
Abstract
Person-centered care is presently the standard healthcare model, which emphases shared clinical decision-making, patient autonomy and empowerment. However, many aspects of the modern-day clinical practice such as the increased reliance on medical technologies, artificial intelligence, and teleconsultation have significantly altered the quality of patient-physician communications. Moreover, many countries are facing an aging population with longer life expectancies but increasingly complex medical comorbidities, which, coupled with medical subspecialization and competing health systems, often lead to fragmentation of clinical care. In this article, I discuss what it truly means for a clinician to know a patient, which is, in fact, a highly intricate skill that is necessary to meet the high bar of person-centered care. I suggest that this can be achieved through the implementation of a holistic biopsychosocial model of clinical consultation at the physician level and fostering coordinated and continuity of care at the health systems level.
Keywords
Introduction
Person-centred care has now become the standard model of healthcare delivery as the medical field shifted from a traditionally more paternalistic clinical approach to one that emphasises patient autonomy, empowerment and shared decision-making. Yet, the rapid integration of medical technologies and artificial intelligence in clinical practice have led to increased automation of clinical processes, virtual/off-site clinical interactions and significantly altered quality of patient–physician communications.1,2 Moreover, with increasing medical subspecialisation, competing health systems and an ageing population with rising burden of medical comorbidities, much of our present medical care has become fragmented with adverse clinical effects on the patients. In this article, I sought to review what it truly means for a clinician to know a patient, which is actually a highly intricate skill that is needed to meet the standards of person-centred care and requires dedicated commitment to being intentional in information gathering and optimising physician–patient interactions. In addition, I suggest practical strategies at both the physician and health systems level to optimise patient–physician relationships/interactions and foster holistic, coordinated and person-centred care.
What does it mean to know one’s patient?
To be clear, knowing a patient is not the same as knowing about a patient – a physician can know that a patient has a primary diagnosis of diabetic ketoacidosis requiring intravenous insulin therapy, without recognising that the patient has a history of poorly controlled diabetes mellitus with medication non-adherence and suboptimal clinical follow-up, and has personal circumstances, psychosocial and cultural contexts that predispose to this phenomenon. For instance, the patient may have poor health literacy and is working long hours with financial difficulties – all of which can contribute to inability to comply with treatment regimen and clinical follow-up, and these may be further related to underlying income and social inequalities. Moreover, the patient may also have a fear of having to self-administer insulin injections 3 or a misconception that blood glucose monitoring and insulin jabs are not permitted during the religious fasting period. 4 Therefore, a physician who truly ‘knows’ his/her patient must be able to have an accurate understanding of patient’s active clinical issues and concerns, previous medical/treatment history, psychosocial circumstances, cognitive beliefs/barriers and sociocultural determinants of health. Such intimate knowledge would then form the basis for person-centred care that tackles not only medical issues at a superficial level but also addresses underlying predispositions and co-existing concerns.
Adopting a biopsychosocial clinical consultation model at the physician level
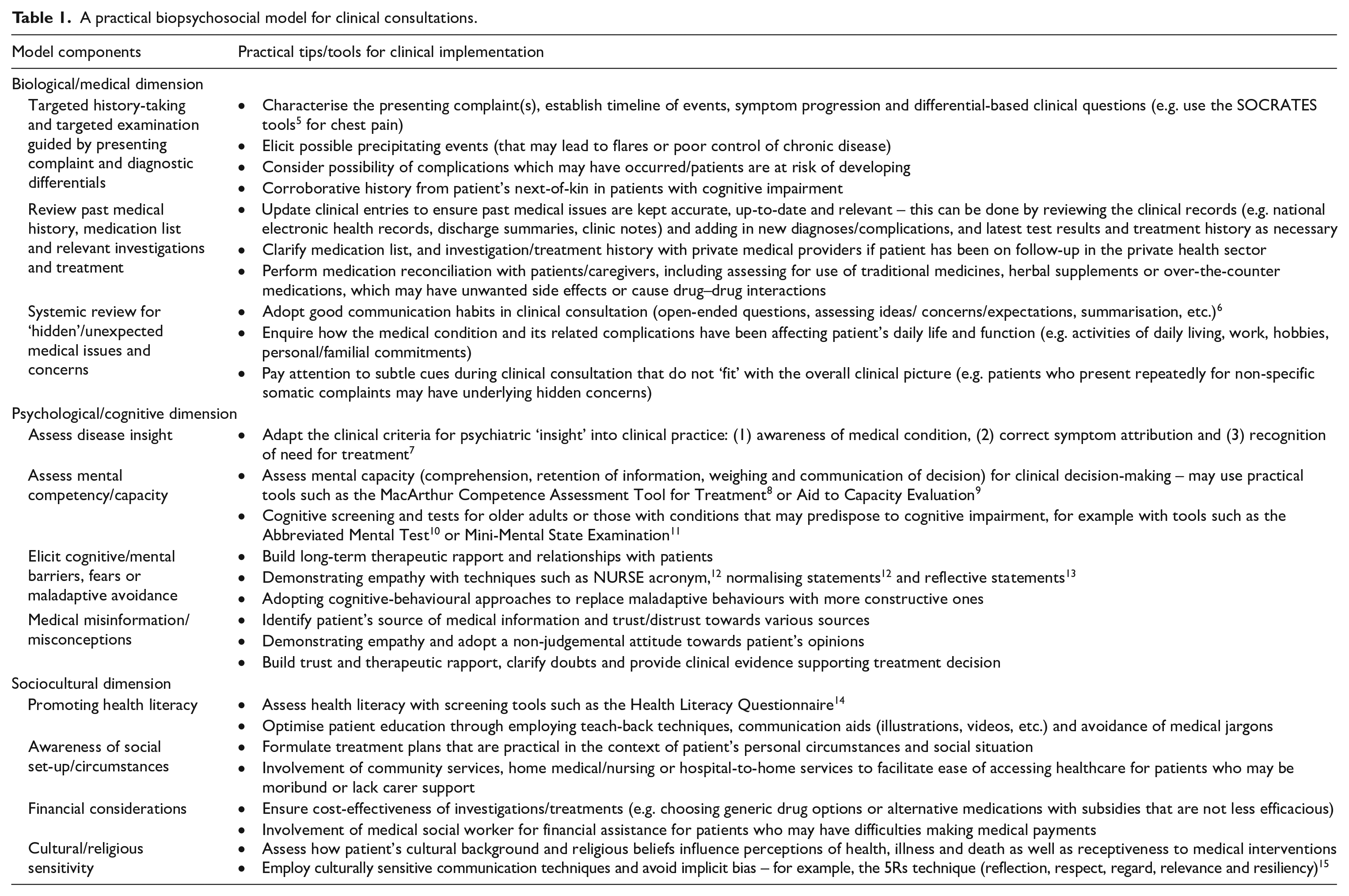
I herein suggest a biopsychosocial model of clinical consultations (Table 1) that can help to optimise patient–physician interactions to facilitate holistic understanding of patient’s medical and non-medical issues, and other relevant sociocultural and psychological determinants of health in a personalised manner.
A practical biopsychosocial model for clinical consultations.
Biological/medical aspect of clinical consultation
The medical aspect of a clinical consultation can be conceived in three main components: (1) characterising and assessing the presenting complaint(s), (2) reviewing past medical records and (3) systemic review to ensure other pertinent clinical problems/concerns are not missed. In practice, a patient-centred history-taking would involve not only detailed clerking of patient’s presenting complaints to arrive at relevant differential diagnoses, identifying of underlying aetiologies/precipitants and relevant complications, but also adequate exploration of patient’s ideas, concerns and expectations and how the disease is currently affecting their daily functioning. 16 Likewise, clinical examination is not limited to targeted evaluation of signs/features that are relevant to the presenting complaint, but should also involve paying attention to subtle clinical cues and patient mannerisms that may reveal other pertinent issues that should be addressed. For example, a patient who comes in repeatedly for clinical consultation for ‘flu-like symptoms’ but is oddly wearing sunglasses in an indoor environment might actually be hiding periorbital bruises and injuries inflicted by spousal abuse. In recent years, the use of electronic medical records (EMRs) has been widely adopted to assist in the documentation, storage and sharing of pertinent patient clinical information between health providers at different centres, which improves clinical efficiency, avoid medical errors and unnecessary duplication of investigations. 17 However, there are pitfalls to medical technology in clinical practice that physicians should be privy to and actively seek to avoid. For example, copy-pasting practices in the EMR can lead to clinical documentations containing significant inaccuracies and outdated information, 18 and result in information overload (with abundance of clinically irrelevant details with poor data display) that may predispose to medical errors. 19 Therefore, clinicians have to be conscientious in upkeeping the veracity and relevance of clinical documentations through verifying original entries and investigation findings, updating on recent clinical events that have taken place in-between follow-ups, and providing good summaries of relevant medical issues without unnecessary/irrelevant clinical details.
Psychological aspect of clinical consultation
At the psychological level, it is important to assess patient’s health perceptions, insight into medical condition and identify mental barriers to health-seeking behaviour. For instance, some patients with significant cognitive impairment, comorbid psychiatric conditions or fixed, preconceived notions may have impaired insight into their medical condition, affecting their perceived need for treatment. To assess patients’ disease insight, we must consider if they have awareness of illness, correct attribution of clinical manifestations to underlying illness and recognising the need for treatment/intervention. 7 Sometimes, patients may also develop specific fears or maladaptive avoidance in response to certain medical diagnoses, leading to suboptimal adherence to medical treatment and follow-ups. In such instances, cognitive-behavioural techniques to re-frame patient’s thought patterns and replace maladaptive behaviours with more constructive responses will be important. Finally, the spread of medical misinformation has becoming increasingly prevalent in the present age perpetuated by social media and political agendas, 20 where patients can be easily susceptible to falsehoods about vaccines, lifestyle habits, communicable and non-communicable diseases and medical treatments. 21 To help these patients, physicians should identify patient’s source(s) of medical information, explore patient’s views in a non-judgemental manner and adopt communication techniques of persuasion to help patient become more receptive to evidence-guided medical options.
Sociocultural aspect of clinical consultation
At the sociocultural level, it is increasingly recognised that overall health and health disparities in patient populations are often driven by non-medical, social determinants of health. 22 In practice, patients’ health behaviours may be affected by their health literacy, social/familial set-up, financial situation, cultural and religious practices and other unique circumstances. Till date, inadequate health literacy remains a prevalent problem worldwide, affecting one-fifth to one-third of hospitalised patient populations23,24 and disproportionately affecting underprivileged groups in societies. 23 Patients with poor health literacy, which may be associated with low education levels, 24 may not recognise the clinical implications of their condition and need for treatment, or find it difficult to grasp complex treatment regimens. In such cases, patient education can be optimised through techniques such as ‘teach-back’, 25 with appropriate communication adjuncts/aids and avoidance of medical jargons. In other cases, patient’s social circumstances may form a huge barrier to treatment adherence. For example, it may be impractical for a young diabetic patient who works long hours as a delivery personnel, living paycheck-to-paycheck and being the sole breadwinner to a family with young children, to adhere to a healthy diet, regular exercise regimen, perform regular blood glucose monitoring or take up expensive medication options like sodium-glucose cotransporter-2 inhibitors or glucagon-like peptide 1 receptor agonists. Therefore, medical treatment options offered to patients must be practical and feasible given their social circumstances and financial situation. Finally, health beliefs and practices can be significantly influenced by one’s cultural background and religious beliefs. For example, Asian cultures often place great value on collectivism, filial piety and family-centric health decision-making at the expense of individual autonomy, leading to heavy familial involvement in patient’s healthcare decision-making including end-of-life/extent of care decisions.26,27 In addition, religious beliefs may be associated with vaccine hesitancy due to concerns over the permissibility of receiving specific vaccines/components. 28 Physicians who consciously practice cultural sensitivity in their clinical interactions will be able to demonstrate respect for patient’s beliefs, show understanding towards patient’s concerns and address misconceptions.
Coordinated and continuity of care at health systems level
At the broader level, healthcare systems need to strike a healthy balance between providing essential, subspecialised clinical care for complex health conditions while avoiding fragmentation of care that results in lack of clinical continuity. Previous studies have shown that inpatient care fragmentation is common in those with recurrent hospitalisations and also in patients with lower income and inadequate health insurance who are living in population-dense regions. 29 With fragmented medical care, the patients’ physicians are unlikely to ‘know’ them well, due to discontinuity in care, incomplete medical records and the lack of time to build relationships and therapeutic rapport necessary to understand patient’s circumstances, concerns and expectations. In Singapore, we have implemented various strategies to improve continuity and coordination of patient care that includes forging of stronger partnerships among healthcare providers, 30 establishing common care interfaces and EMRs, 30 and strengthening of primary care systems to provide dedicated general practitioner care for patients. 31 Ultimately, health systems in populated cities would benefit from both a shift in the care model from hospital to community-based care 32 as well as training of specialist-generalists with adequate breadth and depth of clinical expertise to provide integrated, consolidated care for common conditions in the population. 33
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.