
Abstract
Background:
Cellular rejection is most common 3–6 months after heart transplantation while chronic rejection, that is, cardiac allograft vasculopathy and malignancy are the most common causes of death in heart-transplant recipients beyond the third year after transplantation. However, the heart transplantation recipient’s perceived threat of graft rejection has never been explored.
Aim:
The aim was to explore perceived threat of the risk of graft rejection and its relationship to psychological wellbeing, fatigue, health literacy, adherence and self-efficacy 1–5 years after heart transplantation.
Methods:
In a nationwide, cross-sectional study that constituted part of the Self-management after thoracic transplantation project, 79 heart recipients (68% men and 32% women with a mean age of 52.6 years) were investigated after one year (n=28), two years (n=17), three years (n=11), four years (n=17) and five years (n=6). The instruments used were: the Perceived Threat of the Risk of Graft Rejection, the Psychological General Well-being, Self-efficacy for Managing Chronic Disease, the Multidimensional Fatigue Inventory, the Newest Vital Sign and the Basel Assessment of Adherence to Immunosuppressive Medication Scale.
Results:
Twenty-eight per cent of the heart transplantation recipients perceived graft rejection as a serious threat. Intrusive anxiety was low and 37% perceived the threat of the risk of graft rejection as being beyond their control. Heart transplant recipients with high level of fatigue and low psychological well-being reported stronger intrusive anxiety and less control.
Conclusion:
A perceived threat of the risk of graft rejection is present in the everyday lives of heart transplantation recipients and is strongly related to overall psychological well-being.
Introduction
More than 5500 heart transplantations were performed worldwide during 2017. 1 During 2019, 163 heart transplantations were performed in Scandinavia, 60 of them in Sweden. 2 According to The International Society for Heart and Lung Transplantation, 3 the one-year survival after heart transplantation is 87%, five-year 72% and the 10-year survival is estimated to be 55–60%. Cellular rejection is most common 3–6 months after heart transplantation while chronic rejection, that is, cardiac allograft vasculopathy (CAV) and malignancy are the most common causes of death in heart transplant recipients beyond the third year after transplantation. After five years post transplantation, CAV affects over 30% of patients, and ensuing allograft failure from CAV eventually accounts for 30% of recipient deaths after transplantation. 4 Cardiac allograft rejection occurs when the recipient’s immune system recognizes the transplanted heart as a foreign object and triggers a cascade of immune responses. Graft rejection can be either hyperacute, acute cellular-mediated, acute antibody-mediated or chronic. Different forms of rejection require different treatment modalities. 5 Fortunately, the incidence of hyperacute rejection is rare (<1%) due to careful pretransplant screening of circulating antibodies in the recipient, prospective cross-matching of donor and recipient blood and careful ABO blood group matching. However, acute antibody-mediated rejection occurs in approximately 15% of heart recipients. 5 The clinical presentation might vary from asymptomatic to haemodynamic compromise and cardiogenic shock. Because rejection is a natural process of the body’s immune system, many of the signs and symptoms can mimic those of a generalized flu-like infection, for example, malaise, nausea, vomiting and diarrhoea. Rejection can also mimic the signs and symptoms of heart failure as it involves irritation, damage or destruction of cardiac myocytes that reduce the heart’s pumping ability, thus essentially causing heart failure. 6 Graft rejection is prevented by lifelong immunosuppressive medication.
For nearly two decades a Swedish research group has focused on recipients’ experiences of graft rejection within the context of solid organ transplantation, which is the only consistent work available regarding the organ recipients’ perspective of fear of graft rejection. The results of these studies7–11 have led to the development of a theoretical framework 12 and an understanding of the impact and consequences of fear of graft rejection on the organ recipients’ everyday life and health related quality of life. The theoretical framework involves a four-step approach to the organ recipient: 1) assessment which involves context-specific deliberative actions to approach and assess threat-induced emotions and actions to relieve intrusive anxiety in the organ recipients. Assessment can be either subjective or objective. 2) Development including person-centred nursing care plans, which is a standard intervention. 3) Implementations which are context-specific threat reducing interventions that promote the organ recipient’s mastering of GRT and support adoption of useful and reasonable strategies to protect oneself from harm, that is, a graft rejection. 4) Evaluation: the level of the perceived threat of the risk of graft rejection as a nursing outcome.
Data on heart recipients’ experiences were missing until the present study. In a recent study of lung recipients’ perceived threat of the risk of graft rejection (PTGR) 13 it was revealed that the fear of graft rejection after lung transplantation was a relatively insignificant problem with no gender differences. When it occurred, it was mainly in the form of intrusive anxiety, which was strongly related to the patient’s overall psychological well-being. A reasonable assumption is that this perceived threat is relevant for heart recipients and involves various psychological reactions, such as efforts to cope with the perceived threat. We also assumed that heart recipients with high fatigue might experience more fear of graft rejection linked to the performance of the graft and that persons with low health literacy might have difficulties in grasping the complexity of graft rejection. Further adherence is strongly linked to the prevention of graft rejection and self-efficacy is assumed to play a possible role in trust of the transplanted heart, presumably causing uncertainty regarding the performance of the heart. 14 Since heart and lung transplants are both performed within thoracic transplantation and cared for in the same context, one rationale was to compare these two groups to understand possible similarities or differences, enabling a person-centred approach. The rationale behind this study is that the patients’ inside perspective regarding the perceived threat of the risk of graft rejection after heart transplantation has never been explored. The perceived threat of the risk of graft rejection is prominent in the lives of solid organ recipients 7 and is the phenomenon that they fear the most. Therefore, the aim of the present study was to explore the perceived threat of the risk of graft rejection and its relationship to psychological general wellbeing, fatigue, health literacy, adherence and self-efficacy 1–5 years after heart transplantation as well as to compare with a cohort of lung recipients within the Swedish national Self-management after thoracic transplantation (SMATT) study. The key research questions were: what are the characteristics of the experienced threat of the risk of graft rejection and related psychosocial aspects among heart recipients? and does their experience of the threat of graft rejection differ from that of lung recipients?
Methods
Design
This multicentre, cross-sectional, cohort study is a part of the nationwide SMATT study. The SMATT study extensively investigates heart and lung recipients during the first five years after transplantation and includes a total of six different cohorts, both cross-sectional and longitudinal, as well as studies with a qualitative design.
Study population
The inclusion criteria in this study were the same as in the whole SMATT-project, that is, being a heart transplant recipient due for the annual follow-up 1–5 years after heart transplantation at either of the two thoracic transplant centres in Sweden, Swedish speaking, mentally lucid, not hospitalized and without on-going treatment for acute antibody-mediated rejection. The main reasons for not being included were poor health status as assessed by the transplant nurse at the outpatient clinic, declining to participate and non-Swedish speaking. When the study began there were 303 eligible heart recipients due for their annual follow-up 1–5 years after transplantation. Of these, 153 were invited to participate and 90 (58.8%) were included in the study. The final study group comprised 79 heart recipients. The reason for external drop-out was being included twice instead of once as intended, which occurred by mistake at two different yearly follow-ups, declining to participate, language barrier, being transplanted with several solid organs or being critically ill. Unfortunately, it is not possible to reconstruct the exact number of drops-outs for each reason since this was never documented in detail.
Instruments
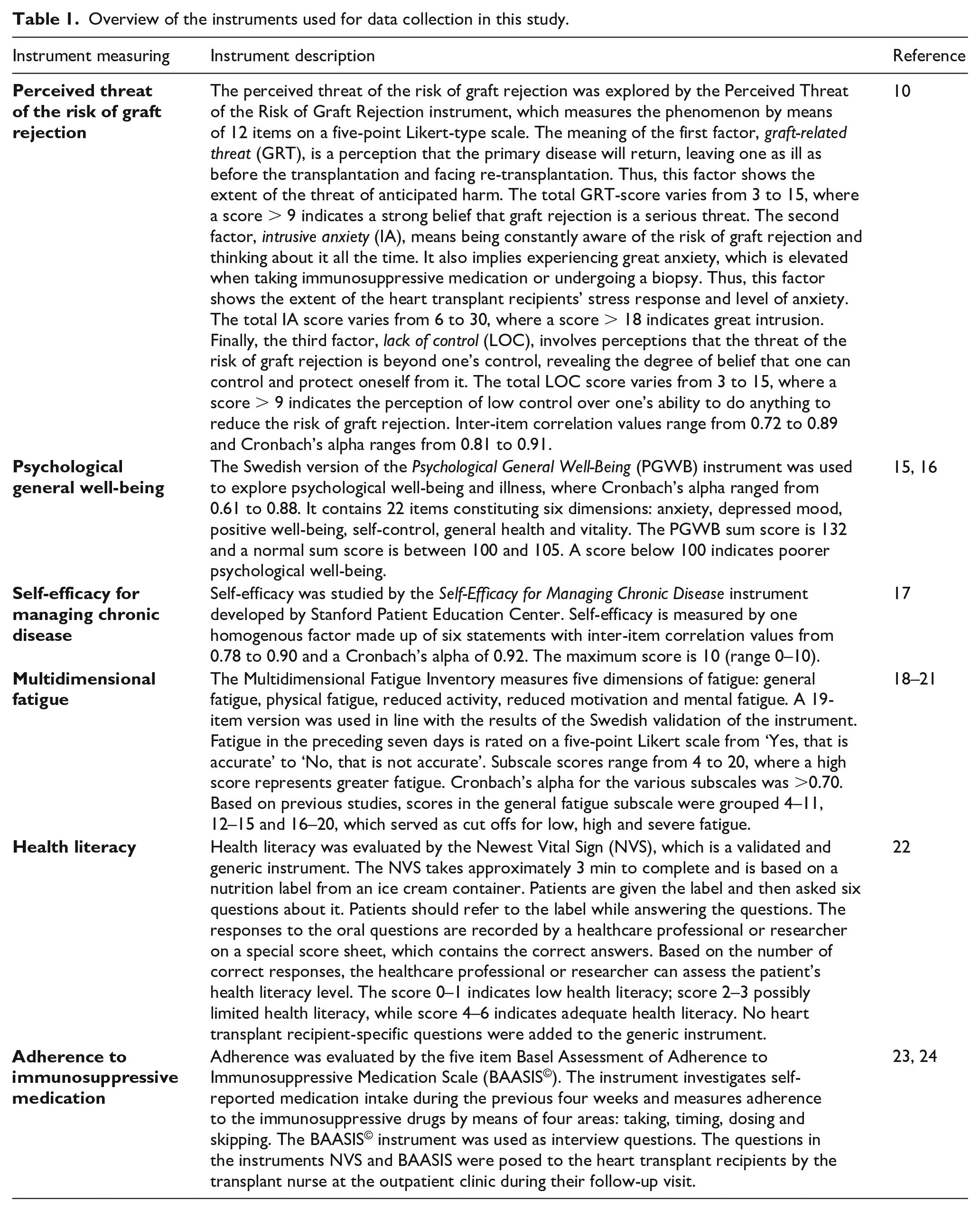
The instruments are described in previous publications from the SMATT project reporting lung recipients’ self-reported experiences. In this study, six different instruments were used to answer the research questions: the PTGR, the Psychological General Well-Being (PGWB), Self-Efficacy for Managing Chronic Disease, the Multidimensional Fatigue Inventory (MFI-20), the Newest Vital Sign (NVS) and the Basel Assessment of Adherence to Immunosuppressive Medication Scale (BAASIS©), as displayed in Table 1.10,18–27
Overview of the instruments used for data collection in this study.
Data collection
Data were collected between 2014 and 2017. The questionnaires were handed out on paper during the yearly follow-up, at each of three Swedish university hospitals by the nurses at the out-patient transplant clinic. No reminders were sent. Data were returned in a study specific envelope and stored according to the current legislation for storage of research data in Sweden. Ten heart recipients never sent their questionnaires back. Due to a high nursing turnover at the out-patient clinics at the time of the data collection reminders were not sent.
Ethics
This investigation conformed to the principles outlined in the Declaration of Helsinki. 25 Permission to carry out the study was granted by the Regional Ethical Review Board of southern Sweden (D-nr 2014-124) with supplementary approval from the Swedish Ethical Review Authority (Dnr. 2019-02769). All participants gave their written informed consent and the information they provided was kept confidential and stored by the researchers in accordance with the Swedish personal data act.
Statistics
Data analyses were mainly ordinal. Single-scale ordered category data were summarized with median and percentiles (P25, P75). When applicable, values of p < 0.05 (two-tailed) were considered statistically significant. The analysis was performed by the authors stepwise as follows:
The proportions were explored by chi-square and the distribution of PTGR and its consequences for psychological general well-being, self-efficacy, fatigue, health literacy and adherence were described.
Possible differences between two unpaired groups, for example, men and women, were explored by Mann–Whitney U.
Possible relationships were explored by Spearman’s correlation.
The SPSS Statistics 23 (SPSS Inc., IBM Corporation, Armonk, New York, USA) was used.
Results
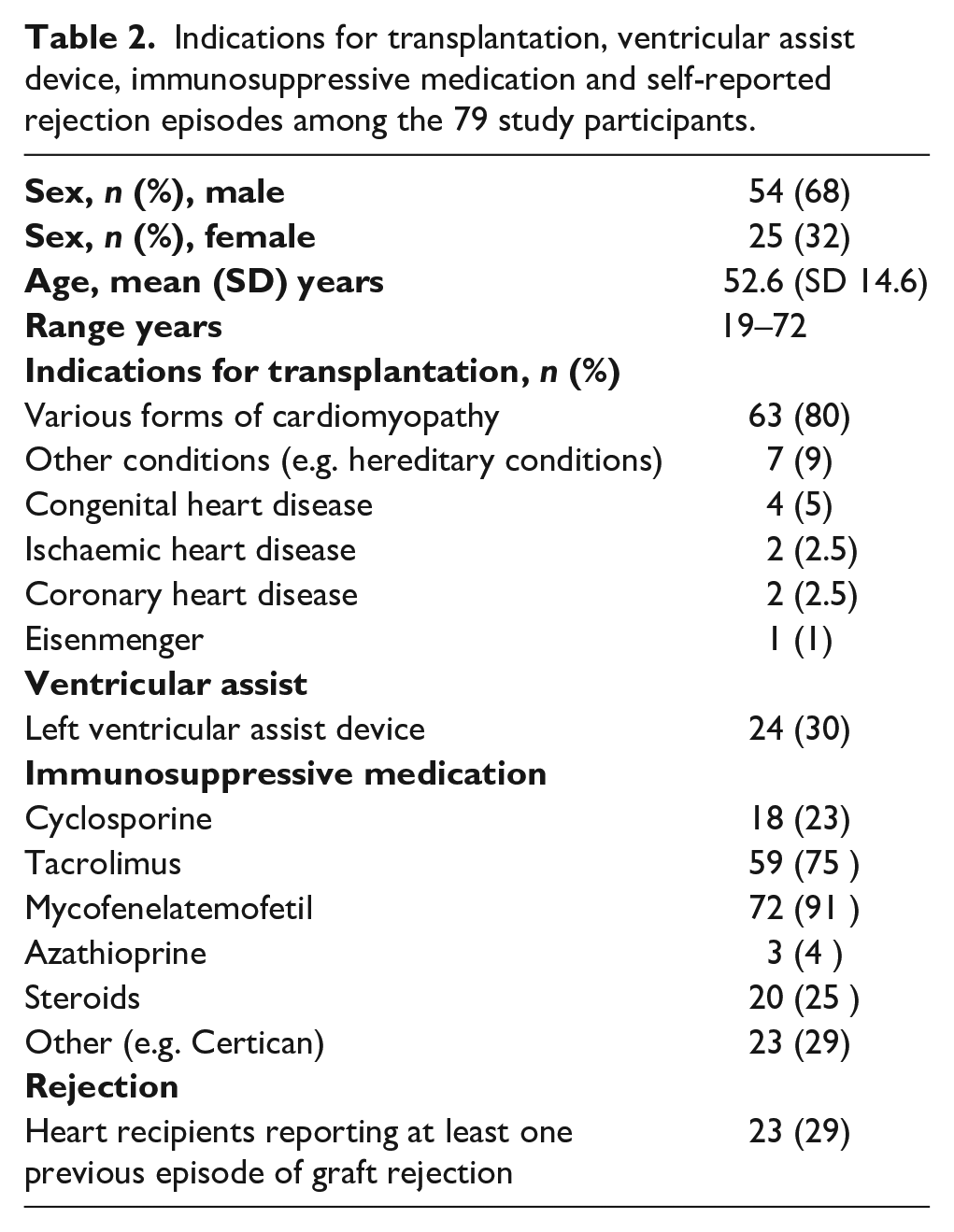
The final study group comprised 79 heart recipients followed for one year (n=28), two years (n=17), three years (n=11), four years (n=17) and five years (n=6). Demographics, indications for transplantation and medications among the 79 included participants are presented in Table 2. A cross-sectional cohort of Swedish lung recipients (n=117) previously reported within the SMATT-project was used as a comparison group. This group was transplanted during the same time frame, they had similar follow-up and their mean age was equal: 53.5 years. The gender distribution differed, which was due to different indications for transplantation as well as prevalence and incidence of different diseases causing end-stage organ failure. The lung recipients’ perceived threat of the risk of graft rejection is reported in detail in a previous publication. 13
Indications for transplantation, ventricular assist device, immunosuppressive medication and self-reported rejection episodes among the 79 study participants.
The response rates of the 79 participants in this study for the different instruments were 99% (n=78) for PTGR, 85% (n=67) for the PGWB, 89% (n=70) for Self-efficacy for Managing Chronic Disease, 97% (n=77) for MFI-19, 95% (n=75) for NVS and 97% (n=77) for the BAASIS©.
Fear of graft rejection in the whole group
In the whole group the median score for all three dimensions of PTGR, that is, graft related threat (GRT), intrusive anxiety (IA) and lack of control (LOC), was 7. Of the participants, 28% (n=22) scored 9 or above in GRT, indicating a strong experience of graft rejection as a serious threat. A great intrusion indicated by an IA score of 18 or above was experienced by 3.8% (n=3). Low control was reported by 37% (n=29). Table 3 shows the median score for each year and reveals that GRT is reduced after the second-year post transplant.
Self-reported perceived threat of graft rejection among 79 heart recipients 1–5 years after heart transplantation divided into five groups by their follow-up.
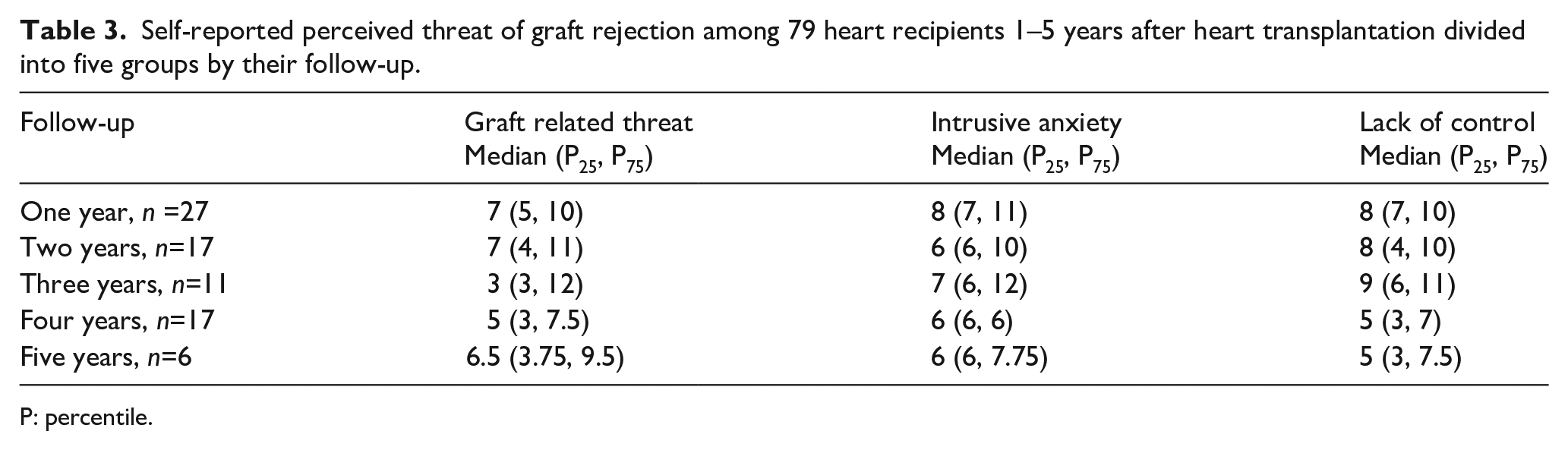
P: percentile.
Sub-group analysis regarding gender, age, ventricular assist device (VAD) treatment and previous graft rejection
There were no gender differences, as shown in Table 4. When comparing participants older and younger than 50 years, the older reported worse GRT (p=.020) while there were no differences in IA (p=.134) and LOC (p=.815). Heart recipients with a pre-transplant VAD reported more IA than those without VAD treatment, although not significant (p=.060). The recipients who self-reported one or more graft rejections reported lower GRT (p=.036) than those without rejection episodes, but equal IA (p=.580) and LOC (p=.849).
Gender experiences in self-reported perceived threat of graft rejection.
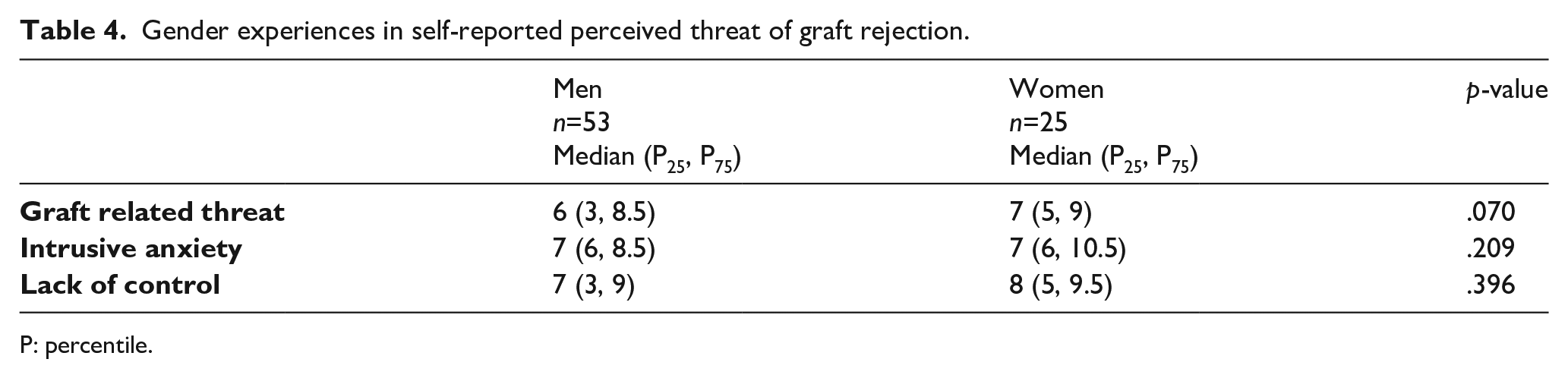
P: percentile.
Sociodemographic analysis, health literacy and adherence
When comparing groups based on sociodemographic variables no differences were revealed in the three dimensions of PTGR between those with a higher or lower education respectively or between those working half or full time versus those not working. Fear of graft rejection was not more pronounced among those considered non-adherent compared with the adherent heart recipients. There were also no differences in PTGR when comparing three different health literacy levels.
Fear of graft rejection in relation to fatigue, psychological well-being and self-efficacy
As displayed in Tables 5 and 6, participants with high fatigue experienced more IA and less control. The same pattern was found when comparing those with poor and good psychological well-being. These findings were further supported when determining relationships between PTGR, psychological well-being and the various dimensions of fatigue (Table 7). When scrutinizing each follow-up group separately, IA was strongly related to all dimensions of psychological well-being, especially at one and three years after heart transplantation. Three years after transplantation, IA was also strongly related to self-efficacy, suggesting that a high level of IA might reduce the heart recipients’ belief in their ability to master their health situation.
Differences in self-reported perceived threat of graft rejection related to level of self-reported fatigue. A score < 12 on the general fatigue scale constitutes low fatigue while a score > 12 constitutes high fatigue.
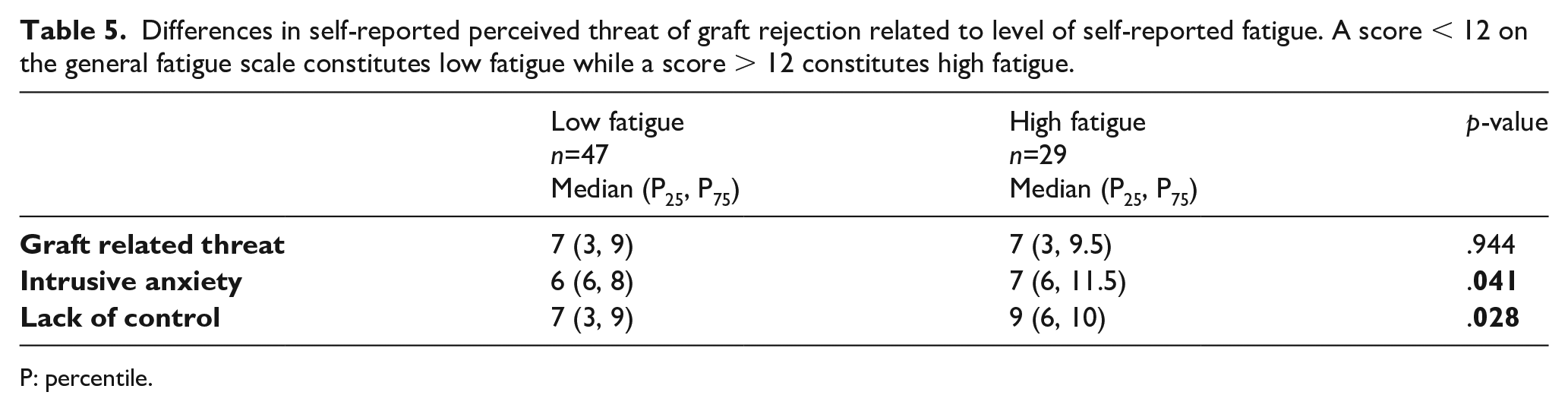
P: percentile.
Differences in self-reported perceived threat of graft rejection in relation to level of psychological well-being. A psychological general well-being sum score less than 100 constitutes poor psychological well-being.
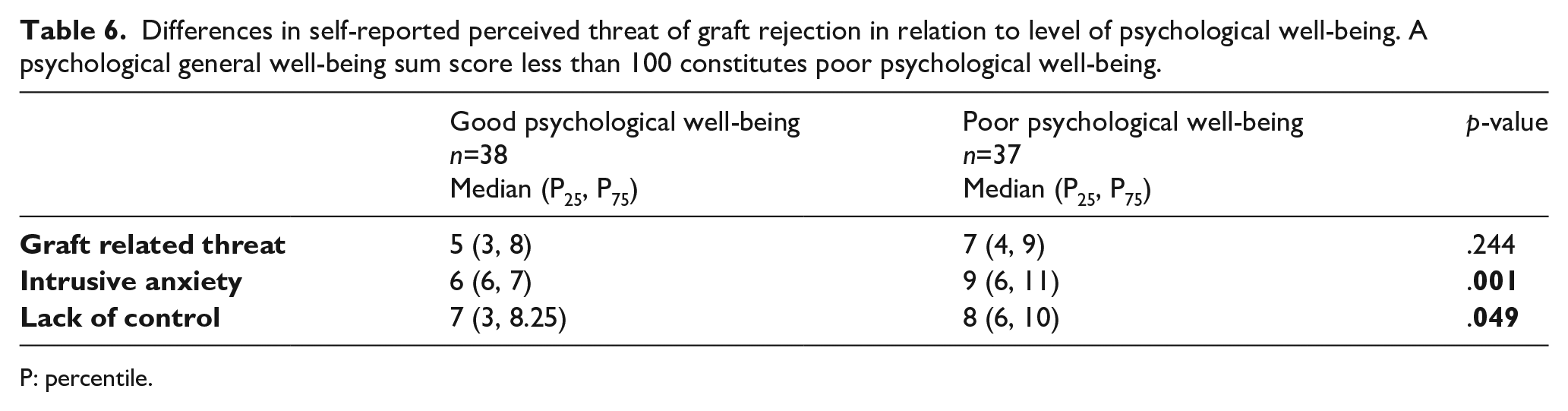
P: percentile.
Relationship between perceived threat of graft rejection (PTGR) involving the three dimensions graft-related threat (GRT), intrusive anxiety (IA) and lack of control (LOC), and psychological well-being (PGWB), fatigue and self-efficacy among 79 heart recipients 1–5 years after heart transplantation.

Significant strong correlations are shown in bold.
p<.05
p⩽.001
Fear of graft rejection among heart recipients versus lung recipients
When comparing the whole group of heart recipients with the whole lung cohort no differences in PTGR were found. However, when comparing each follow-up year, participants at their one-year follow-up reported significantly worse IA (p=.016) than lung recipients measured at the same time point. No other differences were found between heart and lung recipients. Thus, the self-reported experiences during the first five years after transplantation were fairly similar for heart and for lung recipients regardless of the follow-up year.
Discussion
The majority, 72%, of the participants reported low GRT while 28% perceived graft rejection as a serious threat. IA was low and 37% perceived that the threat of the risk of graft rejection was beyond their control and believed that they were unable to control and protect themselves from it, suggesting a fatalistic approach. The fact that almost one-third of the heart recipients perceived graft rejection as a serious threat highlights the need for person centred patient education by the transplant nurse about what graft rejection is and what it is not, based on each patient’s own meaning making and personal beliefs. Further, to allocate resources to the patients in most need, the transplant nurse could use the PTGR instrument to screen the patients in order to find those with pronounced fear.
The study showed that participants with high level of fatigue and low psychological well-being reported stronger IA and less control. The transplant nurse needs to be aware of patients with anxiety and try to identify those with great distress since that condition can increase fatigue and the overall psychological well-being. Further, those with a history of at least one self-reported rejection episode experienced less GRT. This is probably due to the fact that experiencing a successful treatment for graft rejection increases the trust in the organ. Nilsson et al. 7 revealed that solid organ recipients perceive graft rejection in many ways, from something that is easy to handle to a life-threatening condition leading to re-transplantation or even immediate death. Thus, we know that organ recipients expect damage if graft rejection occurs, that is, reduced function of their transplanted organ.
One year after transplantation liver transplant recipients experienced the threat of graft rejection as alternating between being something of no significance to fear of death. These feelings involved being constantly aware of their bodies, having a continual sense of fear, experiencing an invisible threat and being failed or simply ‘let down’ by their bodies. 8 Our result showed that at their one-year follow-up heart recipients experienced stronger IA than lung recipients one year after their transplantation in our previous study, 13 meaning being constantly aware of the risk of graft rejection and thinking about it all the time. Most organ recipients make strong efforts to protect themselves from graft rejection 7 and about 33% fear that it will occur. 9 When investigating kidney, liver and heart or lung recipients regarding GRT, Nilsson et al. 10 reported that the patients’ scores were widely spread: 33% of the patients perceived a low level of GRT, 40% were uncertain and 27% experienced a high level of GRT. However, there were few lung recipients in the study by Nilsson et al. and those that participated were added to the group of heart recipients. Most of the organ recipients (74%) reported low levels of IA. A high level of LOC was experienced by 48%. 10
There was a strong relationship between intrusive IA and all dimensions of psychological well-being, especially one and three years after heart transplantation. IA was low and 37% perceived that the threat of the risk of graft rejection is beyond their control and believe that they cannot protect themselves from it. A similar pattern was seen among Swedish lung recipients, 13 where a median of 6 (P25 6, P75 9) showed that the perceived IA was low. Seven lung recipients (6%) scored above 18, indicating problematic intrusion. Furthermore, almost 75% of the lung recipients reported that they perceived some sort of control over their ability to reduce the risk of graft rejection compared with 63% in this study of heart transplant recipients.
While thoracic transplant recipients cannot control their immune system and how it reacts to the graft, they can minimize the risk by adhering to the immunosuppressive regimen and to the restrictions recommended by the transplant professionals. However, a recent study of adherence among Swedish lung transplant recipients 26 revealed that 30% were non-adherent (35/117). Non-adherence regarding taking the immunosuppressive medication was 43% (15/35) and the most frequent non-adherence behaviour was in timing, that is, lacking punctuality (80% (28/35)). Ten participants reported more than one non-adherence dimension (29%), where the most common combination was taking and timing. Of those working full or part time 43% were non-adherent. Lung recipients able to work full or part time were significantly (p=.032) less adherent than those unable to work.
We find it reasonable that heart recipients with high fatigue and low psychological well-being reported stronger IA and less control. Fatigue most likely affects self-efficacy in a negative way, meaning that after transplantation one doubts one’s ability to master self-management, leading to a constant awareness of the risk of graft rejection and thinking about it all the time. It also means that the anxiety is elevated when taking immunosuppressive medication or undergoing a biopsy. Here it is important for transplant nurses to provide self-management support in order to improve self-efficacy. We know from previous research that great uncertainty is a cause of distress one year after heart transplantation. 14 Being uncertain regarding one’s graft function might contribute to an overall uncertainty regarding survival and life itself. We also know from previous research on coping strategies in relation to graft rejection 11 that mainly positive coping strategies are used among solid organ recipients, that is, social trust, minimization and problem reducing actions. However, those having had a rejection experienced more isolation, women used more fatalism and patients younger than 50 years reported more intrusion. There was also a very strong relationship between the factors, lack of control and the coping strategy fatalism, confirming that lack of control might be synonymous with a fatalistic approach. The coping strategies also had consequences regarding health related quality of life. The negative coping dimensions, isolation and protest, decreased general health, vitality, role-emotional, social functioning, and mental health while there was no relationship at all between the positive coping dimensions and health related quality of life. 11
Heart recipients with a history of at least one rejection episode perceived less GRT. This is reasonable as a graft rejection that was successfully treated provides an experience that the threat is manageable and that does not inevitably lead to graft failure. Learning from this experience has previously been shown to be positive. 7
Heart recipients at their one-year follow-up experienced stronger IA than lung recipients one year after transplantation, meaning that they were constantly aware of the risk of graft rejection and thought about it all the time. This is in line with Almgren et al., 14 who showed that heart recipients experience great uncertainty after one year in contrast to lung recipients, who have a constructive trajectory of recovery involving reconstructing daily occupation during their first post-transplant year. 27
There is a strong relationship between IA and all dimensions of psychological well-being, especially one and three years after heart transplantation. This finding suggests that approaching heart recipients with IA in relation to graft rejection might affect their overall psychological well-being. However, the opposite may also be clinically useful, that is, dealing with low psychological well-being and in order to minimize the fear of graft rejection. Here the middle-range theory of PTGR might be highly advantageous as it is context specific and developed from the patient perspective. 12
Dealing with a lifelong PTGR is a complex challenge for the solid organ transplant recipients, but also for the transplant nurse, whose key mission is risk assessment and health promotion throughout the whole transplant process. To have a psychologist in the clinical out-patient team would be a great advantage; however, this is close to non-existent in Sweden. For the transplant nurse; using a theoretical framework is one tool. Another strategy is to employ mobile application education tools for solid organ recipients in general and heart recipients in particular in order to relieve anxiety and uncertainty, thus supporting self-management in a long-term perspective.
Study strengths and limitations
A strength of this study is the novel approach to in-depth exploration of the fear of graft rejection from the heart recipients’ perspective, which has not previously been done. Limitations are the cross-sectional design and that the numbers of participants are small, especially when divided into each follow-up year. Not being able to declare reasons for the drop outs is of course a study limitation. Also, the study reflects a Swedish sample with low ethnical diversity decreasing the representativeness of the findings.
Conclusion
Few heart recipients (28%) experience GRT and very few (3.8%) suffer from intrusive anxiety. The fear of graft rejection is strongly related to overall psychological well-being. Heart transplant recipients with high level of fatigue and poor psychological well-being also suffer from stronger IA and more LOC, suggesting that these are symptoms of concern when evaluating the PTGR.
Footnotes
Acknowledgements
We would like to express our sincere gratitude to Johanna Granström, Clinical Nurse Specialist at Karolinska University Hospital in Stockholm, Inga-Maj Konkell R.N. and Ida Gustafsson R.N. at the Sahlgrenska University Hospital and Cecilia Åkesson, occupational therapist at Skåne University Hospital in Lund for invaluable assistance with the data collection. We would also like to give all participants a hearty thank you for part taking in this study. Author contribution: AF – design of the study, collecting the data, analysing the data, critically discussing the findings and writing the manuscript. AMK – critically discussing the findings and overall development of the manuscript. AP – critically discussing the findings and overall development of the manuscript. CR – critically discussing the findings and overall development of the manuscript. MD – critically discussing the findings and overall development of the manuscript. AL – design of the study, collecting the data, critically discussing the findings and writing the manuscript.
In transplant nursing a person-centred approach is vital to enable implementation of the below suggested implications: • Begin with a subjective assessment with a one-on-one approach, listening to the heart recipient’s perceptions of experiences of graft rejection. A simple introductory question might be the following: ‘When I say graft rejection, what comes to your mind?’ • The 12-item perceived threat of the risk of graft rejection instrument used in this study is useful for carrying out objective assessment. • Repeated instructional conversations can be a useful intervention to promote the mastering of a graft-related threat, specifically discussing the meaning of graft rejection. • Assess the level of fatigue and psychological well-being using appropriate instruments. • Psychological distress after heart transplantation causes uncertainty and fear of graft rejection is a part of being uncertain. Therefore, education and mental support on an individual basis is needed on a regular basis.
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.