
Abstract
Background:
In general, adults with congenital heart disease have reduced exercise capacity and many do not reach the recommended level of physical activity. A physically active lifestyle is essential to maintain health and to counteract acquired cardiovascular disease, therefore enablers and barriers for being physically active are important to identify.
Aim:
To describe what adults with complex congenital heart diseases consider as physical activity, and what they experience as enablers and barriers for being physically active.
Methods:
A qualitative study using semi-structured interviews in which 14 adults with complex congenital heart disease (seven women) participated. The interviews were analysed using qualitative content analysis.
Results:
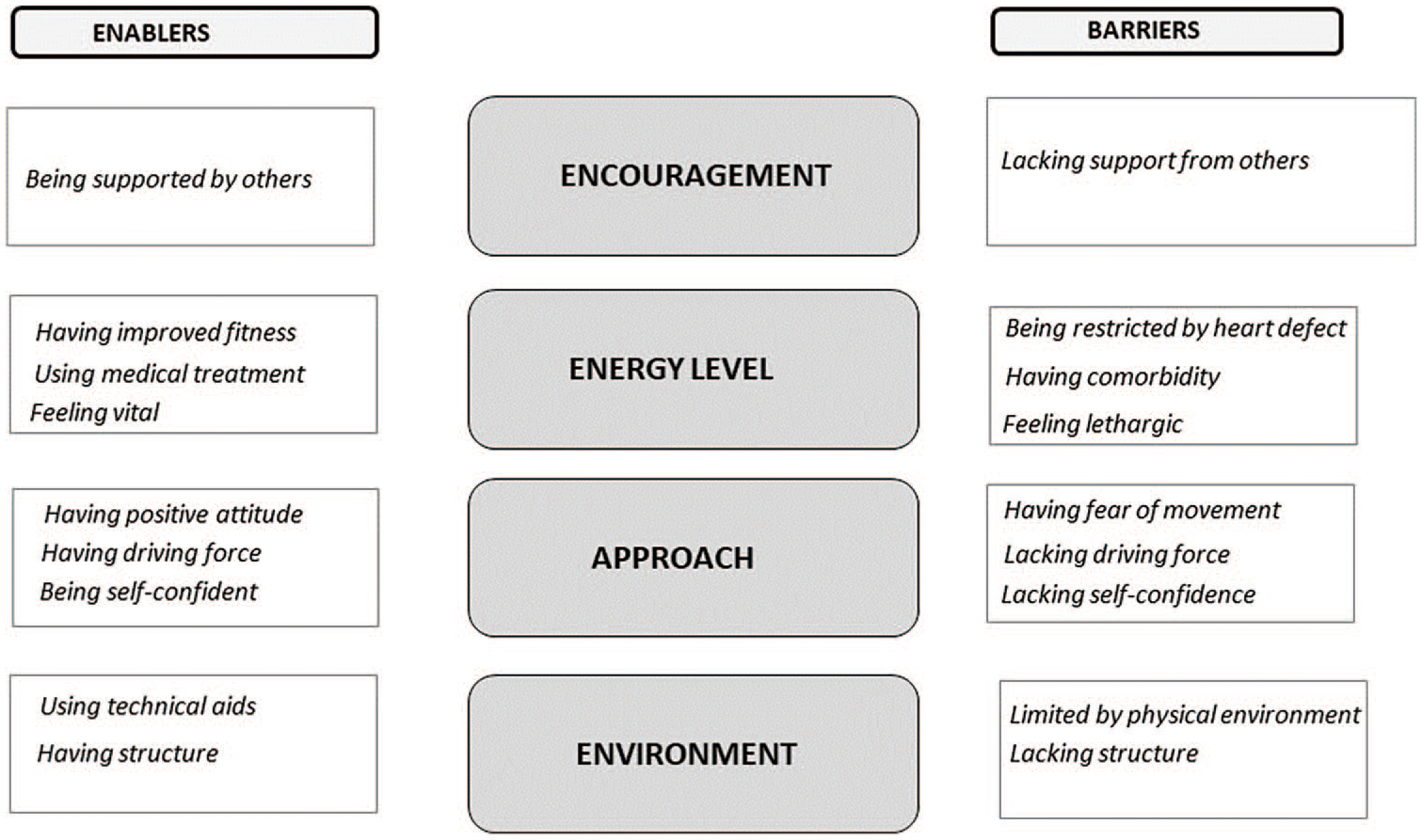
The analysis revealed four categories considered enablers and barriers – encouragement, energy level, approach and environment. The following is exemplified by the category encouragement as an enabler: if one had experienced support and encouragement to be physically active as a child, they were more positive to be physically active as an adult. In contrast, as a barrier, if the child lacked support and encouragement from others, they had never had the opportunity to learn to be physically active.
Conclusion:
It is important for adults with congenital heart disease to have the opportunity to identify barriers and enablers for being physically active. They need knowledge about their own exercise capacity and need to feel safe that physical activity is not harmful. This knowledge can be used by healthcare professionals to promote, support and eliminate misconceptions about physical activity. Barriers can potentially be transformed into enablers through increased knowledge about attitudes and prerequisites.
Introduction
Adults with complex congenital heart disease (CHD) are a growing population due to improved surgical techniques and specialized medical care.1,2 However, surgical treatment is rarely curative, and as a consequence of the improved survival, long-term complications and comorbidity increase.1,3 It is reported that already at a relatively young age, this population has the same or even a higher risk as the general population to develop acquired cardiovascular diseases.4,5 Being physically active is important to prevent future acquired cardiovascular disease, and many adults with CHD do not reach the recommended level for physical activity. 6 The present study contributes to current knowledge about experienced enablers and barriers for physical activity among adults with CHD.
Background
Physical activity is a part of a healthy lifestyle and it decreases the risk of acquired cardiovascular diseases.7,8 The general definition of physical activity, also used in the present study, is all body movements that result in increased energy consumption. 9 Physical activity can be integrated in everyday life at home, school or work. Physical exercise is defined as planned and structured physical activity intended to maintain or improve fitness or strength. 9 According to the European Society of Cardiology guidelines (2010), adults with CHD are encouraged to be physically active, and exercise training should be individually prescribed. 10 Practical recommendations have been developed to support healthcare providers for advice in this setting. 11
Previous studies focusing on physiological limitations show that adults with CHD have reduced aerobic exercise capacity and impaired muscle endurance capacity.12–14 Age and muscle endurance capacity are associated with exercise self-efficacy. 15 In addition, age and patient-reported outcomes have been shown to be associated with physical activity both in a national context 16 as well as in an international context. 17 However, knowledge is scarce of how adults with CHD experience physical activity. In a recent mixed-methods study on young adults, behaviours and perceptions when being physically active were described. 18 In that study, influence from the family in childhood was important for participants to adopt a positive perception of physical activity that remained in young adulthood. 18 A previous study showed how adults with complex CHD describe themselves in relation to physical activity. 19 Descriptions were over a wide range from being very physically active to not being active at all. 19 Nevertheless, knowledge is lacking about what adults with complex CHD experience as enablers and barriers to being physically active. The aim of the present study was to describe what adults with CHD consider as physical activity, and what they experience as enablers and barriers for physical activity.
Methods
Design
An inductive and descriptive design with semistructured interviews was used in this study. Fourteen adults with complex CHD 1 participated and the interviews were analysed using qualitative content analysis. 20 As the intention was to describe participants’ experiences of enablers and barriers towards physical activity, an inductive and manifest approach inspired by Graneheim and co-workers 21 was used to answer the question ‘what’. An inductive approach was applied by searching for patterns in the data based on similarities and differences and moving from empirical experiences to a theoretical understanding. 21
Data collection
Twenty-four adults with complex CHD, 1 semi-consecutively selected from the clinic waiting list, were asked to participate in connection with a regular follow-up clinic visit. Inclusion criteria were a diagnosis of complex CHD, age greater than18 years and the ability to speak and understand Swedish. Fourteen adults aged 19–68 years (median 31.5 years) accepted (Table 1). Interviews were conducted during May 2016 to January 2017 at a specialised centre for adults with CHD in northern Sweden.
Demographic and clinical characteristics of the study population.
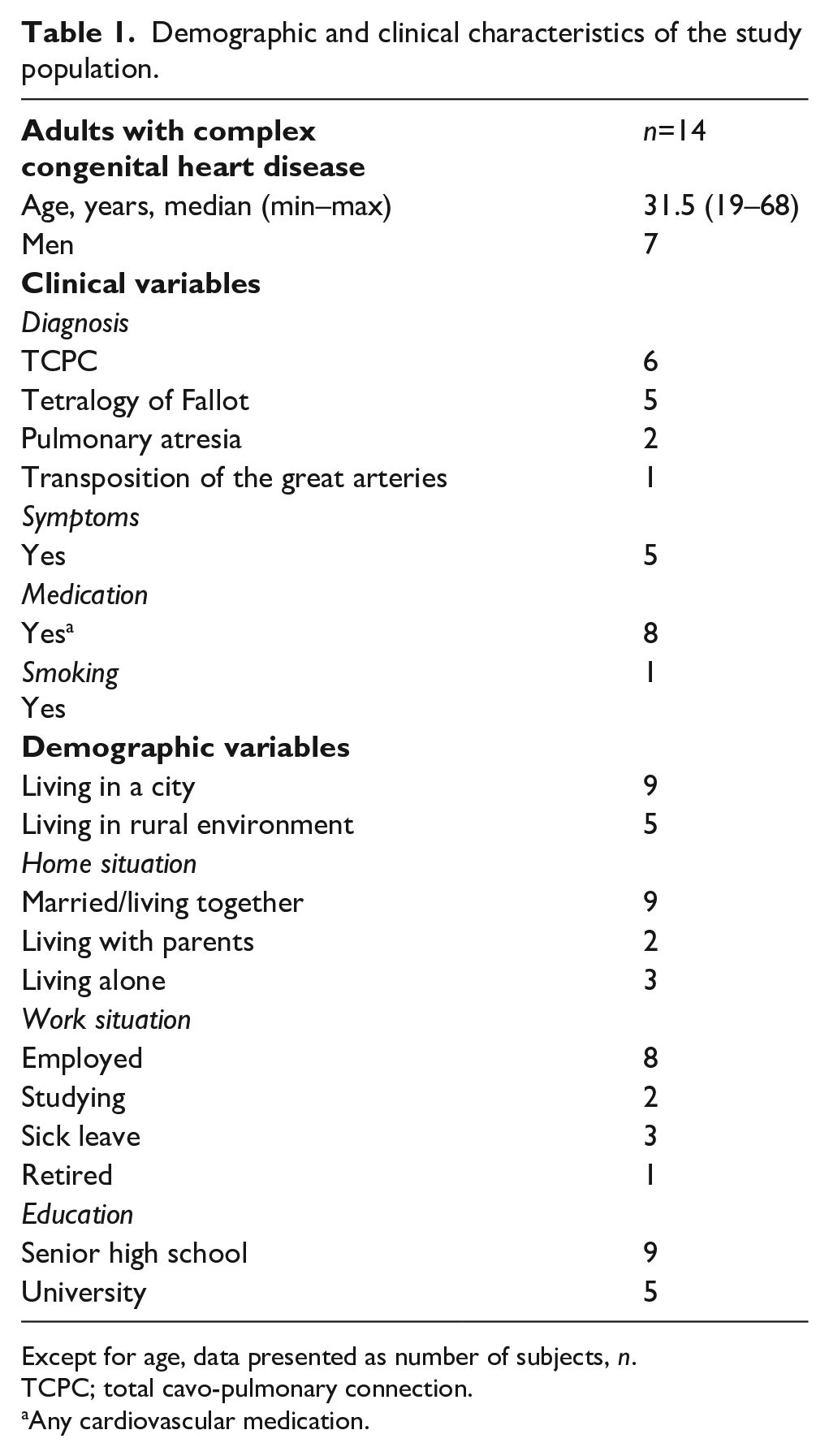
Except for age, data presented as number of subjects, n.
TCPC; total cavo-pulmonary connection.
Any cardiovascular medication.
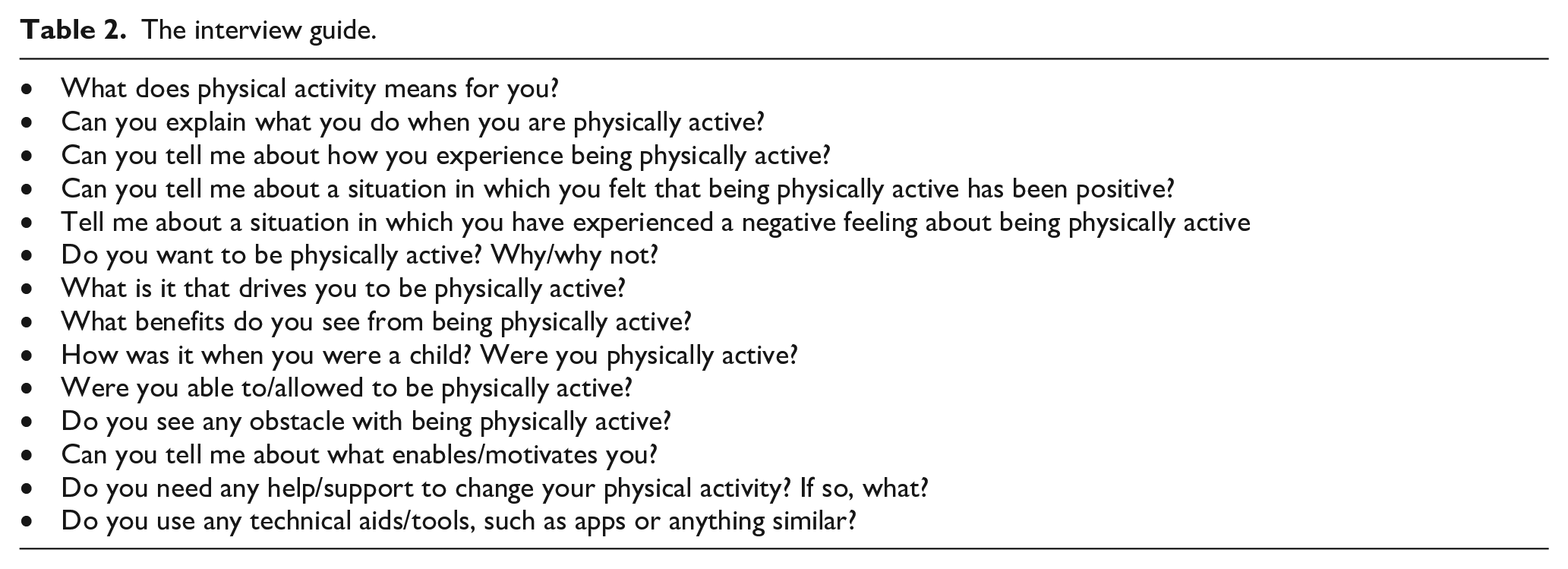
The individual interviews followed a semi-structured interview guide that was developed from the authors’ clinical experiences, previous research, previous findings in the beginning of a PhD project and through discussions in the research team. The semistructured interviews were conducted by AB (first author) in a private room within the clinic, and after patients had visited with their cardiologist. All interviews started with the open question ‘Can you tell me what physical activity means to you’? (Table 2). Follow-up questions were asked for clarification and further exploration of the aspects of enablers or barriers to physical activity. The interviews lasted 20–45 minutes (median 32 minutes) and were digitally recorded and transcribed verbatim by AB.
The interview guide.
Data analysis
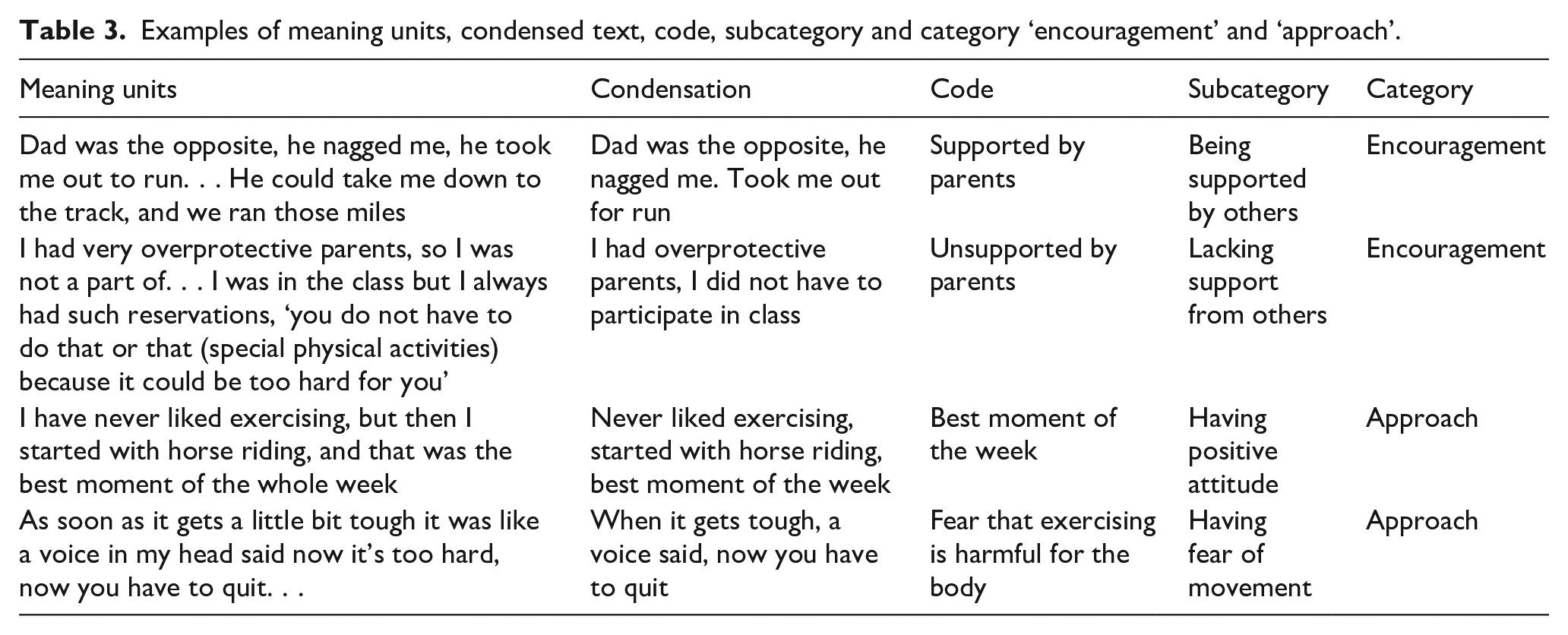
Initially, the first author read the text repeatedly to obtain an overview. Two authors performed the open and selective coding of the text, and all co-authors reflected on and discussed the steps in the analysis. Furthermore, the codes were compared and sorted based on similarities or dissimilarities and then followed grouped in subcategories and categories (Table 3). Even if the description of the analysis process seems linear, there has been movement back and forth between the whole and the part of the text including subcategories and categories. 19
Examples of meaning units, condensed text, code, subcategory and category ‘encouragement’ and ‘approach’.
Ethical considerations
The participants received written and oral information about the study, and all gave written informed consent for participation. The digital recordings were anonymised. A code list identifying the participants was created and stored separately from the recordings. The study was approved by the ethics review board (no. 2016-78-32M) in Umeå, Sweden, and it conformed to the principles outlined in the Declaration of Helsinki. 22
Findings
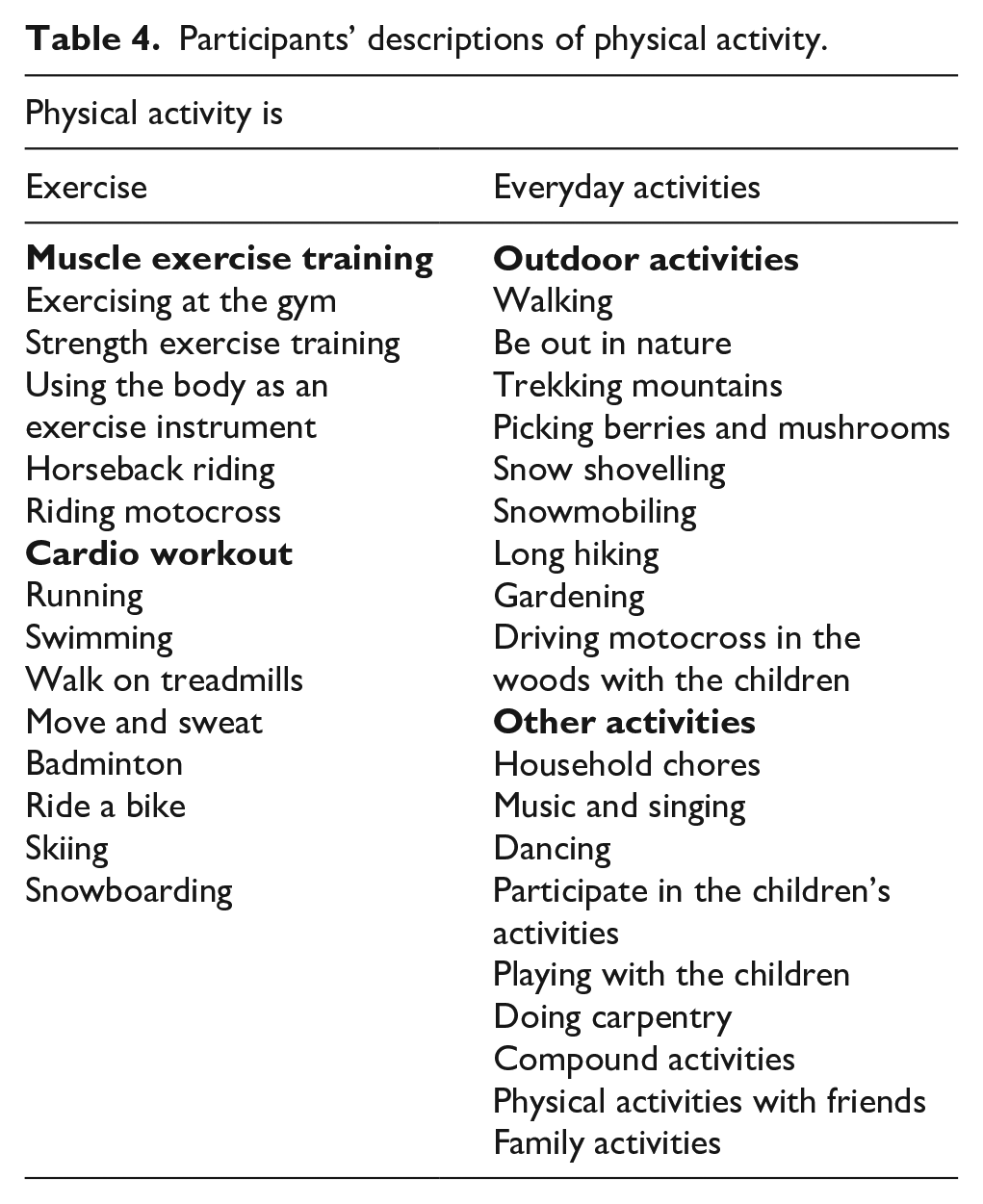
A description of what participants considered as physical activity and what they did when they were physically active is shown in Table 4.
Participants’ descriptions of physical activity.
The analysis revealed four categories – encouragement, energy level, approach and environment (Figure 1). Each category included two perspectives, each phenomenon described as enablers has a negative contrast that was described as a barrier.
Categories and subcategories.
Encouragement
The category encouragement included both to be encouraged and the absence of encouragement. One subcategory, being supported by others, was described as an enabler and one subcategory, lacking support by others, as a barrier.
Being supported by others was an enabler that included both being encouraged and not being restricted. To be active as a child seemed to enable the opportunity to be physically active as an adult. In childhood, participants had engaged in sports activities and played like everyone else. There were no restrictions from their cardiologist or parents. Furthermore, they participated in family activities and other activities just like their healthy siblings.
My parents took me to football every week and so, and there was no one who restricted me. . . there was no thought that you would not be able to make it, so it was just as usual. . . P8
The participants were supported and encouraged by parents, teachers or peers, which thereby created an opportunity for physical activity. They felt strengthened by the fact that others believed in them, and that they felt supported in that they actually managed to be physically active even if sometimes feeling physically or mentally constrained.
I had a good teacher. . . she sat down with me and then she said, ‘I know that you do not have as much vigour as the others, but at least you try; take that with you in life!’. . . That has been with me a little as a mantra. It meant so much, at least then! P13
In contrast to having support and encouragement, participants were lacking support from others in childhood. They described never having to make an effort or taking part in different sports activities. They expressed that parents and teachers were overprotective and kept them from strenuous activities. They were not allowed to participate in physical activities. This means, in part, that they never learned to be physically active in childhood, and therefore lacked positive experiences for motivating them to be physically active in adulthood. Those who described themselves as inactive as a child were not active as adults according to the interviews.
that is exhausting, I am not doing it (be a part of physical education). I do not need to, I have never needed to. And this was pretty stupid, if you are thinking back now. . . How stupid it was P7
The participants described that a well-informed community, where teachers and peers have knowledge and understanding, was a prerequisite for giving support to physical activity. Information from healthcare to teachers and peers could have led to a better understanding regarding disabilities due to the heart defect. The information to the community was suggested to include the importance of being physically active when having a CHD as well as more individualised advice on appropriate activities. In this way, the information would be an enabler that could have supported participants to increase physical activity during childhood.
. . .the school should be better at understanding, and then maybe healthcare could sometimes be helpful, that they explain too. . . . . .that the surroundings know and get good information about what it means. . . because you can rarely see it on the outside P2 I think that I would have needed someone who could guide me. . . P14
The lack of knowledge and understanding of the CHD created a barrier towards being involved in activities, especially during school hours. Instead of finding suitable activities that the person could do, participants described that they watched their classmates or went for a walk during gym class in school.
Energy level
The category energy level contained aspects related to physical capacity, and the subcategories were described as either enablers or barriers. improved fitness, using medical treatment and feeling vital were described as enablers, whereas being restricted by the heart defect, having comorbidity and feeling lethargic were described as barriers.
Having improved fitness was described to have increased the energy level and made it possible to be physically active. The participants described themselves as not being constrained or limited by their heart defect, thereby their aerobic fitness enabled them to be physically active. One description was that exercise training had improved their aerobic fitness. As a result, participants could perform more strenuous physical exercise, became less tired than before, and recovered faster.
You feel that the exercise training has given something, you feel like you might be able to do another lap, or that you are not as tired as you usually are. . . P12
Using medical treatment was another enabler described to improve the ability to be physically active. In some cases, inserting a pacemaker had increased physical ability and also shortened the recovery time.
Several physical symptoms that had negative impact on energy level were described as barriers. Participants described being restricted by the heart defect and experienced symptoms such as hypotension, arrhythmias and breathlessness. Aerobic exercise training (dynamic activities) and muscle exercise training at high intensity exercise became too strenuous and participants would tire faster compared with peers. In addition, they were in need of a longer recovery time.
. . .when I have been exercising at the gym lifting heavy weights above my head, I almost passed out, and then you feel very bad afterwards. Then I feel faint for several hours, I can hardly walk to the car. . . P5
Another barrier was having comorbidities such as migraine and joint related pain that affected the energy level and participants currently performed less compared to earlier in life.
Most participants worked, and it was expressed that work and recovery time affected the energy level and how physically active they could be. This is exemplified by feeling vital that meant having a good day, being well-nourished, or just feeling full of energy, which enabled them to be physically active. In contrast, having a bad day feeling lethargic could be a barrier for being physically active. Participants expressed that they adapted the activity to match the daily condition.
When I have had a good day, or have been eating well, I am excited for working out; then I can bike almost more than one song during warming up, and I feel very excited to work out and it just goes better and better. . . P4
Approach
The participants’ approaches were described as both enablers and barriers for physical activity. One enabler was having positive attitude, whereas one barrier was having a fear of movement. Furthermore, there were two subcategories in which different aspects were both enablers and barriers – having driving force versus lacking driving force and being self-confident versus lacking self-confidence.
One enabler was having a positive attitude to physical activity that was based on the positive emotions created from the physical activity. The participants described that physical activity acted as a distraction and made it possible to think about something else for a while. They expressed that they felt happier when they could get out for a while; for example, taking a walk. The happiness was also in relation to the experience of being able to handle the physical activity. Participants expressed that they got an ‘endorphin kick’ when completing a good workout.
That it feels good, that I can do it, also when you have done a good workout you get an ‘endorphin kick’ P2
A negative approach to physical activity could be created by a fear of movement, which then became a barrier. The participants thought that their health could be impaired by physical activity, and that physical effort could possibly be harmful for the heart. This was especially so if they became breathless or the heart rate increased. During childhood, parents’ fears of allowing them to be physically active had created a mental barrier that had remained in adulthood.
I had very overprotective parents, so I was not like joining physical education; I have always had such reservation that you do not need to do this and this because it may be too hard. . . P7
Having driving force was described as an enabler while lacking driving force was a barrier. Having a positive approach towards physical activity was important for the driving force; that is, if they thought the activity was fun they could perform better and did not think that it was strenuous. Driving force was expressed as wanting to participate in physical activity and to challenge the limits. Wanting to show others that they possessed the capacity to be physically active was another driving force that was described.
I really want to try, I have always been that way, I have always wanted to try things and see if they would work or not. . . P4
Participants described that their driving force for physical activity was due to their heart defect and knowing that they had to be physically active to maintain their health.
I do know what health benefits there are, and that you feel better psychologically,. . . I do not like sedentary living and I do not feel good if I have been sitting on the couch the entire day. . . P6
In contrast, lacking driving force was seen as a considerable barrier. Physical activity, in terms of exercise, was considered boring and difficult, and other activities such as painting or reading was more attractive. Participants did not like to perform exercise and expressed that they usually gave up too early when it became strenuous.
. . .it is more that I do not push myself, I do not know why, I give up too soon when it comes to sports P7
Another approach, being self-confident, was described as an enabler. Self-confidence was described as a feeling of inner trust that seemed to minimise the importance of others’ opinions. Participants described an increase in inner trust with aging. Now that they were adults, it was expressed that it was easier to speak up and tell others about the limitations of the heart defect. They could decide themselves what to do instead.
After all, when you grow older it gets easier to say no; it is like this, I do not have the energy to go quicker, you just have to buy it. . . P2
One approach that was described as a barrier was lacking self-confidence. Participants described both too low and too high self-confidence with regards to physical activity. The low self-confidence was expressed as a fear of not being able to perform at team sports as well as others. Participants expressed that they did not want others to see them become breathless or cyanotic. Instead of explaining about the heart disease, they chose not to participate at all.
but when there were too many people, I did not like that, because then. . . then it was clear that I did not have the energy for it as everyone else P9
On the other hand, too high self-confidence was expressed as setting unreasonable goals for physical activity, which meant that they could not finish the activity. One participant described that he participated in a competition as a member of a team: I was in a relay race once, and I regret it bitterly, I did not have the capacity for it, it was so. . . it was really stupid. I reached the finish line but I simply could not run 3 km P13
Environment
In this category there were subcategories interpreted both as enablers and barriers. Using technical aids was described as an enabler, while limited by physical environment was seen as a barrier. The environmental aspect having structure was interpreted as an enabler and lacking structure as a barrier to physical activity.
Using technical aids such as heart rate monitors or pedometers could be seen as enablers to increase the physical activity level. These stimulated participants to compete against themselves while improving their results. One participant described his heart rate monitor and how he could compare his results after exercise.
Becomes like a little ‘carrot’ to see that I get more even. It becomes easier to keep my green area, I have fewer peaks that hit the ceiling; I have less lazy time; it is a little bit fun, but you can still see that you get results. P11
In the subcategory limited by physical environment, physical environment included terrain, climate factors and facilities. For example, when it was described as a challenging terrain such as a hill, participants chose to take the car instead of walking. Furthermore, a long distance to a fitness centre was described as another barrier. Participants also described being affected by climatic factors such as cold, heat and wind. It took too much energy to keep the body warm in the winter or cool down on hot summer days. A problem with participation in outdoor activities during the winter was described by one participant.
just outside does not work, then I get really breathless and tired and have no energy for anything, and then I do it too much so that I become completely tired.. . . P4
In addition, lack of facilities could be a barrier. The lack of a shower and a changing room meant that participants did not walk to work because they would get sweaty and could not change clothes at work.
In the past when you had work uniforms, you could go into a changing room and change and possibly have a shower if needed; but now it is like nothing, now you should only undress and dress, then you are still a bit sweaty; no it does not work unfortunately. . . P13
Having structure was described as an enabler and lacking structure as a barrier. Finding structures that facilitated physical activities enabled participants. One way of structuring was to schedule the exercise with their partner. Finding a suitable type of exercise was another way of structuring. Some preferred exercise in groups, while others preferred training on their own due to exercise training in a group creating a feeling of pressure. Some exercise modes such as muscle training were described as easier to perform, and participants felt that they recovered faster in comparison to aerobic exercise training.
. . .set some goals or actually schedule what you should do so that it might be easier to stick to it. . . I think that I have to plan it, not just to have time with the activity, but also to have time for recovery afterwards P5
Difficulty to find a functional structure was seen as a barrier to perform physical activity. Lack of time was interpreted to be another example. Some of the participants worked full time and some had families, which made it difficult to find time for their own activities.
On weekdays you are so tired after work, and even if you have energy it will usually only be a short walk with the dog in the evening. . . maybe because I work more now than I did earlier. . . P5
Lack of time was also described as a problem in relation to having enough time to rest and recover. It was expressed that full-time work made it difficult to exercise due to the need for recovery time.
. . .then I often exercised when I was off duty, like not working the morning the day after, then I had a little more recovery in the morning and that was a little better. If I had done the same thing today then I would not have any problem to go to work and so, but then when I get home from work the day after I would have been completely exhausted. I can imagine that then you would not have the recovery that you probably should have P5
Discussion
One aim was to describe participants’ experiences of enablers and barriers for being physically active. Thereby our subcategories in many cases show a wide spectrum with endpoints being each other’s opposites.
The analysis revealed four categories – encouragement, energy level, approach and environment.
In the encouragement the results highlight that social support and encouragement in childhood to physical activity and no restrictions from parents, teachers and healthcare increased physical activity in adulthood. In contrast, lacking support and being restricted by others seemed to create barriers to physical activity.
Being encouraged meant having support from others, which in this study seemed to have a great impact on the possibility of being physically active as an adult with CHD. One important aspect was to be encouraged as a child by parents or teachers. In line with these findings, the importance of a supportive family was recently reported for a group of younger adults. 18 A previous study showed that by being encouraged, participants described that they could be physically active even though they sometimes felt physically or mentally constrained. They found appropriate levels for their physical activity and this sense of being capable remained in adulthood. On the other hand, if being restricted by others, maybe due to lack of knowledge or understanding, the participants described instead that they never had to try or to challenge themselves to be physically active as children. Although children with CHD considered themselves healthy and like everyone else, parents or teachers may see them as fragile. This may be a reason why parents or other adults restricted the children’s physical activity. 23 Individualised and consistent information and encouragement from healthcare professionals was seen as an enabler to increase physical activity. Bäck et al. (2017) showed that patients diagnosed with cardiovascular disease were more willing to participate in exercise-based cardiac rehabilitation when they received tailored and consistent information. 24 Most adults with CHD have no restrictions on participation in physical activity according to current guidelines.10,11,25 However, some participants asked for more information at schools or other public places where adolescents and adults come together. The participants had a need to explain and inform others in school about their illness, and it could be difficult to live with an invisible handicap and always having to explain about their illness. 26 One other aspect of a psychosocial nature was the experience of impaired capacity compared to others, which affected participants’ self-confidence. Physical symptoms could contribute to a psychosocial barrier, as some participants described that they did not want others to watch them become breathless or cyanotic. The feeling of having impaired capacity constrained their participation in sports.
Participants’ energy level being affected by physical symptoms such as arrhythmia and breathlessness was described as a barrier to physical activity. This is confirmed by previous reports showing correlations between physical symptoms and exercise self-efficacy and the level of physical activity.15,16,27 Furthermore, in line with previous research, 28 adults with CHD who regularly engaged in physical activity described that their aerobic fitness increased. The present study showed that vitality impacted physical activity. If a participant had a good day at work, being well-nourished or was just feeling full of energy, they felt they were able to perform better and recovered faster. The participants also described that the structure on when, where and how to perform the physical activity was helpful for the actual performance. This is in line with the results of a previous review that focused on a general population 29 and described aspects associated with higher levels of both physical activity and self-efficacy.
In the category approach, it was described that feeling physical symptoms could lead to a fear of movement; this was interpreted as a negative approach to physical activity. It was perceived as dangerous to be breathless, and that increased heart rate could be harmful. Our results showed that if the participants had been frightened by parents/relatives as children, many revealed having a mental barrier even in adulthood. A fear that physical activity would be harmful to the heart is common, but in many cases is unjustified. With a few exceptions, most adults with CHD are recommended to perform physical activity. 30 Before advising appropriate physical activities, a physician should perform a detailed physical examination including detailed medical and surgical histories along with cardiopulmonary exercise testing. 11
The present study also found that the attitude towards oneself affected physical activity. Some participants described that they had now reached an age at which they were not concerned about the thoughts of others with regard to their physical activities and ability. The participants described that aging gave them self-confidence, and thus an opportunity to handle their physical limitations. They also found appropriate levels to be physically active. A recent study showed that adults with CHD described themselves as ‘being a realist – adapting to physical ability’, 19 and the present study shows that attitudes towards oneself might be an aspect of that statement. On the contrary, self-confidence could also be seen as a barrier as some had set unrealistic goals that led to not being able to finalise the activity. One explanation might be that adults living with complex CHD do not always perceive themselves as physically limited; they are born with these limitations and do not know anything else. As adults they are so familiar with eventual limitations such that they might not even consider these as limitations but instead as just the way that it is. A previous study indicated that persons with transposition of the great arteries, surgically corrected with Mustard or Senning surgery, could participate in ‘normal’ physical activities but that highly intensive sports activities might be too strenuous. 31
Qualitative research on adults with CHD is sparse, and earlier research investigating physical activity was mostly performed on children and adolescents. This emphasises the need for research and more in-depth knowledge on adults living with CHD with regards to physical activity and how they consider their own capacity. Qualitative research contributes with an essential in-depth perspective, which is highly coveted. Knowledge about what is experienced as enablers and barriers for physical activity can provide a significant contribution to innovative ideas on how to support adults with CHD to increase their physical activity; this in its turn may prevent future acquired heart disease.
In order to measure trustworthiness and to achieve credibility and transferability in the present study, the recruitment of the participants was designed to find those who had experiences of living with complex CHD. 20 Twenty-four adults were invited to participate and 14 accepted. This could be seen as a small sample, but a major importance of interview studies is that the data are rich and in correspondence with the aim of the study. Participants were included based on their scheduled follow-up from a single centre, which may have given skewed results. However, the participants had a variety of complex CHD diagnoses, both women and men were represented and there was a wide spread in age. To ensure that dependability was reached, the analysis process, codes, categories and domains were discussed within the research group that consisted of professionals with varying knowledge about the study group.
Conclusion
The results of this study indicate that it is important to provide adults with CHD the opportunity to describe enablers and barriers for being physically active. Our findings indicate that it is important for adults with CHD to have knowledge about their own exercise capacity and that they feel safe that physical activity is not harmful. With this knowledge, participants can challenge themselves to find an appropriate level of physical activity, and in doing so put adequate pressure on themselves. Targeted training and support are needed to overcome barriers, and both adults with CHD and healthcare professionals should focus on abilities rather than on inabilities in performing physical activity. Therefore, healthcare professionals have an important role in creating a feeling of safety and in providing appropriate advice for enabling increased physical activity.
Footnotes
Acknowledgements
The author(s) would like to thank Anna Sundberg for assistance in including patients and Ulla Graneheim for creative ideas.
Providing social support and encouragement for being physically activity in childhood increases physical activity in adulthood. Low energy levels are seen as a barrier to physical activity. Optimising medical treatment as well as informing and encouraging lifestyle changes can help the person become more physically active. Encourage the person to explore different physical activities to find something enjoyable that suits him or herself and inform about normal physical reactions during physical activity to prevent fear of movement. Motivate the person to schedule physical activity to archive regularity.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Swedish Heart–Lung Foundation (20150579), the Heart Foundation of Northern Sweden, the Swedish Heart and Lung Association (registration number: E143-15), Umeå University, the County Council of Västerbotten and the Swedish Society of Nursing.