
Abstract
Background
Self-efficacy refers to a person´s confidence in carrying out treatment-related activities and constitutes the foundation of self-management as well as long-term follow-up after heart transplantation. Exploring the heart recipients´ experiences by means of self-report instruments provides healthcare professionals with valuable information on how to supply self-management support after heart transplantation.
Aims
The aim was to explore self-efficacy in relation to the self-reported level of recovery and psychological wellbeing, among adult heart recipients, one to 5 years after transplantation.
Methods
This cross-sectional study includes 79 heart recipients, due for follow-up one to 5 years after transplantation. Three different self-assessment instruments were employed: the self-efficacy for managing chronic disease 6-item scale; the postoperative recovery profile; and the psychological general wellbeing instrument.
Results
The reported level of self-efficacy was high (median 8.3, maximum score 10). Significantly higher self-efficacy was seen among those who had returned to work (P = 0.003) and those without pre-transplant mechanical circulatory support (P = 0.033). In total, 65.5% (n = 52) reported being reasonably recovered, while 18.8% (n = 12) were not recovered. The median total psychological general wellbeing score was 108 (P25 = 24, P75 = 117), suggesting overall good psychological wellbeing in the whole group of heart recipients.
Conclusion
The heart transplant recipients in our study had an overall high level of self-efficacy. Low self-efficacy was found among those with a low self-reported level of recovery, pre-transplant treatment with mechanical circulatory support or who had not returned to work. This is important information for transplant professionals when helping heart recipients to balance their expectations about recovery.
Introduction
Heart transplantation (HTx) is an established life-saving treatment for people with end-stage heart failure. 1 As a result of medical advances, survival after HTx has improved. 2 With a one year survival rate of 83% and 71% surviving for 5 years, 3 perceived health and quality of life become highly important outcome measures after HTx. Despite the replacement of the heart, HTx should be viewed as a chronic condition due to the life-long immunosuppressive medication and numerous recommended restrictions involving healthy eating, physical exercise, sun protection and mastering the risk of infections. 4 It also involves psychosocial challenges during the transition from a life-threatening condition to a chronic but more stable state including coping with the threat of graft rejection 5 or other medical problems, thus constituting an uncertain and unpredictable future. The success of transplantation partly rests on the self-management ability of the heart transplant recipient (HTR), in conjunction with family and transplant professionals to manage symptoms, treatments, lifestyle changes and psychosocial, cultural and spiritual consequences. After HTx self-management is mainly constituted by the ability and process that the HTR uses in conscious attempts to gain control of his or her everyday life with a new heart rather than being controlled by it. 6
One important aspect of chronic illness management is self-efficacy, 7 which is also a part of mastering the uncertainty of being a HTR. 8 Self-efficacy is defined as a person’s confidence in carrying out a specific task. 9 In the context of chronic illness this includes managing self-care despite the presence of symptoms or side effects from the disease or medications. Self-efficacy is acting as a moderator in self-management, 6 which is why self-efficacy constitutes the foundation of self-management and self-management programmes, 10 thus it is highly relevant for transplant nurses involved in long-term management. Self-management focuses on the activities people carry out in order to create structure, discipline and control in their lives. 11 Self-management programmes enhance self-efficacy and thereby previous research has reported high levels of self-efficacy among HTRs, suggesting a great confidence about their post-transplant management. 13 This has also been shown in other transplant populations, 14 in which a high self-efficacy score was related to the extent of illness interference in activities of daily life. 14 Self-efficacy has been shown to be related to stress among HTRs 13 and also seems to correlate with depression. 13 Good perceived health among HTRs15,16 has been demonstrated up to 10 years after transplantation, 16 with a general increase in perceived health from pre-transplant levels. 17 Predictors of good perceived health after HTx are fewer psychological symptoms, social interaction, not having any transplant-related complications and low symptom distress. 15 Symptoms, setbacks and complications negatively affect performance accomplishment which potentially decreases self-efficacy. 7
However, despite the overall findings of improved health and wellbeing, some HTRs still struggle with psychological problems post-transplant. The prevalence of depression has been estimated at 17–41% up to 5 years after HTx.13,18 A high level of comorbidities and a high New York Heart Association (NYHA) score have been shown to correlate with symptoms of depression and severe distress. 19 Finally, interviews with HTRs have indicated that perceived distress after HTx is underestimated. 20 Also, health-related quality of life seems to be overestimated when using self-report instruments compared to qualitative methods in outcome research after HTx, 21 thus indicating distress to be an underestimated problem after HTx.
To the best of our knowledge, this cross-sectional, nationwide study is the first to explore HTRs` self-reported degree of recovery in relation to self-efficacy. In order to help HTRs to balance their expectations we need to understand how the recovery process is experienced from their perspective. This exploration can provide HTRs and caregivers with a road map of what to expect regarding recovery and psychological wellbeing, thus illustrating the factors potentially affecting self-management.
The rationale behind this study is that in a previous qualitative investigation we hypothesised that disappointments related to expectations, such as setbacks and complications during recovery after HTx, might hinder self-efficacy when performance accomplishment fails. 7 The absence of physical improvements during the recovery process caused by muscle weakness, sleep problems and fatigue have been identified as factors affecting performance among HTRs. 7 Our previous study suggested that assessing the HTRs’ expectations and providing support and strategies for how to balance them might generate an optimum level of self-efficacy and enable HTRs to master uncertainty. 7 Thus in order to promote adaptation to accepting uncertainty as a natural state as well as to accepting one’s present physical abilities, the aim of this study was to explore self-efficacy in relation to the self-reported level of recovery and psychological wellbeing, among adult HTRs, one to 5 years after transplantation.
Methods
Study design and participants
This cross-sectional study is a part of the Swedish national Self-Management After Thoracic Transplantation (SMATT) study, which involves six different cohorts of heart or lung recipients, who completed nine different self-report instruments. The instruments in this paper have also been used within the main project for lung recipients.
The study was carried out at the two thoracic transplant units in Sweden where HTx is performed, in addition to the largest HTx follow-up clinic. Data collection took place from 2014 to 2017. Adult HTRs who were due for their annual follow-up one to 5 years after HTx were consecutively included. Due to small groups in each year we considered all included HTRs as a single group, irrespective of which follow-up year they attended. Inclusion criteria were transplant recipients receiving only a heart, over 18 years of age, Swedish speaking, mentally lucid, no ongoing treatment for acute rejection and not hospitalised. A reason for exclusion was previous transplantation with either an organ or tissue. The patients were approached by the nurse at the outpatient clinic and received both verbal and written information about the study and provided their written informed consent. They were asked to fill in a total of nine self-report instruments, three of which are included in this study. Each participant could choose either to fill in the instruments at the clinic or at home and send them back in a pre-paid envelope.
During the data collection period a total of 303 HTRs due for their annual follow-up one to 5 years after transplantation were eligible for inclusion. 22 However, practical difficulties occurred such as staff turnover at the outpatient clinic and the fact that follow-up visits also took place at local hospitals where we were unable to contact the patients. Thus, from the 303 eligible HTRs, 153 were invited to participate and 90 (58%) were consecutively included in the study. The reason for external drop-out was being included twice instead of once, declining to participate, being transplanted with several solid organs or being severely ill. The exact figure for each reason for drop-out cannot be reconstructed. Ten HTRs forgot to send back their questionnaires and were not reminded due to the high nursing turnover at each outpatient clinic. Thus the final sample consisted of 79 HTRs who were due for follow-up at one year (n = 28), 2 years (n = 17), 3 years (n = 11), 4 years (n = 17) and 5 years (n = 6). Transplantation indications and medications are presented in Table 1.
Demographics of the included heart recipients (n = 79).
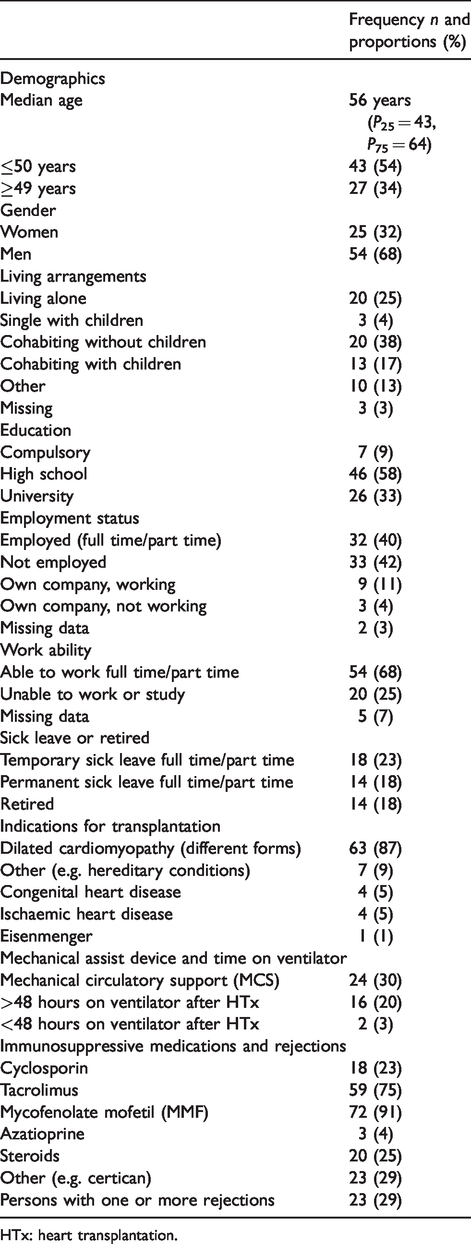
HTx: heart transplantation.
Instruments
The German version of the self-efficacy for managing chronic disease 6-item scale (SES6G) 23 was translated into Swedish by the research group and used to measure the self-efficacy score. The scale consists of six items graded in 10 steps on a Likert scale from 1 ‘not at all confident’ to 10 ‘totally confident’. A mean score is calculated with a minimum of four of the six items (allowing for two missing item responses). Thus the mean score can vary between 1 and 10, in which higher values indicate stronger self-efficacy. The German version of the scale showed good convergent construct validity with the self-efficacy for managing chronic disease 6-item scale (SES6G) (Spearman rank correlation 0.578) as well as high internal consistency (Cronbach´s alpha coefficient 0.93). 23 No validation in the Swedish context was made.
The postoperative recovery profile (PRP) was used to measure the degree of self-reported recovery. 24 The 19 questions in the instrument evaluate both mental and physical symptoms, in addition to the possible effects of daily occupation and social life. The scale has four grades, that is, none, mild, moderate and severe and the level of self-reported recovery is based on the number of ‘none‘ answers. Nineteen ‘none‘ answers equal fully recovered with a descending gradient down to over seven ‘none’ answers, which means not recovered at all. The content validity of the instrument was high, and a vast majority of the items showed a high level of intra-patient validity. 24
The Swedish version of the psychological general wellbeing (PGWB) instrument was used to measure psychological wellbeing (Table 2). 25 It contains 20 questions constituting six dimensions: anxiety, depressed mood, positive wellbeing, self-control, general health and vitality. A high score indicates better health status and psychological wellbeing. The timeframe is specified in the instrument as the last 7 days. The maximum PGWB index is 132 (best subjective wellbeing), descending to 22 (poor subjective wellbeing). 25 A normal sum score is defined as being in the range of 100–105, in which women tend to report lower wellbeing than men. 26 Inter-item correlation values range from 0.53 to 0.79 and Cronbach’s alpha ranges from 0.61 to 0.89. 25
Score for each sub-dimension of PGWB for the whole group of HTRs (n=79).
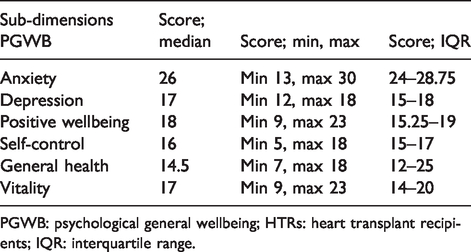
PGWB: psychological general wellbeing; HTRs: heart transplant recipients; IQR: interquartile range.
Statistical analysis
Due to the small sample size at each follow-up, the correlations between self-efficacy, demographics, subjective recovery and psychological wellbeing included the whole group, regardless of time since HTx (1–5 years).
SPSS Statistics 24 (SPSS Inc., IBM Corporation, Armonk, NY, USA) was used for analysing data, which were mainly ordinal. Descriptive statistics (patient demographics, sociodemographics, medical indication and medical treatment) are presented with frequencies. In order to test for differences between two unpaired groups we used the Mann–Whitney U test and when testing relationships between the different aspects reported we employed Spearman’s rho.
The statistical analysis was performed stepwise as follows:
Exploration of the level of self-efficacy for the whole group at each yearly follow-up. Exploration of self-efficacy depending on demographic characteristics, self-reported level of recovery and psychological wellbeing. Exploration of possible differences in the self-reported level of self-efficacy between two unpaired groups (e.g. men and women, working or not working…). Exploration of associations between the level of self-efficacy and psychological wellbeing and self-reported degree of recovery.
Ethical considerations
The study was approved by the regional ethics board of Lund (no. 2014/670-14/10) with supplementary approval from the Swedish ethical review authority (no. 2019-02769). The study conforms to the principles outlined in the Declaration of Helsinki. 27 The data were kept confidentially and stored in accordance with Swedish regulations for protection and storage of data.
Results
Patient characteristics
Demographics, indication for transplantation and immunosuppressive medication are presented in Table 1. The whole group of HTRs (n = 79) comprised 54 men (68%) and 25 women (32%). Their median age was 56 years (P25 = 43, P75 = 64) and 24 (33%) had mechanical circulatory support (MCS) pre-transplant. The response rate varied between the instruments: self-efficacy 89% (n = 70), PGWB 85% (n = 67) and PRP 81% (n = 64).
Self-efficacy
The overall self-efficacy score was high, with a median of 8.3 (P25 = 6.27, P75 = 9.23) and no differences between men and women. There was a tendency that HTRs aged over 50 years reported higher self-efficacy (P = 0.05) than those aged under 50 years. Significantly higher self-efficacy was found among those who had started work again (P = 0.003) and those without pre-transplant MCS (P = 0.033). No significant relationship was found between the groups living alone versus those cohabiting, or between those who reported having had a rejection and those who did not or between those with a higher educational level (university) and those with only an elementary education.
Self-efficacy and recovery
The self-reported recovery data showed that in the whole group, four HTRs were fully recovered, 18 almost fully recovered and 30 partly recovered. Thus 52 (81%) were reasonably recovered, while 12 (18.8%) were slightly (n = 2) or not recovered at all (n = 10). Those not recovered were seven men and five women, with a median age of 47.5 years. Seven were due for their one-year follow-up, one the 2-year follow-up, two the 3-year follow-up and two the 5-year follow-up. Half of those not recovered were working and seven had a high school or university education. Among the 12 not recovered, seven (58%) also reported low psychological wellbeing. The median self-efficacy among those not recovered was 7.5, which was significantly lower than that of those who were reasonably recovered (P = 0.047).
Self-efficacy and psychological wellbeing
The median total PGWB score was 108, minimum 54 and maximum 129, (P25 = 24, P75 = 117) suggesting overall good psychological wellbeing in the whole group of HTRs. In Table 2 scores for each sub-dimension is provided.
There were 23 HTRs, 11 men and 12 women, with a median age of 48 years, with poor psychological wellbeing defined by a PGWB sum score of less than 105. The majority (n = 9) were due for their one-year follow-up, followed by the 2-year follow-up (n = 5), 3 year (n = 5), 4 year (n = 3) and finally the 5-year follow-up (n = 1). Among those, 16 had a high school or university education, while the rest (n = 7) had compulsory education, 14 were working half or full time and nine could not work. The median self-efficacy among those with poor psychological wellbeing was 6.80. No significant differences in self-efficacy were seen between those reporting low psychological wellbeing and those who reported good psychological wellbeing. However, there was a correlation between those who reported low self-efficacy and had a lower score (r = 0.446) in the general health sub-dimension of the PGWB scale.
Discussion
The key findings in this study were that HTRs reported a relatively high level of self-efficacy with no gender differences. Higher levels of self-efficacy were found among those who had returned to work and among those who reported being reasonably recovered. HTRs treated with MCS pre-transplant reported lower self-efficacy than those who had not received MCS. The overall psychological wellbeing could be regarded as good, with no significant differences in self-efficacy among those reporting low psychological wellbeing and those reporting good psychological wellbeing.
Our results show that HTRs who were due for their yearly follow up one to 5 years after HTx report a high level of self-efficacy (median 8.3), which is in line with previous research.13, 14 Self-efficacy was lower among those who reported poor recovery, which supports previous findings, showing that self-efficacy is related to the amount of illness interference in daily life. 14 In this study we have not focused on expectations. However, our assumption is that self-efficacy is about balancing expectations, in this context about being a person living with a new heart, and thereby minimising disappointments related to the current status. Our hypothesis is that HTRs by doing this will find an optimum level of self-efficacy. 7 High expectations about recovery and wellbeing after HTx might therefore increase the risk of disappointment, leading to uncertainty about recovery and regaining health, which in turn might undermine self-efficacy, thus raising the importance of discussing what the optimum level of self-efficacy is and how it is valued.
Compared to the results in our interview study with HTRs at their one-year follow up, 7 the high level of self-efficacy in the present study was surprising. Those interviews indicated experiences of disappointment and uncertainty about the future, recovery and health, which could potentially have affected self-efficacy. Another study reported work, eating, social interaction, recreation, home management and ambulation as major problems one year after transplantation that affected functional status among HTRs, 28 which is in line with the results of our interview study. 7 This prompts the question about how to interpret the self-efficacy level. The self-efficacy score might need other complementary measurements in order to understand whether the rated level is optimal, or alternatively could be used as a measure over time to follow possible improvement. However, neither the studies by Jalowiec et al. 28 or our present study investigated self-management ability, which might have added information, because self-efficacy is a mediator for self-management. Disparities between the results of different methods might indicate a gap between data from self-report instruments or narratives, thus highlighting the importance of providing a more comprehensive picture by using complementary measurements and methods.
No differences in self-efficacy between genders were observed, which was also the hypothesis from our previous research. However, gender differences became apparent regarding symptoms and disability, in which women reported worse symptom distress and more functional disability. 29
Our results showed that those who had MCS before transplantation reported lower self-efficacy than those who did not. This is interesting, because they were probably in better condition at the time of the transplantation and had already undergone surgery, an accomplishment that could potentially have strengthened their self-efficacy. However, expectations based on previous experiences are a potential source of disappointment, especially if recovery after transplantation is more complicated and time consuming than it was after the MCS surgery. Recovery after MCS and HTx can differ, which is important information when guiding HTRs and balancing their expectations.
HTRs who had returned to work reported a higher level of self-efficacy than those who did not work. Performance accomplishment is acknowledged as an important aspect of self-efficacy, 8 which in this study was identified as returning to work and being recovered. Those who reported a low level of recovery also reported lower self-efficacy. This strengthens the results of our previous study about sources of performance accomplishment. 7 Previous studies have identified greater symptom distress and lower left ventricular ejection fraction as predictors of low functional status. 28 Those who do not return to work after HTx have been shown to experience more rejections, infections and medical complications 30 and more depression up to 10 years after HTx. 31
We hypothesised that lower psychological wellbeing would generate a lower level of self-efficacy, but surprisingly this was not the case. This result suggests that the physical aspects of accomplishment have a greater impact on self-efficacy than the mental aspects.
Methodological considerations and limitations
About 65 HTxs are performed each year in Sweden, 22 which is a relatively small number. However, this explorative design is still of great importance for optimising recovery and the prerequisite for returning to wellbeing and health after HTx. Due to the small sample size it is not relevant to present analysis of the data for each year.
According to the registry, 303 HTRs in Sweden were eligible for the study during our data collection period. However, not all HTRs have their annual follow-up at any of the transplant centres where the study took place. Due to limited resources it was only possible to include those visiting the transplant centres for their yearly follow-up in the study. The final sample illustrates the challenges involved in performing clinical studies.
The SES6G cale was translated by the research group, and due to limited resources, was not psychometrically tested in the Swedish context. However, the German and Swedish context was considered to be similar in terms of language, culture and healthcare.
Conclusion
In conclusion, it is possible to experience high self-efficacy after HTx. High self-efficacy might be a marker for return to work and being fairly recovered. However, because of the potential effects of a low level of self-efficacy on self-management ability it is important to focus on these aspects in order to provide efficient self-management support.
Implications for practice
Exploring the patients’ self-reported experiences provides healthcare professionals with a road map, which is of great importance in order to supply heart transplant recipients with enough support. Gaining more knowledge regarding what heart transplant recipients struggle with after transplantation gives healthcare professionals an opportunity to adjust efforts to match the actual needs of the heart transplant recipients. Exploring recovery and wellbeing as well as their relation to self-efficacy is essential for helping heart transplant recipients to balance their expectations about recovery and life with a new heart, thereby boosting performance accomplishment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.