
Abstract
Hypothyroidism is an endocrine disorder which occurs due to a deficiency of thyroid hormones. Hoffmann’s syndrome is a rare complication of hypothyroidism – presenting as hypothyroid myopathy. We describe the case of a 20-year-old lactating female, known to have hypothyroidism (diagnosed during her pregnancy and having discontinued treatment following delivery), presenting with complaints of pain, swelling of bilateral calf muscles with cramps in bilateral lower limbs. Symptoms of muscle pseudohypertrophy with muscle stiffness are relatively rare in subclinical hypothyroidism and it is important to identify and diagnose this rare condition, and initiate appropriate treatment.
Keywords
Introduction
The symptoms of hypothyroidism vary in severity and can range from subclinical to potentially fatal conditions. Among adults, while clinical presentations vary, the most frequently reported symptoms include fatigue, sluggishness, intolerance to cold temperatures, weight gain, constipation, changes in voice, hair loss and dry skin. 1
Overt hypothyroidism is a condition where levels of thyroid-stimulating hormone (TSH) in the blood are higher than the normal range (>4.2 µIU/ml), while the levels of free thyroxine (FT4) are lower than the normal range (<5.5 µg/dl). Subclinical hypothyroidism is considered an early stage of thyroid dysfunction – characterised by TSH levels above the normal range, while FT4 levels remain within the normal range.
Muscular symptoms as the primary or sole indication of hypothyroidism are frequently overlooked, creating challenges in distinguishing it from other potential causes of myopathy.2,3 Hypothyroidism may have varied muscular symptoms, including rhabdomyolysis, Hoffmann’s syndrome, and acute compartment syndrome.
In this case report, we describe a case of Hoffmann’s syndrome, which is a rare muscular disorder characterised by proximal muscle weakness and pseudohypertrophy of muscles in individuals with hypothyroidism.
Case
A 20-year-old lactating female patient presented with complaints of swelling of calf muscles, stiffness, pain and cramps in bilateral lower limbs for 1 day. The patient did not complain of weakness of limbs, tingling/numbness, trauma to the limbs or fever in the recent past. She was diagnosed with hypothyroidism during her pregnancy, the details of which were not available, and treated with thyroxine which was discontinued after her delivery 10 months prior to presentation. The patient had no other symptoms suggestive of hypothyroidism at presentation.
On examination, the patient had a pulse rate of 98 bpm, and a blood pressure of 120/80 mmHg, with an apparent hypertrophy of calf muscles (bilateral gastrocnemius) (Figure 1).

Pseudohypertrophy of calf muscles can be seen – as marked by white ellipses.
The hypertrophied muscles were tender, with no local rise of temperature and all deep tendon reflexes were elicitable. There was no proximal or distal muscle weakness in both lower limbs. Plantar reflex was flexor bilaterally and there was no sensory involvement. She was able to walk, though with a slight limp due to the cramping pain in her calf muscles. No tongue hypertrophy was seen. Other systems examination was unremarkable.
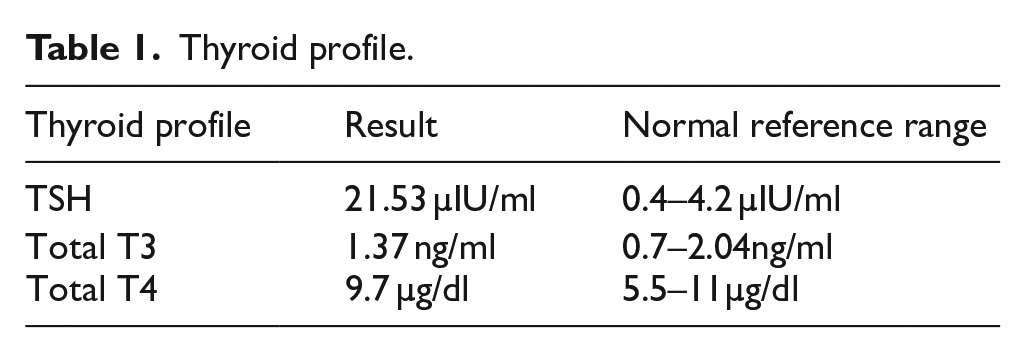
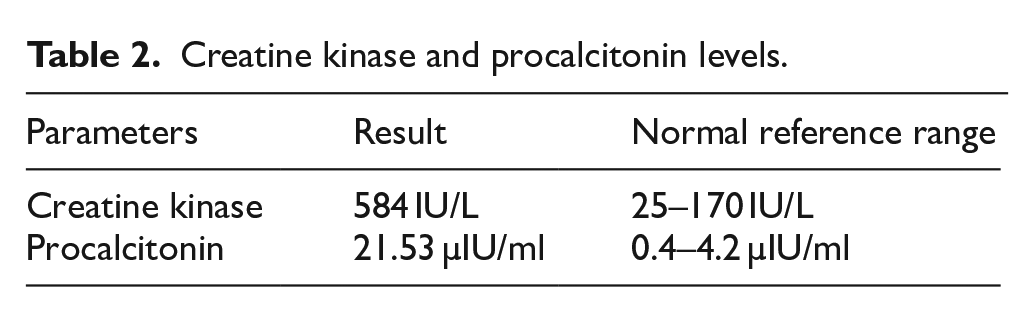
Investigations revealed elevated TSH levels with normal Total T3 and T4 levels, suggestive of subclinical hypothyroidism. Procalcitonin levels were also raised. Creatine kinase was found to be elevated, suggestive of muscle damage (Tables 1 and 2).
Thyroid profile.
Creatine kinase and procalcitonin levels.
Complete haemogram, serum electrolytes, urine routine, liver function tests (LFT), serum calcium, magnesium, phosphorus and vitamin D levels were all within normal limits. Random Blood Sugar was normal. No abnormalities were noted on electrocardiogram or echocardiogram. The patient developed chills on the third day after admission and complained of bifrontal headache with frontal sinus tenderness, but no fever. X-ray of the paranasal sinuses was normal. At this stage, deep vein thrombosis and pyomyositis were considered as red flag differential diagnoses and ruled out.
Bilateral lower limb venous Doppler study showed mildly bulky and heteroechoic right calf muscles without any evidence of deep vein thrombosis in both lower limbs. MRI revealed bulky calf muscles with no intramuscular collection or subcutaneous edema (Figure 2). Anti-thyroid peroxidase (anti-TPO) antibodies were also ordered.
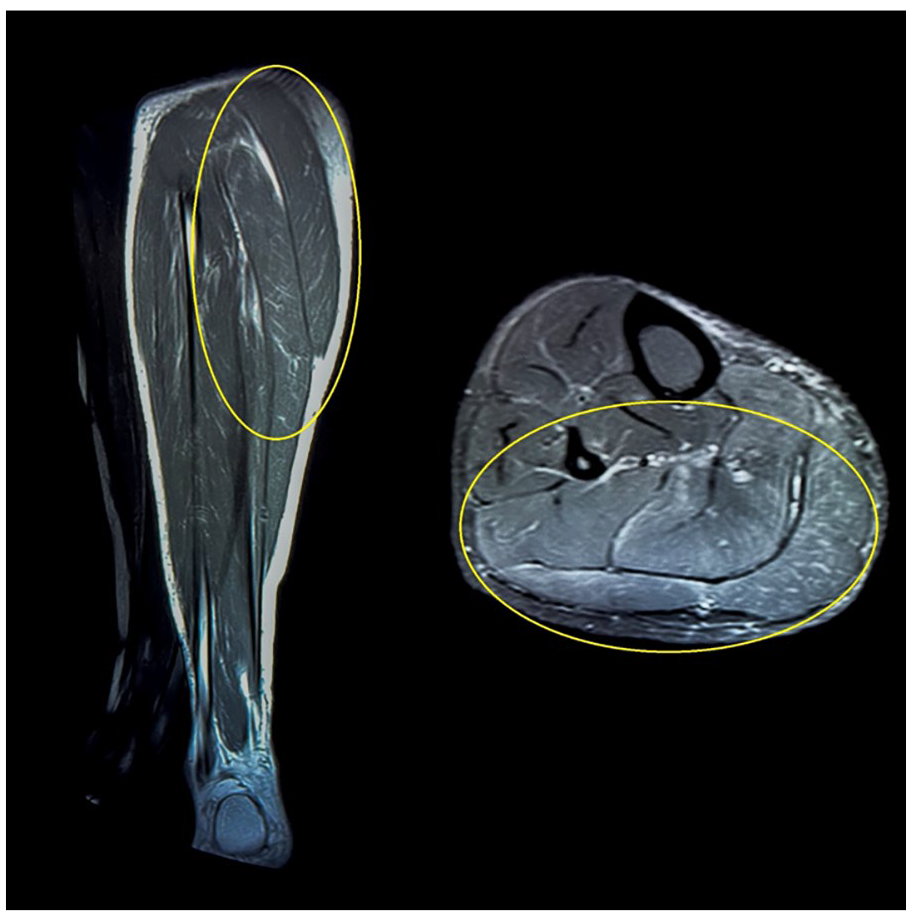
MRI images in coronal and axial sections showing bulky, hypertrophic calf muscles marked with a yellow ellipse.
The patient was diagnosed with subclinical hypothyroidism with hypothyroid myopathy – Hoffmann’s syndrome, and was started on Thyroxine 50 µg OD, along with analgesics, and empirical antibiotics (in view of elevated procalcitonin and clinical suspicion of pyomyositis). EMG-nerve conduction study and muscle biopsy were not done as the patient refused any further investigations. She noticed improvement in cramps and calf stiffness from the fourth day onwards and was able to walk normally with very minimal pain at the time of discharge. Anti-TPO Ab report came as positive – 86.80 (0–34 IU/ml).
Discussion
We have described the case of a patient without overt hypothyroidism who developed hypothyroid myopathy (Hoffmann’s syndrome) despite having only subclinical hypothyroidism.
Hypothyroidism is a common endocrine disorder that affects millions of people worldwide, including in India. It is caused by an underactive thyroid gland, which produces too little thyroid hormone. This condition is more common in women than men and can occur at any age. The prevalence of hypothyroidism in India is estimated to be around 10.95%. 1
Inadequate levels of thyroxine result in decreased mitochondrial capacity for oxidative processes, abnormal glycogenolysis, and cellular insulin resistance. This, in turn, precipitates the specific degeneration of type 2 muscle fibres (known as fast-twitch fibres) owing to their reliance on glycolysis for energy, which results in the observed clinical manifestation of slowed muscle contractions in individuals with hypothyroidism. As a compensatory response, muscle pseudohypertrophy occurs, postulated to be incited by the accumulation of glycosaminoglycans within the muscle tissue, 4 with the gastrocnemius muscle being the most frequent site of involvement.
Proximal symmetrical muscle weakness, muscles stiffness and cramping, delayed reflexes and myoedema represent the various neuromuscular manifestations of hypothyroidism. Predominantly, weakness serves as the prevailing clinical presentation, followed by occurrences of cramps.2,5,6 In acute presentations, hypothyroid myopathy may even culminate in rhabdomyolysis. 3
Muscular disturbances, typified by pain on muscular exertion, may occur due to slow or reduced protein turnover and/or an impaired carbohydrate metabolism. 7 These myopathic changes in hypothyroidism arise due to alterations in muscle fibre composition, transitioning from fast-twitch type 2 fibres to slow-twitch type 1 fibres. Additionally, there is an accumulation of glycosaminoglycans, impaired contractility of actin-myosin units, diminished activity of myosin ATPase, and attenuated ATP turnover within skeletal muscle tissue.2,8
Impaired calcium sequestration by the sarcoplasmic reticulum is responsible for the delayed relaxation of deep tendon reflexes observed in hypothyroid myopathy.7,9 This impaired sequestration prolongs the duration of muscle twitches. Mounding of the muscle (myoedema), which occurs as a response to pressure or light percussion, is one of the classical signs of hypothyroid myopathy. 10 This hypertrophy can be ascribed to an increase in both connective tissue and muscle fibres. Additionally, patients with thyroid dysfunction experience a reduction in muscle carnitine levels, which contributes to the manifestation of myopathic symptoms.
Elevated procalcitonin (PCT) levels in autoimmune thyroid disease may stem from the release of PCT into the bloodstream, a consequence of the destruction of PCT-producing tissues (chiefly the parafollicular C cells of the thyroid gland). Another possible explanation could be an increased signalling of the CALC-1 gene, leading to an increase in its expression, and hence to the increase in production of PCT-calcitonin via cytokines. Nevertheless, the signal responsible for the increased expression of the CALC-1 gene remains unknown. 11
Calf muscle hypertrophy, accompanied by muscle weakness, may be attributed to a spectrum of underlying aetiologies, including Duchenne and Becker muscular dystrophies, focal myositis, sarcoid granulomas, and the deposition of amyloid in muscles.4,6 Although patients with hypothyroidism frequently exhibit muscular symptoms, such as myalgia, weakness, stiffness, cramps, and fatigue (in approximately 30%–80% of cases), the occurrence of muscular pseudohypertrophy and stiffness is comparatively rare, affecting less than 10% of individuals with hypothyroidism. 4 Muscle biopsies are often normal, revealing no abnormalities. 12
Hoffmann’s syndrome is a distinct and uncommon type of hypothyroid myopathy observed in adults, characterised by weakness in the proximal muscles and the development of pseudohypertrophy in affected muscles. 4 As previously elucidated, muscle pseudohypertrophy with stiffness and pain is relatively rare. 4 The presentation of this patient was atypical, with pain and swelling of the calf muscles in the absence of classical attributes of Hoffmann’s syndrome (muscle weakness and myoedema). We are reporting this case for the rarity of this entity in subclinical hypothyroidism. It is also worth noting that if hypothyroid myopathy were to present in children with congenital iodine deficiency syndrome, it would be referred to as Kocher-Debré-Sémélaigne syndrome. 13
Conclusion
Hoffmann’s syndrome is a rare complication that can arise in patients with hypothyroidism, very rare in subclinical hypothyroidism. Clinicians must be aware of this entity and rule out other red-flag conditions such as DVT and polymyositis before arriving at the diagnosis, to ensure appropriate management and targeted interventions. Screening and regular follow-ups should be considered, as the prompt treatment of hypothyroidism is important to prevent further complications like rhabdomyolysis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.