
Abstract
Background:
The connection between stress and disease has been part of folk wisdom for a long time and has even made its way into our language with phrases such as ‘scared to death’ and ‘a broken heart’. Takotsubo syndrome is a form of acute, reversible heart failure characterized by ballooning of the left ventricle. Post-menopausal women are primarily affected, but cases have been described in both sexes and at all ages. The complete pathophysiology is unknown, but the disease has been connected to psychological or physical stress and a surge in catecholamines. Despite the strong connection with stress, knowledge about the life of patients before the onset of Takotsubo syndrome is lacking.
Aim:
The aim of this study was to describe and interpret patients’ narratives about long-term stress experienced before the onset of Takotsubo syndrome.
Method:
Nineteen people diagnosed with Takotsubo syndrome were interviewed. The narrative interviews were recorded and transcribed verbatim. The resulting texts were analysed using phenomenological hermeneutics.
Results:
The analysis revealed that the interviewees lived under stressful circumstances, characterized by feeling burdened by responsibilities, injustice and uncertainty, long before the onset of Takotsubo syndrome. This long-term stress wore down the defences of the interviewees to the degree that their capacity was exhausted and the smallest stressor could ‘tip them over the edge’. The findings indicated that the social structure of gender possibly contributed to the interviewees’ condition.
Conclusions:
These findings indicated that long-term stressful circumstances may cause vulnerability to acute psychological or physical stressors and, subsequently, to the onset of Takotsubo syndrome.
Keywords
Introduction
The connection between stress and disease has been part of folk wisdom for a long time and has even made its way into our language with phrases such as ‘scared to death’ and ‘a broken heart’. 1 Takotsubo syndrome (TS) is very strongly connected to stressful events. Identified stressors are mostly emotional, such as the death of a relative or a quarrel, but can also be physical, such as the use of cocaine or a subarachnoid haemorrhage. 2 The complete pathophysiology of TS is unknown, but the leading hypothesis is that overstimulation of the myocardium by catecholamines elicited by a stressful trigger leads to the development of severe contractile dysfunction, resulting in the characteristic apical akinesia in the left ventricular muscle. 3 In the acute phase, TS mimics myocardial infarction and it is thought that 1–2% of all patients with the clinical symptoms of a myocardial infarction actually have TS. The mean age range of patients with TS is between 58 and 75 and about 90% of cases occur in women. 2 The large discrepancy in the prevalence of TS between men and women has long been established,2,4,5 but explanations of this are contradictory and no clear pathophysiological explanation has been established.6–8 Stress events are a common part of everyday life 9 and most people are not affected by TS, so these alone cannot explain the syndrome, although there are factors that may make some people more susceptible to a stress trigger. Risk factors such as hormonal processes, endothelial dysfunction, genetic factors and a lifetime prevalence of depression have been suggested. 10
The concept of stress is not always clearly defined and the term is commonly used to describe both stressors and the response to stressors. 11 Selye 12 defined stress as a non-specific response of the body to any demand placed on it; he assumed that all positive and negative things that create a stress reaction are stressors and that the body’s response to different stressors is the same. 12 Another widely used definition is that by Lazarus and Folkman, 13 who viewed stress as a relationship between a person and the environment that taxes or exceeds the person’s resources and endangers their well-being. 13 A distinction is often made between acute stress, such as an earthquake or the sudden death of a relative, and long-term or chronic stress, such as caring for a sick loved one or stress at work. 11 In medical research, the concept has been adopted as a basis for examining the role of psychological factors in the causation and progression of disease. 9 In this study, stress is defined as a taxing environment or event. The reaction of the body to this environment or event is defined as the stress response. Despite the strong connection between acute stress and TS, there is a lack of research on how patients perceive their life situation before the onset of TS and whether they are subject to long-term stress. The aim of the study was to describe and interpret patients’ narratives about long-term stress experienced before the onset of TS.
Methods
Design
To fulfil the aim of this study, we chose a qualitative method, namely phenomenological hermeneutics, with an explorative design. Narrative interviews were used to gain knowledge about the informants’ personal experiences. The phenomenological hermeneutical method was developed to explore lived experience, which made it suitable for this study. 14
Participants and settings
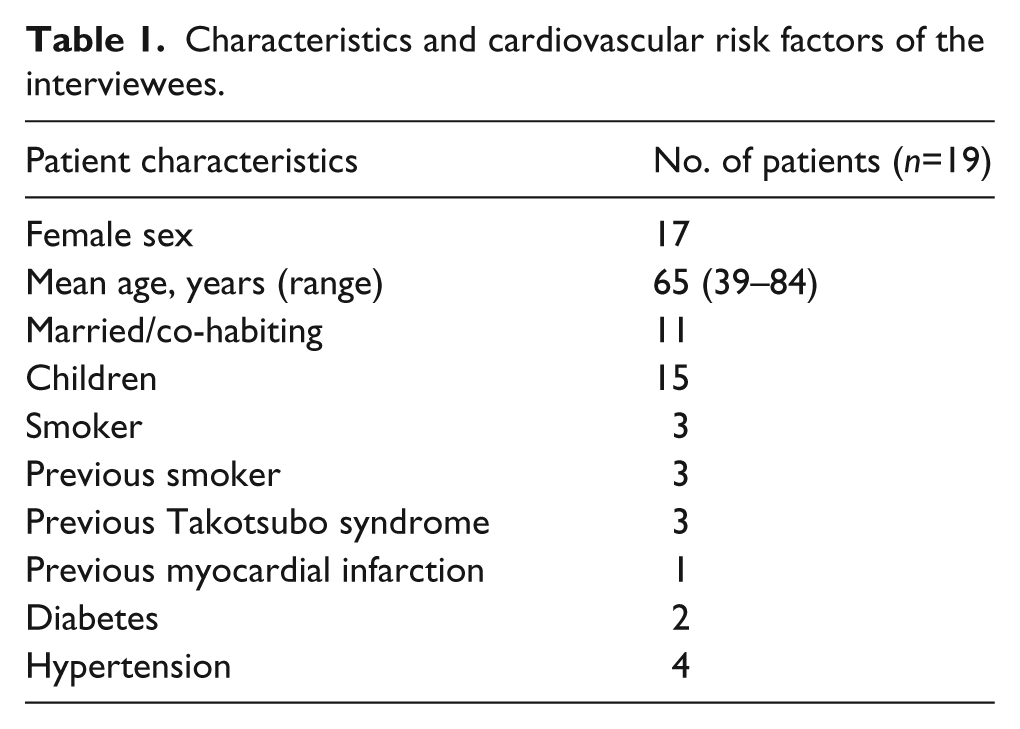
Participants were selected after coronary angiography and the following inclusion criteria were used: (a) an established diagnosis of TS according to the Gothenburg criteria, 15 which are used in the participating hospitals in Western Sweden, in the previous six months; (b) being physically and mentally capable of participating; and (c) able to speak Swedish. A strategic sample was used to include participants of both sexes and of a wide age range. Twenty-five patients were asked to participate, either at hospital or by telephone after discharge; three declined, two were excluded because no narrative could be obtained, and one was excluded because she was not diagnosed with TS. The remaining 19 participants were included in this study. The characteristics and cardiovascular risk factors of these patients are described in Table 1; there was no difference between the men and women.
Characteristics and cardiovascular risk factors of the interviewees.
Ethical considerations
The study was approved by the Regional Ethical Review Board of the University of Gothenburg (Application No. 275-11 and Amendment T693-11) and conforms to the Declaration of Helsinki. 16 Informed consent was obtained from each participant.
Data collection
The interviews were conducted during 2011 and 2012, seven during hospital admission and 12 after discharge. In two cases, a face-to-face meeting could not be arranged and the interviews were conducted over the phone. Data were collected through narrative interviews, which lasted for 15–120 minutes and were recorded and transcribed verbatim, resulting in rich descriptions. In total, the transcribed interviews consisted of 165,789 words, equivalent to 235 pages of text.
Interpretation of data
By analysing the narratives in the form of text, it is possible to take part in other peoples’ experiences, which are otherwise personal. The phenomenological hermeneutic approach has been developed over the last two decades to provide a structured and comprehensive way of interpreting the meaning of a text. It draws on both phenomenology and hermeneutics. From phenomenology, it takes its focus on essential meaning and emphasizes that preconceptions should be restrained. From hermeneutics, it takes the tradition of interpretation because phenomena conveyed through text cannot be understood without interpretation. The analysis entails a circular stepwise process, back and forth between understanding and explaining the text. It consists of three intertwined phases: naïve reading, structural analysis and interpretation of the whole. 14
Naïve reading and structural analysis
In the naïve reading, the text is read through and an impression of the meaning of the text is formed. In the structural analysis, the text is divided into meaning units; those parts of the text that are not relevant to the aim are considered, but are not included in the analysis. The meaning units are abstracted and formed into sub-themes. The sub-themes are formed into themes and possibly a main theme. The whole process of analysis is a dialectical movement between focusing on the individual parts and the overall impression of the text. The structural analysis is a validation of the naïve reading; it may be in concordance with it, but it may also reveal new aspects of what was initially formulated as a guess or idea of what the text is about (i.e. naïve reading). Several structural analyses may be performed to explore aspects of the phenomena. 14
Interpretation of the whole
In the final part of the analysis, the pre-understanding, naïve reading and structural analysis are taken into consideration when interpreting the overall meaning of the text. To achieve a more profound understanding of the text, theoretical literature is consulted and reflected upon simultaneously with the interpretation of the text. 14 For this study, gender theory was chosen and the interpretation of the whole has, in this paper, been combined with the discussion.
Findings
The first impression of the text was that, in patients where a stress trigger had occurred, this trigger was not experienced as traumatic or very stressful. Instead, the interviewees reported being subjected to low intensity stress for a long time before the onset of TS and they experienced this as more burdensome. All of the interviewees described that the circumstances had been present for a long time and most described situations dating back years or even decades. Furthermore, the naïve reading revealed that the interviewees worried a lot, both about practical things and for the people around them. The interviewees did not seem at peace with their situation in life or how their life had turned out.
The structural analysis confirmed the first impressions of the naïve reading that long-term stress was more burdensome for the interviewees than stress triggers. For this reason, the structural analysis focused on the meaning of living under long-term stressful circumstances and not an eventual stress trigger. The analysis represents the body of text as a whole and every one of the 19 interviews is represented in all of the themes. An overview of the main theme, themes and sub-themes can be found in Table 2.
Overview of the main theme, themes and sub-themes in the phenomenological hermeneutical study of long-term stress experienced before the onset of Takotsubo syndrome.

Worn down to the bone
The analysis revealed the presence of a stressful life situation long before the onset of TS. This situation was characterized by feelings of injustice and powerlessness to change the situation. The interviewees felt that there was no possible way to act that could ease their burden. Feelings of injustice regarding the situation and other people’s behaviour were present. Moreover, mistrust in other peoples’ ability to perform tasks and take responsibility led to a constant state of readiness to help relieve other peoples’ worries and problems. Despite this, the interviewees wanted to be able to trust other people, to relax and not be constantly ready to act. Continual dwelling on the past, on the unsatisfying situation and worrying about the future rendered a barrier to living in the present. In addition, feelings of inner stress, loneliness, not feeling part of a wider context and a feeling of being misunderstood were present at the same time as the interviewees built walls around themselves and did not ask for help. The hopelessness and lack of power over the situation wore down personal resources. This was a prolonged process that slowly peeled away individuals’ resources until they balanced on the verge of illness. These experiences were the result of a combined burden and not tied to specific events: ‘Yes, tired and weak as if I can’t fight anymore’ (patient 3).
Everlasting responsibilities
The interviewees felt a need to protect, help and worry about others: ‘I probably worry a lot and I should sort of protect our daughter’ (patient 15). Instead of burdening others with their own problems, the interviewees chose to keep them to themselves. For example, one interviewee did not tell their family about a long period of illness. Moreover, a strong façade and always being there for others was also important. Having lots of responsibility was experienced as both a burden and enjoyable in the sense that it entailed appreciation from others, which was desired. Busyness was a wanted burden because it provided the satisfaction of being needed and asked to help, but it was a burden when the influx of tasks and responsibilities could not be controlled – for example, by caring for a dependent family member. Furthermore, others always asked for help with new tasks, such as painting, cleaning or watching children: ‘And it fell on me to prepare it. As it usually does. Partly I want to make the food and I find it fun’ (patient 2). Satisfaction was also found in being proficient, with the concomitant assumption that everyone else should be equally proficient and active. When people were not, or were less concerned with details, the interviewees found this irritating. Their activity made them feel different from other people and not totally accepted. This, together with the influx of eternal responsibilities, culminated in a sense of powerlessness.
Recurring injustice
Not having needs met led to feelings of loneliness and abandonment. Furthermore, the interviewees reported receiving less appreciation than they thought they deserved, and feeling that when appreciation was given it was too little, too late. Living in an unhealthy relationship was one circumstance where needs were not meet. Interviewees gave a lot of themselves and were disappointed that others did not appreciate that they did not want to spend all their time servicing others – for example, by helping with choirs. To be hardworking and attentive was considered a virtue and this was expected from others. When these standards were not lived up to, it was a disappointment to not get the same consideration in return. The interviewees felt that others should notice their needs and that their own responsibility in asking for and receiving help and support was lost, which resulted in a sense of powerlessness: ‘I expect it to be in order when I come to do things because I always leave everything in order … I don’t understand why I waste energy on it because I know it won’t be in order’ (patient 17). To always be considerate to others and not receive the same in return was seen as a great injustice. Having to live with recurrent conflicts that could not be avoided was one example. This frustration to not be able to influence the situation led to feelings of powerlessness, hopelessness and injustice: ‘No, he sold everything online. I called the police … I called the insurance agency, nobody does anything’ (patient 18). Remembrance of events in the past that had led to disappointment resulted in feelings of sadness over how things turned out. The interviewees had always worked hard and done the right thing, but they were still not rewarded. They had experienced a lack of control over these events and they were stained by unjust treatment. The choice to keep things active by dwelling on the past, which could not be accepted, made it impossible to live in the present and find peace: ‘Yes, I became so sad in a way that I hadn’t done, taken care of it before’ (patient 7).
Perpetual uncertainty
This theme is characterized by a sense of powerlessness over the situation, which was seen as static and impossible to change. Endurance of the situation was a survival mechanism and a way of diminishing the situation. The acceptance of the life situation and the sense of powerlessness became an almost self-imposed inability to change the life situation. The interviewees often diminished the severity of their problems. One way of maintaining a capacity of endurance was to try to turn every situation into something positive, even though there was nothing positive in the situation. One interviewee said that a positive thing that came out of their daughter falling ill was that they could help her. The diminishment of problems and always trying to see the positive aspect of situations were survival mechanisms to gain some control over the situation and to facilitate endurance. Furthermore, it was very important to be appropriate and keep up appearances. Things should be done in the correct way and a feeling of doing things a little better than other people was apparent. Help was not asked for because the interviewees did not want to complain or be bothersome. Moreover, asking for help may have resulted in refusal, which was feared: ‘I tinker a lot, it must be in a certain order, place demands on myself. Actually perfect’ (patient 13). An inner insecurity or fear of being insufficient was almost constantly present. This worrying was not directed towards anything specific. Instead, some interviewees described it as part of their personality. If one worrying thing was resolved, it was immediately replaced by something new: ‘I stress myself when it’s something even though I don’t need to do it I do it internally and it’s tiresome. Why do you do that? I wish I could be calm’ (patient 11).
Interpretation of the whole and discussion
The analysis of the text showed that the interviewees lived under stressful circumstances long before the onset of TS. These stressful life circumstances were characterized by experiences of everlasting demands and responsibilities, being unjustly treated, not getting what they were entitled to, and not being able to control or get out of the situation. Long-term stress before the onset of TS has also been found in previous studies. Kastaun et al. 17 showed that patients with TS had had more stressful life events, such as abuse, severe injury or spousal loss, than both patients with myocardial infarction and healthy controls. A higher frequency of long-term stress – for example, recurrent conflicts or a dependent family member – than patients with myocardial infarction was also found by Delmas et al. 18 The findings in our study show that the same or similar situations – unhealthy relationships, a dependent family member or recurrent conflicts – led to long-term stress that wore down the resources of the interviewees. The presence of long-term stressful circumstances is in agreement with a previous interview study. 19 Our findings, together with the previously reported studies, give a clear indication that the patients’ life situation was perceived as stressful in agreement with the definition of Lazarus and Folkman 13 and should therefore create biological responses to the taxing environment. 12 Moreover, the connection between long-term stress and heart disease, primarily cardiovascular, is long established.11,20 Psychosocial stress, such as described in this study, leads both to an increased risk of myocardial infarction 20 and a poorer prognosis after an infarction. 21 Long-term stress should be considered a risk factor for TS.
To examine the sex discrepancy in the prevalence of TS further and to gain an understanding of why the interviewees may be exposed to long-term stress, our findings were analysed from a gender theory perspective. Gender theory does not view disease as a passive unfolding of biology, but instead tries to understand how culture and social structures affect the biological body and therefore contribute to disease. 22 The different life circumstances, such as different amounts of long-term stress, of women and men take their toll on the human body and, at least partly, determine what diseases people are affected by, 23 which is in line with the described definition of stress.12,13 For example, although men have a shorter life expectancy, women report more strain and psychological symptoms, such as stress. 9 The intrinsic power gradient in the gender structure of society – in which women as a group have less power, control and influence over their situation and life than men as a group – is thought to be one reason that mental illness is more prevalent in women than in men. This is a social structure, which we are all co-creators of and which is not the result of individual actions. 22
To gain a more complete explanation of how inequality is structured and reproduced in formally and judicially equal societies, we can use love as an analytical tool. According to Jónasdóttir, 24 the dominating form of socio-sexual relations is love power, generally given voluntarily by women and exploited by men. Men gain access to the resources, care and love of women without returning these resources. This happens under stipulations that make women incapable of building emotional reserves and authoritative social powers. This is possible as a result of the different stipulations for women and men. Women need to love and be loved to be socio-existentially confirmed – that is, to become a person. However, women do not fully control how and under which conditions they may legitimately use their capacities. The consequence of this exploitation is an exhaustion of capacities. 24
The findings from this study are concordant with gender theory 22 and the theoretical writing of Jónasdóttir. 24 Both the female and male interviewees adopted or were assigned female roles, such as taking care of and worrying about others, organizing and being responsible for their home life. The findings showed that the interviewees gave a lot of themselves and did not feel that they received the same in return. They also needed to be busy, helpful and not be cumbrous to feel confirmed and validated as persons. Jónasdóttir 24 writes that women need to love to be confirmed; the interviewees needed to help and protect – that is, love – others to feel accepted. Moreover, the intrinsic power gradient in gender structure is evident in these findings. The interviewees could not control the stipulations of how and when they assisted others, which was frustrating. The findings show that the interviewees did not fully feel a part of society, which was also described by Jónasdóttir. 24 Furthermore, the interviewees felt trapped and that they could not change their circumstances. These circumstances slowly drained the interviewees of power and resources and carved away their resilience. Living under these circumstances wore the interviewees down to the degree that they felt their capacity was exhausted and the smallest stressor could tip them over the edge.
Further research is needed to investigate whether there is a higher prevalence of stress among patients affected by TS than among patients with other heart diseases or the general population. This could be achieved by using questionnaires. A sense of coherence, depression and anxiety are other aspects that may influence the perception of stress and could therefore give further insights if they were investigated.
According to Lincoln and Guba, 25 the trustworthiness of qualitative studies consists of four parts: credibility, dependability, confirmability and transferability. One single truth is not sought in phenomenological hermeneutics because there is always more than one way of interpreting the text. 26 However, not all possible interpretations are equally probable. The timing of the interviews in relation to the onset of TS can be seen as a limitation. This could have caused some recall bias, but because the primary focus of the study was how the interviewees lived long term before the onset of TS, this was not considered to be a major drawback. Some of the narratives described events that happened years or, in some cases, decades, before the interview, so a couple of months of lag from the diagnosis of TS to the interview probably did not greatly affect the participants’ memory. The analysis of the text was discussed by SW, KU, SM and IE until agreement was met to guarantee as truthful and reproducible an interpretation as possible. The first interview was conducted by IE and the remaining by SW. IE has long experience of clinical cardiac care, whereas SW has none. This was assumed to offer a more unbiased interview process. Transferability is always a delicate matter in qualitative studies.
A second limitation of the study was the sample size compared with quantitative studies. Nineteen interviews are considered to be a large sample for a qualitative study and the great mass of text is an indicator of rich interviews. In addition, only two men were included. Although more men would have been desirable, the sex distribution of the participants is in line of that of the disease. 2 Given the relatively large sample size, the large body of text and the diversity in the age of the interviewees, the findings should be transferable to other settings when the few narratives from men are taken into account.
Conclusions and clinical implications
These findings indicate that stressful circumstances, such as gender structures in society and the entailing social roles, may cause vulnerability. This vulnerability, in turn, contributes to an increased susceptibility to acute psychological or physical stressors, which triggers TS. This study showed that long-term exposure to stress could be an important predictor of why a minority of people are affected by TS following an acute stressor.
In conclusion, this study indicates that prolonged perceived psychosocial stress is a component in the onset of TS. Prolonged psychosocial stress, enhanced by the identities ascribed by society’s gender structure, wears down defences and creates vulnerability to an acute stressor. The acute stressor is not the sole cause of TS, but rather the ‘last straw that breaks the camel’s back’.
Footnotes
Acknowledgements
The authors thank the study participants for sharing their experiences.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research was supported by the Centre for Person-Centred Care (GPCC), University of Gothenburg, Sweden. GPCC is funded by the Swedish Government`s grant for Strategic Research Areas, Care Sciences (Application to Swedish Research Council No. 2009-1088) and co-founded by the University of Gothenburg, Sweden. It was also supported in accordance to the the Swedish agreement between the government and county councils concerning economic support for providing an infrastructure for research and education for doctors (ALF). The Swedish Heart and Lung Association, Emelle Fund and the Royal and Hvitfeldtska Foundation also contributed to the funding of the study.
Long-term stress was present long before onset of Takotsubo syndrome, which may have worn down the defences of the interviewees and caused a vulnerability to this syndrome. Gender structure and its division of labour means that women and men are exposed to different types of strains – for example, stress – which take their toll on the body. Health care professionals need to be aware that the gender structure in society may influence health.