18,19 Cases with scores between 10 and 15 are often considered a questionable diagnosis. 18
There is still no consensus on the ideal treatment for patients with EoE. Treatment should be individualized and preferably based on the clinical context. Success has been reported in treating allergic EoE with oral fluticasone propionate administered by metered-dose inhalers. 20 Oral viscous budesonide has also been shown to be effective; however, esophageal candidiasis has been described in approximately 15% of these patients.20,21
There are no objective criteria for assessing treatment response; subjective clinical monitoring and/or endoscopy combined with histology have been used for this assessment. 12 The clinical symptoms and eosinophil counts after treatment are considered to be markers of improvement.
Patients in our sample received topical corticosteroids for a short period of two months after the diagnosis of EoE. However, most of the subjects exhibited a favorable clinical response after starting the recommended treatment with swallowed inhaled steroids used either alone or in association with the exclusion of the responsible allergen (if detected).
Despite the debate regarding whether to treat histologically confirmed EoE in the absence of symptoms, treatment is recommended given the known long-term risks of remodeling, fibrosis, potential esophageal strictures, and lymphoproliferative diseases. 20
It has been suggested the use of an algorithm for investigation of pediatric patients with esophageal symptoms in order to provide pediatricians with the information required for clinical suspicion and treatment (Fig. 4).
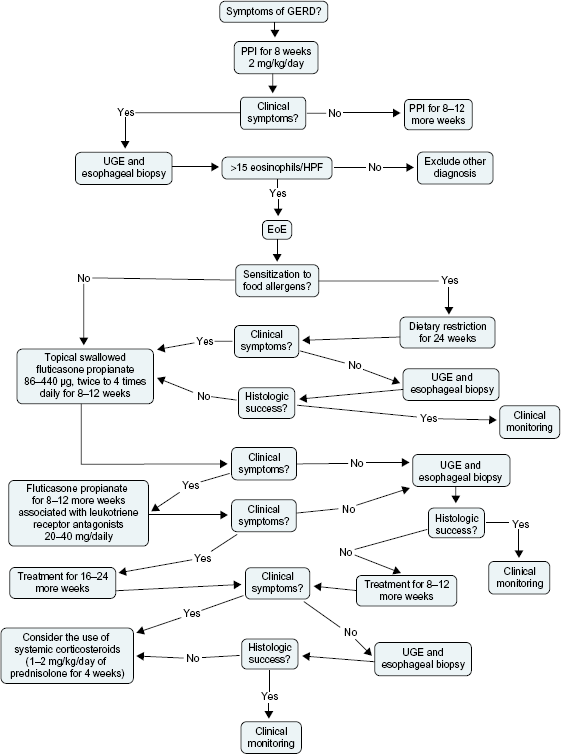
Algorithm approach to pediatric patients with suspected EoE.
Conclusions
The late diagnosis of eosinophilic esophagitis in 11 pediatric patients whose symptoms had been attributed to other diseases, such as food allergies, gastroesophageal reflux disease, and gastritis, resulted in the adoption of inappropriate treatments and the persistence of symptoms that affected the patients’ quality of life.
Author Contributions
Wrote the first draft of the manuscript: MICP. Contributed to the writing of the manuscript: MICP, CABS, LPGC. Jointly developed the structure and arguments for the paper: MICP, RSH, LHAM, MCF, CABS, LPGC. Made critical revisions and approved final version: MICP, RSH, LHAM, MCF, CABS, LPGC. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.