
Abstract
There has been an international effort to improve the quality of care available to persons living with dementia and their caregivers. As such, research has emphasized the importance of community-based interventions designed to help mitigate some of the health effects associated with caregiving. Physical activity and social support are two elements with the potential to enhance caregivers’ health and may be beneficial to include when designing and implementing interventions. Thus, to inform implementation and future research, this scoping review sought to describe and identify what is already known about physical activity and/or social support and dementia caregivers' physical, mental and social well-being. To do this, we followed Arksey and O’Malley’s framework for scoping reviews. Five databases (SPORTdiscus, CINAHL, PubMed, MEDLINE, PsychINFO) were searched in October 2022 and again in February 2024, and July 2025. Covidence was used to organize all relevant studies, and two researchers independently reviewed all articles. Knowledge users (dementia caregivers & community program providers) (n = 4) were also consulted during a focus group to determine if their lived experiences aligned with the findings. Thirty-four studies met the inclusion criteria. Ten studies examined physical activity; 14 studies examined social support; and 10 studies examined interventions inclusive of physical activity and social support. Regardless of intervention type, the most common finding was participation increased caregivers’ mental well-being. No difference in physical or mental health outcomes were found between in-person and online interventions. Participation in joint reminiscence therapy was the only intervention to result in a decrease in health. All knowledge users agreed with this finding. From this review it is evident that participation in PA and/or social support is beneficial for the physical, mental and social well-being of dementia caregivers. The findings from this review may help to inform the development and improvement of community-based interventions for this population.
Introduction
By 2050, estimates suggest over one million dementia caregivers in Canada (Alzheimer Society of Canada, 2022) and over 11 million within the United States (Alzheimer Association, 2025). Dementia caregivers, often called “invisible second patients”, are essential to the health of care recipients (Brodaty & Donkin, 2009, p. 217). Despite some positive effects, dementia caregivers face an increased risk of developing negative health outcomes due to the progressive impairments in cognition, daily functioning, and behavioural expressions associated with dementia (Vitaliano et al., 2003; Zhang et al., 2006). However, the effects experienced by caregivers are often associated with the age of the care recipients, with caregivers for people with young onset dementia (i.e., dementia diagnosed before the age of 65) (Alzheimer Society of Canada, 2023 May 31; Rosser et al., 2010) experiencing an increased risk of developing ill-health (such as depression or anxiety) in comparison to late-onset dementia caregivers (i.e., dementia diagnosed after the age of 65) (Aria et al., 2007; Hvidsten et al., 2020; Kimura et al., 2021). Although less prevalent than late-onset dementia, young onset dementia accounts for approximately 3.9 million dementia cases worldwide (Hendriks et al., 2021). People with young onset dementia often experience a misdiagnosis or delay in diagnosis which may be attributed to lower prevalence rates (Harris et al., 2004; Prince et al., 2013), higher occurrence of early neuropsychiatric symptoms (e.g., mood disturbances, anxiety, depression) (Harris, 2004; Prince et al., 2013), and variability in terms of the types of dementia experienced (i.e., higher rates of rare dementia’s such as Lewy body dementia or Frontotemporal dementia) (Hendricks et al., 2021; Vieira et al., 2013). Likewise, due to the timing of the diagnosis, individuals are often in their peak earning years (Kilty et al., 2023) and thus may may still be working and/or caring for dependent children (Greenwood & Smith, 2016; Kilty et al., 2023), causing young onset dementia to affect the entire family (Aspo et al., 2023). These unique factors help explain why previous research has found caregivers for people with young onset dementia to experience greater health effects in comparison to late-onset dementia caregivers. Because of this, previous research has highlighted the need for tailored support services and information regarding young onset dementia (Millenaar et al., 2016; Sansoni et al., 2016); however, tailored services are not always feasible making it imperative to understand how traditional dementia services influence young onset dementia caregivers’ health.
Physical activity is defined as any form of purposeful movement increasing the body’s metabolic rate and can take the form of sport, leisure, transportation, self-care, and play (Speakman & Selman, 2003). Research has found regular participation in physical activity has physical and psychological benefits for people of all ages; however, less is known about physical activity and the health of dementia caregivers (i.e., young onset and late-onset) (Loi et al., 2014). Nonetheless, a few studies have found physical activity can increase physical strength/stamina required to perform caregiving duties, while decreasing feelings of depression (Arai et al., 2007; Etkin et al., 2008), and perceived caregiver strain (Orgeta & Castillo, 2014).
Similarly, several studies indicate the physical and psychological benefits of social support (e.g., Ozbay et al., 2007; Southwick et al., 2005). However, the definition of social support varies by source. Some definitions focus on functional aspects (e.g., type of support – emotional, informational) while others focus on structural support (e.g., number, type, quality of relationships) (Gottlieb & Bergen, 2010). This makes the conceptualization of social support complex because individuals receive social support through informal social networks (e.g., friends, family) but also formal support services (e.g., counselling) (Dam et al., 2016). To help navigate the complexities of social support, previous reviews regarding dementia caregivers narrowed their focus to one type of psychosocial intervention, namely formal support groups (Chien et al., 2011), befriending initiatives (Lins et al., 2014), or virtual support (Boots et al., 2014; McKechnie et al., 2014; Smith & Greenwood, 2014). However, narrowing the focus to one form of psychosocial support presents challenges for comparison due to variability in intervention designs and thus limits our understanding of the effects of social support on dementia caregivers’ health. A 2016 systematic review addressed this and defined social support as “the social resources persons perceive to be available or that are actually provided to them by non-professionals in the context of both formal support groups and informal helping relationships” (Cohen et al., 2000, p. 4). Here, regardless of intervention category, caregivers’ well-being was positively affected by social support; however, emphasized future research should continue to examine social support since it is a multi-dimensional concept and should consider objective (frequency) and subjective (perceived satisfaction) social support measures (Dam et al., 2016). Further, the experiences of young onset dementia caregivers were not acknowledged making it unclear if the results were applicable to this population.
Despite individual benefits of physical activity and social support, to our understanding, no reviews to-date have examined interventions inclusive of both physical activity and social support, rather they have examined interventions inclusive of physical activity or social support, which limits practitioners understanding of the types of interventions beneficial for caregivers’ health. Previous reviews (Dam et al., 2016; Orgeta & Castillo, 2014) also did not consider if participants were young onset dementia caregivers or late-onset dementia caregivers despite the existing differences in needs (e.g., Lim et al., 2018; Millenaar et al., 2016). Thus, the purpose of this review was to update and add to existing knowledge by examining physical activity interventions, social support interventions, and interventions inclusive of both within the context of young onset dementia and late-onset dementia caregivers. Due to the complexities of the social support definition, the selection of social support papers was guided by the theory of Cohen, also used by Dam et al. (2016). However, unlike Dam et al. (2016) this review only examines formal social support interventions (i.e., from professionals/public services) and does not consider social support from informal relationships (e.g., friends, family) (Shiba et al., 2016). Narrowing the focus to only formal social support allowed for better comparison between the various interventions, and thus greater insight into the types of formal social support interventions beneficial for dementia caregivers health. In sum, this review’s objectives were to: (1) identify and describe what is already know about physical activity and/or social support interventions and the health of dementia caregivers; and (2) understand the breadth of literature on PA and/or social support within the context of young onset dementia and late-onset dementia caregivers. As such, since objective two of this review was to understand the breadth of literature on physical activity and/or social support within the context of young onset dementia and late-onset dementia caregivers it was important to consider all types of formal social support interventions and not restrict our inclusion to solely one type of formal social support (e.g., formal support groups, or formal virtual support), like previous reviews (see for example: Chien et al., 2011; Lins et al., 2014; Boots et al., 2014).
Methods
This review was guided by Arksey and O’Malley’s (2005) five-stage framework for scoping reviews. See Wang et al. (2022) and Roberts et al. (2024) for other relevant studies utilizing this framework.
Stage 1: Identify the Research Question
Research questions included: (1) What are the primary and secondary health outcomes of community-based physical activity interventions for dementia caregivers? (2) What are the primary and secondary health outcomes of community-based social support interventions for dementia caregivers (3) What contextual factors (e.g., intervention location, group composition) are considered within community-based physical activity and/or social support interventions for dementia caregivers? and (4) What are the characteristics of the physical activity and/or social support interventions implemented for dementia caregivers? For this study health was defined as a “state of complete physical, mental, and social well-being” (World Health Organization, 2025) and thus all data was extracted corresponding to physical, mental, and social well-being when discussing health outcomes.
Stage 2: Identify Relevant Studies
Keywords and Inclusion Criteria
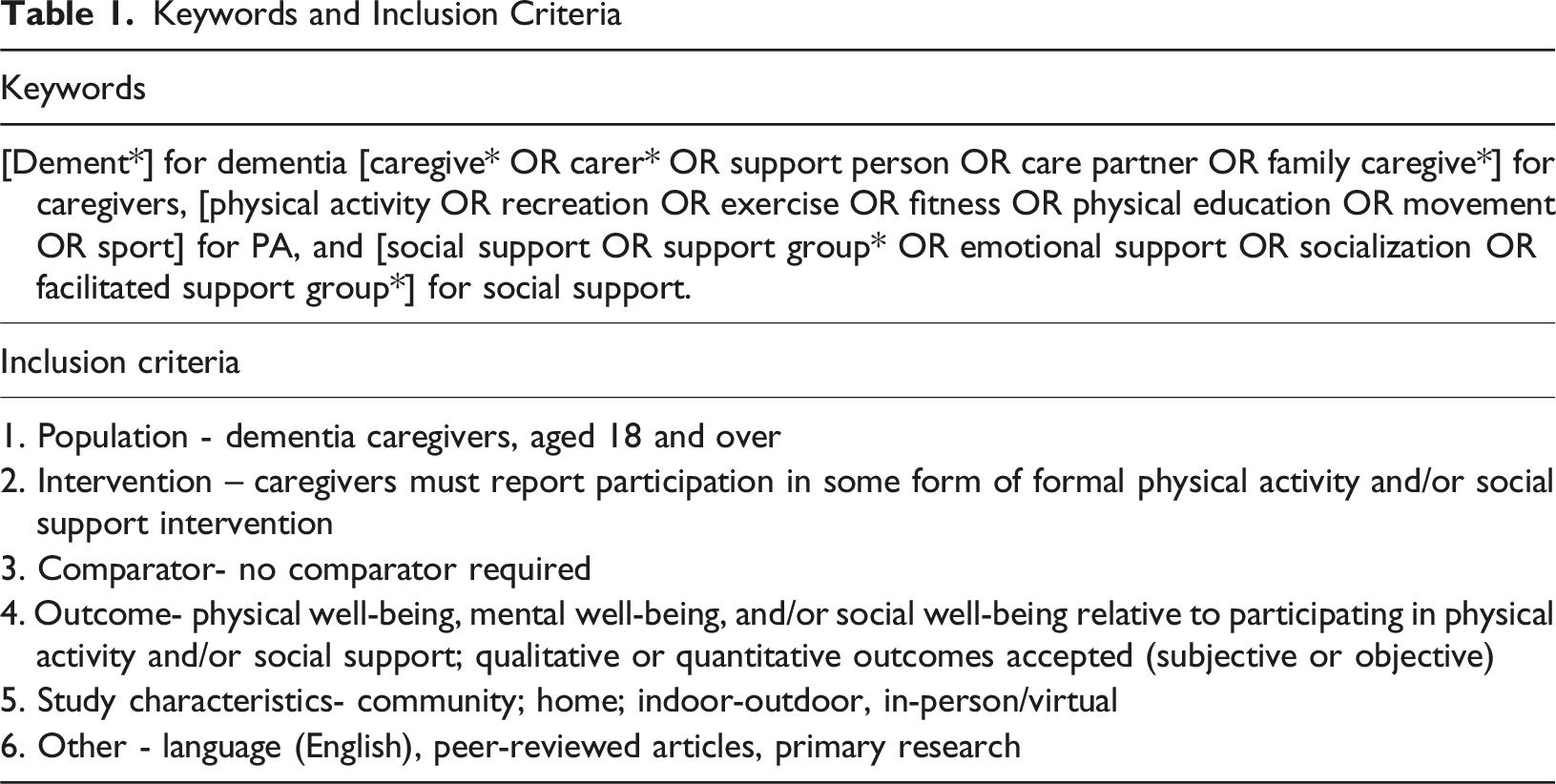
Stage 3: Study Selection
Table 1 also outlines the inclusion criteria guiding study selection. Date range was limited to studies published after the year 2000, helping to ensure only the most recent and relevant studies were included. Over the past two decades our understanding of dementia and caregiving practices have evolved, making the results of earlier studies less informative for future intervention development and enhancement (Schulz et al., 2002; Shi et al., 2020).
Titles and abstracts were screened by HO and PF. Full-text review (n = 139) was also completed by HO/PF, with a 67% agreement rate regarding inclusion/exclusion. For the conflicts, HO and PF reread the articles and discussed their individual reasons for inclusion/exclusion. PB served as the moderator during this session. If the authors still disagreed, PB made the final decision (two of which were excluded, and one was included in the final review).
Stage 4: Chart the Data
A customizable template within Covidence designed for scoping reviews was used to organize information from the included studies. Specifically, extraction was organized using the following headings: (1) general information (e.g., title, author(s)); (2) study characteristics (e.g., purpose, methods); (3) target population (e.g., population description); (4) intervention; (5) and outcome measures. All information was extracted by HO. Following initial extraction, HO revisited all papers to ensure accuracy of the information collected. Minor revisions were made, and tables were updated.
Stage 5: Collate, Summarize, and Report Results
We organized the data directly related to the four research questions. Since this was a scoping review and not a systematic review, we sought to present an overview of the findings from all relevant studies and not “synthesize the evidence or aggregate the findings” (Arksey & O’Malley, 2005, p. 27). Charts and figures were used to help summarize all relevant information. Studies were categorized based on intervention (physical activity, social support or both) and further sub-divided based on articles focused on young onset dementia, late-onset dementia, or both. Despite socialization being a natural part of any physical activity intervention, interventions were only classified as physical activity and social support if they included a structured physical activity component followed by a structured social support component or vice versa. As previously discussed, for this review we restricted our inclusion criteria to only formal social support and did not consider social support through informal social relationships. Social support gained from solely participating in physical activity would be classified as social support through informal social relationships and thus was not considered during our review. This is visually represented within Figure 1 and discussed within the results section. Visual representation of findings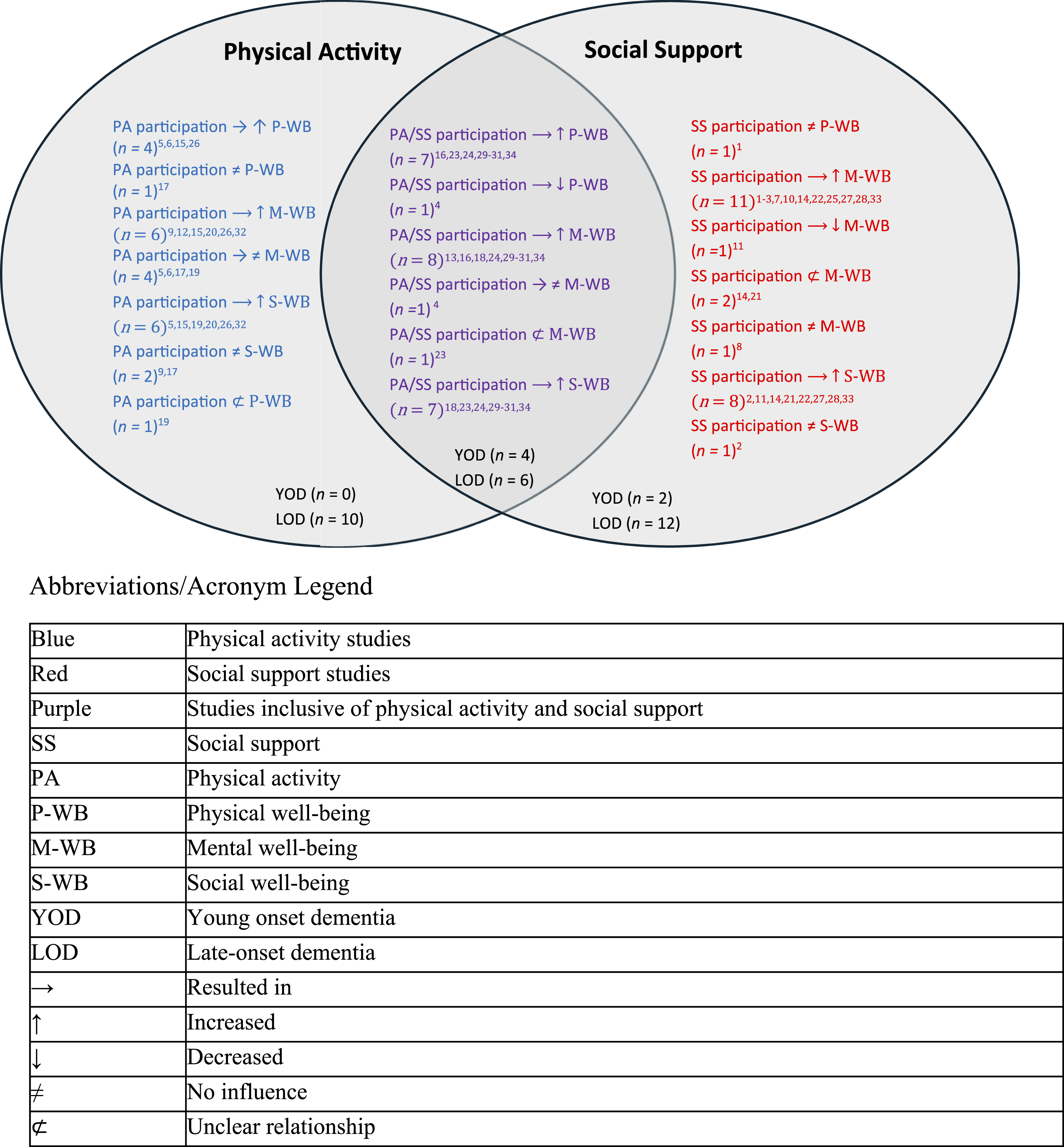
Stage 6: Ongoing Consultation
Arksey and O’Malley’s (2005) framework includes an optional consultation phase with experts in the area of research (e.g., fellow researchers, knowledge users). Four professors (including PF & PB) were consulted during this review. Two additional professors (not included as authors) were also consulted to help refine the research questions, search terms, and inclusion criteria.
Knowledge users, including dementia caregivers’ and community program providers were also consulted within a focus group. Knowledge users were eligible to participate if: (1) they lived and worked within Ontario and were 18 years or older; and (2) they were a dementia caregiver who participated in some form of physical activity and/or social support in the community; or (3) they were a community program provider who was involved in designing, implementing, or evaluating physical activity and/or social support interventions for people living with dementia and/or their family caregivers. Study information was distributed via the Alzheimer Society of Ontario’s research portal and social media (e.g., Facebook, Instagram). Individuals who consented to participate were asked if they knew of other dementia caregivers or community program providers who would be interested in participating and were asked to share study information (i.e., snowball sampling) (Patton, 2015). All participants provided informed written consent prior to participation. This consultation phase was approved by Wilfrid Laurier University office of Research Ethics (REB#8841). Four knowledge users participated in the consultation phase.
Background Questionnaire
Prior to the focus group a background questionnaire was administered online via Qualtrics. The background questionnaire was used to screen all knowledge users corresponding to the inclusion criteria. Caregivers reported demographic information (e.g., age, gender), caregiver experiences (e.g., length of time providing care, caregiving duties), health status (e.g., presence of any illnesses or impairments) and their involvement within physical activity and/or formal social support interventions. Likewise, community program providers reported demographics (e.g., age, gender, education), and their experiences as community program providers (e.g., role within their organizations and length of time they provided dementia programming). Background questionnaires provided context prior to the focus group and aided in rapport building between the primary researcher [HO] and knowledge users.
Focus Group
The focus group followed a semi-structured interview guide and was conducted via Zoom in September 2024. Interview questions explored knowledge users’ perceptions and experiences either participating in (for dementia caregivers) or designing, implementing or evaluating (for community program providers) physical activity and/or social support interventions. Part way through the focus group HO explained the findings from the scoping review via a brief PowerPoint presentation. All knowledge users were then asked how their experiences as a caregiver or community program provider compared to the results of the scoping review. All information disclosed by knowledge users during this phase of the focus group was used during the analysis section of this review. Throughout the focus group, probes were implemented when knowledge users’ responses required elaboration or when further information was warranted (Flick, 2009). Through the focus group, the researchers were able to understand if the results of the scoping review aligned with the lived experiences of the target population (i.e., health of dementia caregivers).
The focus group lasted for 57 minutes and was transcribed verbatim. Pseudonyms were used in the place of knowledge users’ names, and all identifying information was removed to help protect the anonymity of knowledge users.
Enhancing Trustworthiness and Rigour
Within the consent form, knowledge users were given the option to indicate if they would like to complete a member check. Member checks allowed participants the opportunity to “correct, amend, or extend” (Lincoln & Guba, 1985, p. 236) any of the information they disclosed during the focus group. Two knowledge users opted to complete the member check. This optional step contributed to the credibility of the results (Lincoln & Guba, 1985).
Results
The search of databases yielded 2393 articles, reduced to 2134 after the removal of duplicates. From title and abstract screening, 139 were deemed relevant and progressed to full-text review. Following full-text review, 34 articles were eligible for inclusion: 18 quantitative; 9 qualitative; and 7 mixed methods. Figure 2 visually represents this process and indicates reasons for exclusion. A PRISMA flow diagram of the study selection process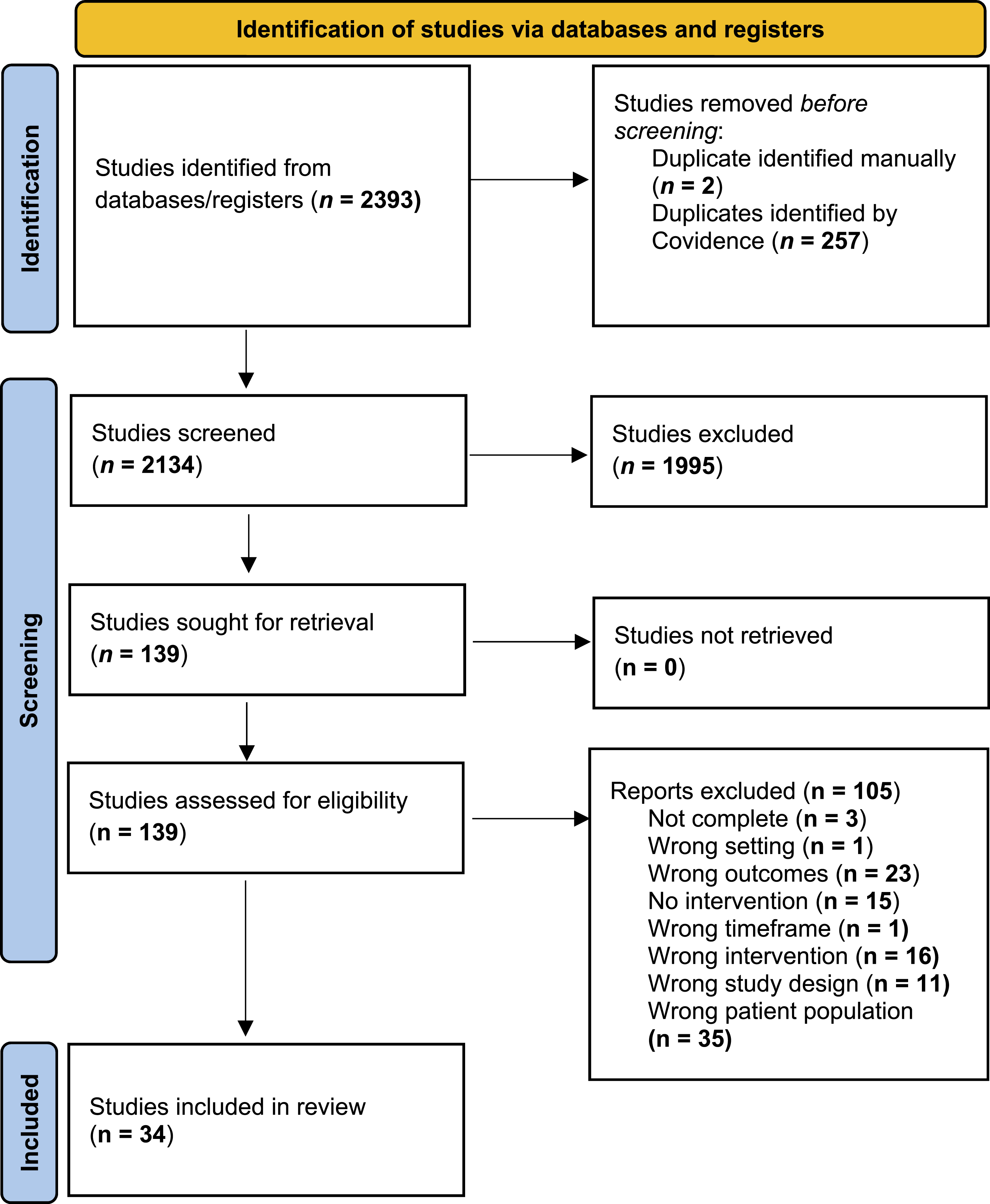
Study Demographics
General Study Information and Participant Demographics
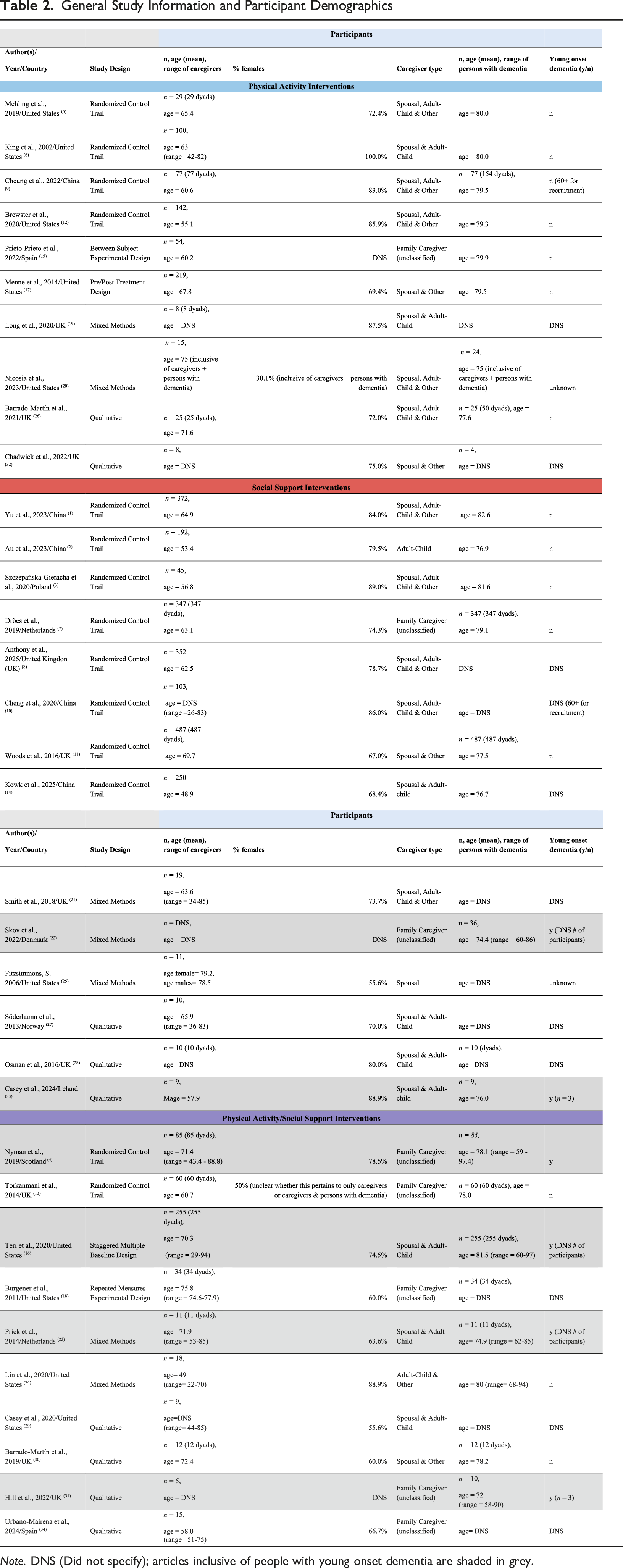
Note. DNS (Did not specify); articles inclusive of people with young onset dementia are shaded in grey.
Nineteen studies examined caregivers and people with dementia (i.e., as dyads) while 15 studies solely focused on caregivers. Nineteen studies required a clinical diagnosis of dementia, while 15 did not specify. Most studies (n = 22) included caregivers to care recipients with any type (e.g., Alzheimer’s disease, frontotemporal dementia etc.) and stage (e.g., mild, moderate, advanced) of dementia. Only one study specifically focused on caregivers for people with advanced dementia (Nyman et al., 2019), and two studies were specific to caregivers for people with Alzheimer’s disease (Au et al., 2023; Urbano-Mairena et al., 2024). One study excluded people with Lewy Body or Parkinson’s related dementia (Barrado-Martín et al., 2021), while six studies were specific to caregivers for people with mild-moderate dementia (any type). Only six studies included people with young onset dementia (Casey et al., 2024; Hill et al., 2022; Nyman et al., 2019; Prick et al., 2014; Skov et al., 2022; Teri et al., 2020); however, no studies specifically excluded those with young onset dementia and their caregivers.
Intervention Locations
Data Collection Methods and Intervention Types
Note. DNS (did not specify); HRQOL (health related quality of life); ZBI (Zarit burden interview); CES-D (center for epidemiological studies – depression); CBS (caregiver burden scale); BDI (beck depression index); BSSS (berlin social support scale); TUG (Times up and go); ICEpop CAPability (Fear of falls & quality of life measures); CBI (caregiver burden inventory); PAC (positive aspects of caregiving); GDS (geriatric depression scale); BBS (berg balance scale); LAPAQ (physical activity level questionnaire); DEMQoL (dementia quality of life scale); HADS (hospital anxiety and depression scale); PSS (perceived stress scale); CHAMPS (community health activity model program for seniors); PSQI (Pittsburg sleep quality index); NPI (Neuropsychiatric inventory); TOPICS-MDS (The older persons and informal caregivers survey minimum dataset); QCCRR (quality of the caregiving care recipient relationship); QOL (general quality of life); CCS (Caregiver competency scale); GHQ-28 (general health questionnaire – mental health); RSS (relative stress scale); QCPR (quality of the carer-patient relationship); CG-CR (elder caregiver family relationship scale); MOSS (medical outcome social support survey); PWB; (psychological well-being scale); PHQ-9 (Patient-health questionnaire); SF-12 (12-item short form health survey); ED-5D-5 L (EuroQol five-dimensional, five-level questionnaire). Articles shaded in grey are inclusive of people with young onset dementia.
Physical Activity Intervention Studies
All studies examining physical activity interventions included outcome measures to assess caregivers’ mental well-being (n = 10), with fewer studies focusing on how physical activity participation influenced caregivers’ social (n = 8) or physical well-being (n = 6). No studies included young onset dementia caregivers. Each well-being domain relative to physical activity participation is discussed below.
Physical Activity and Mental Well-Being
Physical Activity interventions varied greatly in terms of intervention design, duration, and delivery. For example, some studies assessed the participation of caregivers in a long-term (∼104 hrs to 138 hrs) home-based walking program (King et al., 2002), while others examined shorter (∼12 hrs), more vigorous, community-based cardiovascular exercises (e.g., marching, running etc.) delivered to caregivers and care recipients as dyads (Long et al., 2020). Outcome measures used to assess mental well-being also varied. Some studies examined caregivers’ anxiety or depression while others looked at perceived levels of caregiver strain. Despite this heterogeneity, most studies (n = 6) reported improvements to caregivers’ mental well-being. With respect to the four studies that saw no improvements, they all consisted of either low intensity physical activity (e.g., walking or breathing exercises) or the physical activity interventions were short in terms of duration (i.e., <13 hr of physical activity across 12 weeks). This suggests for physical activity participation to improve caregivers’ mental well-being, it may need to be of a certain intensity and maintained for a specific period.
Physical Activity and Social Well-Being
There was less variability across the physical activity interventions that assessed caregivers’ social well-being, with most interventions being community-based (n = 5) and examining the participation of caregiver-care recipient dyads (n = 6). However, like mental well-being, inconsistent measures were used to assess caregivers’ social well-being, with no two studies utilizing the same measure. Despite this, the only physical activity interventions that saw no improvements to caregivers’ social well-being, were interventions completed strictly at-home (Menne et al., 2014) or a combination of at-home and in the community (Cheung et al., 2022). This highlights that caregivers’ may need consistent in-person interactions (e.g., with other: caregivers, program facilitators etc.) for their social well-being to be improved from physical activity participation.
Physical Activity and Physical Well-Being
Interestingly, only a few studies examining physical activity interventions considered how participation influenced caregivers’ physical well-being (n = 6). Across these six studies, most reported improvements regardless of intervention design or duration (Barrado-Martín et al., 2021; King et al., 2002; Mehling et al., 2019; Prieto-Prieto et al., 2022). The only physical activity intervention reporting no improvements to caregivers’ physical well-being was an at-home exercise program inclusive of dementia education (Menne et al., 2014). However, one other study did report mixed results as qualitative findings highlighted improvements to caregivers’ physical well-being while quantitative findings reported either no improvements or a slight decline (Long et al., 2020). Nonetheless, inconsistent measures were used to assess the influence of physical activity participation on physical well-being across all studies, with no two studies utilizing the same measure. Future research is warranted to help clarify our understanding of how physical activity participation may influence the physical well-being of dementia caregivers.
Physical Activity and Young Onset Dementia Caregivers
Overall Findings
Note. Study type: Physical activity interventions (blue), social support interventions (red), both physical activity & social support (purple). Symbol legend: → (resulted in), ↑ (increased), ↓ (decreased), ≠ (no influence), ⊄ (unclear relationship); P-WB (physical well-being); M-WB (mental well-being); S-WB (social well-being); BTF (Benefit finding); HRQoL (health related quality of life); ICEpop CAPability (Fear of falls & quality of life measures); RSS (relative stress scale); QOL (quality of life); ZBI (Zarit burden interview). Articles shaded in grey are inclusive of people with young onset dementia.
Social Support Intervention Studies
Like physical activity, all studies examining social support interventions included outcome measures to assess caregivers’ mental well-being (n = 14), with fewer studies focusing on how social support participation influenced caregivers’ social (n = 9) or physical well-being (n = 2). Only two studies included young onset dementia caregivers. Each well-being domain relative to social support participation is discussed below.
Social Support and Mental Well-Being
Regardless of intervention design or duration, the majority of social support interventions reported improvements to caregivers’ mental well-being (n = 10) (Au et al., 2023; Casey et al., 2024; Cheng et al., 2020; Dröes et al., 2019; Fitzsimmons, 2006; Osman et al., 2016; Skov et al., 2022; Söderhamn et al., 2013; Szczepańska-Gieracha et al., 2020; Yu et al., 2023). Across all studies, varying assessment measures were implemented; however, most studies focused on levels of depression, anxiety, and/or quality of life. Participating in joint reminiscence groups was the only social support intervention to report a decrease in caregivers’ mental well-being (Woods et al., 2016). However, in general, social support interventions implemented remotely or virtually appeared to be less effective than community-based interventions, as a few studies exploring remote/virtual interventions reported either no change to mental well-being (Anthony et al., 2025) or inconsistent results (i.e., some measures showed improvements while others did not) (Kwok et al., 2025; Smith et al., 2018). Thus, although several studies reported improvements in caregivers’ mental well-being, not all forms or modes of social support were beneficial. Future research is needed to help clarify how social support participation influences the mental well-being of dementia caregivers.
Social Support and Social Well-being
Like mental well-being, several social support interventions (n = 8) found participation improved caregivers’ social well-being (Au et al., 2023; Casey et al., 2024; Kwok et al., 2025; Osman et al., 2016; Skov et al., 2022; Smith et al., 2018; Söderhamn et al., 2013; Woods et al., 2016), albeit varying intervention designs and measures used for assessment. Group relaxation training in combination with a facilitated support group; delivered in the community; to caregivers only, was the only intervention to report no change to caregivers’ social well-being (Szczepańska-Gieracha et al., 2020). This suggests regardless of intervention design, most social support interventions can improve dementia caregivers’ social well-being.
Social Support and Physical Well-Being
Of the 14 studies to examine dementia caregivers’ participation in some form of social support intervention, only two included measures to assess caregivers’ physical well-being (Kwok et al., 2025; Yu et al., 2023). Yu et al. (2023) examined caregivers’ participation in a community-based strengths-based intervention (∼21 hrs) which discussed topics such as strategies to handle functional loss and self-care, while Kok et al. (2025) examined caregivers’ participation in an online psychoeducation intervention supplemented by self-care skills (∼30.5 hrs). Kwok et al. (2025) reported improvements to caregivers’ physical well-being while Yu et al. (2021) reported no difference. Kwok et al. assessed caregivers’ overall physical health while Yu et al. specifically examined physical functioning. With only two studies found, it is difficult to draw conclusions about the influence of social support on dementia caregivers’ physical well-being. Future research should incorporate measures to assess physical well-being to strengthen our understanding of how social support participation may influence this aspect of dementia caregivers’ health.
Social Support and Young Onset Dementia Caregivers
Across the 14 studies examining dementia caregivers’ participation in some form of formal social support, only two included young onset dementia caregivers. This limited representation restricts our understanding of young onset dementia caregivers’ experiences and reduces the generalizability of the findings to this population. Like physical activity, future research is warranted to strengthen our understanding of how participation in formal social support interventions can influence the well-being of both young onset and late-onset dementia caregivers. For more information on the outcomes of the social support interventions see Table 4.
Physical Activity/Social Support Intervention Studies
Consistent with the studies focusing on dementia caregivers’ participation in either physical activity or social support, all studies examining interventions inclusive of both physical activity and social support included measures to assess caregivers’ mental well-being (n = 10), with fewer studies assessing caregiver’ physical (n = 8) and social (n = 7) well-being. Here four studies included young onset dementia caregivers. Again, each well-being domain relative to participating in physical activity/social support will be discussed below.
Physical Activity/Social Support, and Mental Well-Being
Regardless of intervention design or duration, majority of physical activity and social support interventions reported improvements to caregivers’ mental well-being (n = 8) (Barrado-Martín et al., 2019; Burgener et al., 2011; Casey et al., 2020; Hill et al., 2022; Lin et al., 2020; Terri et at., 2020; Torkamani et al., 2014; Urbano-Mairena et al., 2024). Across all studies, various tools were used for assessment; however, most studies (n = 6) were qualitative, meaning improvements to caregivers’ mental well-being were self-perceived. Conflicting results existed when examining the influence of Tai Chi in combination with group socialization. One study implemented a randomized control trial with structured assessment measures (e.g., Zarit Burden Interview) (Nyman et al., 2019), while another conducted focus groups with caregivers (Barrado-Martín et al., 2019). The randomized control trial reported no change to caregivers’ mental well-being while the focus groups highlighted perceived improvements. Thus, although several studies reported improvements in caregivers’ mental well-being, not all types of physical activity/social support interventions were beneficial. Future research is needed to help clarify how Tai Chi in combination with group socialization may influence dementia caregivers’ mental well-being.
Physical Activity/Social Support, and Social Well-Being
Regardless of intervention design or duration, all physical activity/social support interventions assessing caregivers’ social well-being reported improvements (Barrado-Martín et al., 2019; Burgener et al., 2011; Casey et al., 2020; Hill et al., 2022; Lin et al., 2020; Prick et al., 2014; Urbano-Mairena et al., 2024). Across these studies, there was more consistency in assessment methods utilized, with most (n = 6) conducting interviews or focus groups with caregivers. Only one study (Burgener et al., 2011) assessed caregivers’ social well-being using a standardized assessment tool. Future research should focus on quantifying the relationship between physical activity/social support participation and dementia caregivers’ social well-being to strengthen our understanding of how such interventions influence this aspect of caregivers’ health.
Physical Activity/Social Support, and Physical Well-Being
Most physical activity/social support interventions assessing the physical well-being of caregivers’ reported improvements following participation (n = 6) (Barrado-Martín et al., 2019; Casey et al., 2020; Hill et al., 2022; Prick et al., 2014; Terri et al., 2020). However, like the findings relative to mental well-being, conflicting results existed when examining the influence of Tai Chi in combination with group socialization. Nyman et al. (2019) reported a decrease in caregivers’ physical well-being following participation in Tai Chi/group socialization, whereas Barrado-Martín et al. (2019) reported improvements. While the interventions did not differ in location, they varied in duration and frequency. The longer duration and higher frequency in Nyman et al.’s (2019) intervention may suggest the benefits of Tai Chi/group socialization on dementia caregivers’ physical well-being may not be sustained long-term. Further, Nyman et al. (2019) included young onset dementia caregivers, whereas Barrado-Martín et al. (2019) did not. This disparity may have contributed to the difference in results. Nonetheless, with only two studies examining Tai Chi/group socialization, it is challenging to draw conclusions. Future research is warranted to help clarify how Tai Chi/group socialization influences the physical well-being of dementia caregivers.
Physical Activity/Social Support and Young Onset Dementia Caregivers
Across the 10 studies examining physical activity/social support interventions, four included caregivers for persons with young onset dementia. Physical activity/social support interventions had the greatest representation of young onset dementia caregivers; however, within the individual studies the representation of young onset dementia caregivers was small, and results were reported as one (i.e., young onset dementia caregivers with late-onset dementia caregivers). Like physical activity and social support interventions, future research is warranted to strengthen our understanding of how participation in physical activity/social support can influence the well-being of both young onset and late-onset dementia caregivers. For more information on the outcomes of the social support interventions see Table 4.
Consultation with Knowledge Users
A focus group was conducted online via Zoom with one dementia caregiver and three community program providers (from here on referred collectively to as knowledge users). All knowledge users were women with a mean age of 47, ranging in age from 33 to 61 years. The dementia caregiver provided care to her husband living with vascular dementia and had been a caregiver for five years. A second dementia caregiver had been recruited to participate but did not attend the focus group, despite completing the informed consent and background questionnaire. The community program providers worked for a variety of organizations specialized in dementia care and had experience implementing several physical activity and social support interventions designed for persons with dementia and their caregivers. On average the community program providers had experience working with people with dementia and caregivers for 17.3 years, ranging from three to 37 years. All knowledge users were from Southern Ontario.
Following the semi-structured interview guide, knowledge users were asked to share their perceptions and experiences (a) participating in physical activity and social support or (b) designing, implementing, or evaluating physical activity and social support for people with dementia and caregivers. In terms of physical activity, all three community program providers gave examples of the benefits of physical activity for their clients with dementia and caregivers. One community program provider emphasized participating in physical activity serves as ‘respite’ time for caregivers allowing them to ‘take a deep breath and go on to tomorrow’. The caregiver stated ‘it [physical activity] does make a huge difference’; however, then went on to explain that for both her and her husband with dementia ‘the social aspect of exercise and games…. Are probably much more important than the actual physicality of it’. This was consistent across all knowledge users, with knowledge users emphasizing social support was ‘so key’ for anyone influenced by dementia.
HO outlined the results of the scoping review and asked knowledge users how their experiences compared to the results (e.g., similar, different, agree, disagree). All knowledge users agreed with most findings; but were surprised by some and keen to discuss their varying experiences. For example, within the review one study found joint reminiscence groups decreased mental well-being (Woods et al., 2016). This surprised the knowledge users who were community program providers as they had implemented reminiscence groups in the past and had always received positive feedback from their clients. The knowledge user who was a caregiver discussed her experience in a support group and stated ‘they [dementia caregivers] found it very overwhelming and not at all supportive…reminiscing can be very challenging to some people’. The three community program providers appreciated the caregiver sharing her experience and were then able to recognize how reminiscing may not be beneficial for caregivers. The caregiver further suggested if the measurements were taken too close to the individual reminiscence sessions it may have influenced the results. She believed for social support to be effective it needs to occur long-term and thus data should be collected beyond just a ‘six’ or ‘twelve’ week period. This conversation regarding intervention length continued when discussing the benefits of physical activity. Again, the caregiver emphasized the importance of duration, and that for physical activity to be effective she needed to reach a certain threshold and continue to participate long-term. All knowledge users were curious as to why one article found Tai Chi participation led to decreased physical well-being and looked forward to future research to better understand this finding.
Discussion
This scoping review examined 34 peer-reviewed research articles resulting in several important findings. Regardless of intervention type (physical activity, social support or both) the most common finding was participation enhanced caregivers’ mental well-being. In considering physical activity interventions, in-person interactions may be essential for caregivers to experience benefits to their social well-being. However, no difference was found between the influence of physical activity and/or social support interventions on the physical and mental well-being of caregivers when comparing interventions delivered within the community versus interventions completed at home or over-the-phone. Finally, there is a lack of research within North America regarding community-based physical activity and/or social support interventions, with most research examining interventions within Europe.
Putting the Research into Context
There are limitations of the current review, first and foremost only studies published in English were included and thus may not be generalizable to other cultural contexts. Next, studies were not excluded based on quality, since a scoping review’s purpose is to simply identify research and not conduct a quality assessment. However, some weaker study designs were included and thus quality should be considered before applying these findings to community-based interventions for dementia caregivers. Further, although authors HO and PF followed a series of rigorous steps to ensure all relevant articles were included within this review; it is possible some studies were missed due to limitations within the databases and search terms selected. This review was also restricted to only articles published after the year 2000 which may have biased the results.
A few limitations arose from the included studies. Namely, some studies solely focused on dementia caregivers, while others explored participation of caregivers and people with dementia (i.e., as dyads). This may have influenced the effect of the intervention on dementia caregivers’ health, since the results were often reported in relation to both caregivers and people with dementia. Further, intervention type, duration, location, and frequency varied from study to study, complicating the direct comparison between interventions. Qualitative and quantitative studies were also included which further complicated this comparison. In terms of participants, most studies were inclusive of all family caregivers, to persons of any age, living with any stage, and form of dementia; however, only six studies were successful in recruiting young onset dementia caregivers. Due to the increased health effects experienced by young onset dementia caregivers (Hvidsten et al., 2020; Kimura et al., 2021), future research should specifically explore the effects of physical activity and/or social support on the health of this population. Understanding this relationship may guide the development of specific resources designed to mitigate the health effects experienced by young onset dementia caregivers.
Participation in Physical Activity and/or Social Support and the Health of Dementia Caregivers
Despite limitations, this review provides valuable insight into what is known about dementia caregivers’ health and participation within (a) physical activity, and/or (b) social support. This is one of the first reviews to examine physical activity and/or social support participation on the health of dementia caregivers, despite the increased awareness surrounding the support needs of this population. Overall, we found social support interventions to have the greatest influence on the mental well-being of dementia caregivers, which is plausible due to the direct association between the benefits of social support and the health effects experienced by dementia caregivers (Harandi et al., 2017; Vitaliano et al., 2003; Zhang et al., 2006). This finding was supported by all consulted knowledge users and is consistent with previous research (Dam et al., 2016). Only two studies examining social support included measures to assess physical well-being, one of which found no effect (Yu et al., 2023) and the other having a positive influence (Kwok et al., 2025). In general, social support has been found to be one of the most well-documented psychosocial factors influencing the physical well-being of adults (Berkman et al., 2000; Uchino, 2009). This relationship should be investigated further due to the (1) existing conflicting results, and (2) lack of studies considering the influence of social support participation on the physical well-being of dementia caregivers.
From this review, the influence of physical activity on the physical well-being of dementia caregivers was unclear. First, of the 10 studies focused on physical activity, only six studies included measures to assess physical well-being. Second, physical activity interventions varied in design and duration, with limited studies including a follow-up period. Within the consultation phase, one knowledge user emphasized the importance of physical activity duration on the health benefits she experiences as a caregiver. Due to the lack of studies to assess physical well-being, future research should continue to explore this relationship and consider duration as a factor during analysis. Finally, all studies that found physical activity participation to have no influence on the physical well-being of dementia caregivers examined people with dementia and caregivers as dyads, with results corresponding to both populations. Research regarding caregivers for adults with other physical and mental health conditions has found physical activity to be effective in improving health (Marshall et al., 2022). It would be worthwhile for future research to report the results of caregivers and people with dementia separately to strengthen our understanding of the influence of physical activity participation on caregivers’ health.
Consistent with the results of Orgeta and Castillo’s (2014) review, no studies found physical activity participation to influence the anxiety levels of dementia caregivers. However, three studies exploring interventions inclusive of physical activity and social support did find participation resulted in reduced anxiety (Burgener et al., 2011; Terri et al., 2020; Torkanmani et al., 2014). Thus, for physical activity to be effective in reducing caregivers’ anxiety it may need to be implemented alongside a social support intervention. Contrary to Orgeta and Castillo (2014), three studies found physical activity contributed to decreased levels of depression and stress (Brewster et al., 2020; Chadwick et al., 2022; Nicosia et al., 2023). Future research should continue to explore the influence of physical activity participation, and the levels of depression and stress experienced by dementia caregivers to help clarify this relationship.
When considering overall health, interventions inclusive of physical activity and social support were found to be the most effective. Only one study found participation to have a negative influence. Nyman et al. (2019) explored Tai Chi in combination with socialization and found participation to have a negative influence on caregivers’ physical well-being and no influence on caregivers’ mental well-being. Knowledge users within the consultation phase of this review were curious as to why this occurred and anecdotally had never found physical activity participation to decrease physical well-being, either for themselves or their clients. Barrado-Martín et al. (2019) also examined caregivers’ participation within Tai Chi/group socialization and found participation to have a positive influence on caregivers physical, mental, and social well-being. However, it is important to recognize Barrado-Martín assessed caregivers qualitatively within interviews, whereas Nyman et al. utilized quantitative assessments. Future research, inclusive of qualitative and quantitative assessments should continue to explore Tai Chi in combination with socialization to help clarify the current discrepancy in results.
Implications for Future Research & Practical Implications
This scoping review points to several important directions for future research and practical implications. It is essential for physical activity interventions to include a follow-up period to better understand the long-term influence of participation. Duration and intensity should be reported allowing for greater comparison between intervention types. Interventions inclusive of caregivers and people with dementia would benefit from reporting the results of both populations separately. This would help further our understanding of the influence of physical activity and/or social support participation on caregivers and people with dementia individually. Equally, studies examining social support interventions should include measures to assess physical well-being, since social support has been found to have benefits on the physical well-being of other populations (Uchino, 2009).
We found a general lack of intervention studies exploring young onset dementia caregivers and dementia caregivers who are men. Young onset dementia caregivers often experience increased negative health effects (Hvidsten et al., 2020; Kimura et al., 2021), and thus the results of this review may not be transferable to this population. In general men are less likely to participate in social support initiatives (Greenwood & Smith, 2015) and therefore, the results of this review may not be transferable to dementia caregivers who are men since most studies within this review included primarily women caregivers. Future research should focus on young onset dementia caregivers and caregivers who are men to help fill this gap in understanding.
In terms of practical implications, online or at-home delivery appears to be equally effective for physical and mental well-being and may create enhanced possibilities for delivering physical activity and/or social support interventions to a greater number of dementia caregivers. A previous review has highlighted that online interventions can reduce symptoms of depression, anxiety, and stress among caregivers, while simultaneously enhancing their coping mechanisms and perceived self-efficacy (Leng et al., 2020). Similarly, Ye et al. (2025) review reported virtual app-based interventions can foster self-competence and promote social engagement among people with dementia and their caregivers in their systematic review on App features, security, and useability. However, despite the recognized benefits of online or at-home interventions this approach may cause for increased safety concerns and may not be appropriate for marginalized populations, such as individuals living in rural communities or of a lower socio-economic status as these populations may not have access to the tools required to participate online (e.g., sufficient internet access, knowledge on how to access online programs etc.) (Al-Dhahir et al., 2022). The use of reminiscence therapy within social support interventions should be implemented with caution due to the negative influence found within the literature and expressed by knowledge users within the consultation phase of this review. Future research should continue to explore reminiscence therapy in the context of people with dementia and caregivers to help clarify its influence on the health of both populations.
Conclusions
In summary, this scoping review provides insight into the influence of physical activity and/or social support and the health of dementia caregivers. From the review, it is evident participation in physical activity and/or social support is beneficial for the physical, mental and social well-being of dementia caregivers. The findings from this review should be used to help inform the development and improvement of community-based interventions for dementia caregivers.
Footnotes
Acknowledgements
Thank you to Dr. Carrie McAiney and Dr. Mark Eys for their continuing support and guidance throughout this project.
Ethical Approval
The consultation phase of this study was approved by the research ethics board at Wilfrid Laurier University (REB #8841). All participants provided informed consent prior to participation within the focus group.
Author Contributions
HO is the main author of this paper. She did all data extraction and most of the writing. PF and PB contributed to the design of the study and were involved during study selection. All authors were involved in the writing of the paper.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Centre for Healthy Communities [CHC] and by a SSHRC Doctoral Fellowship (752-2023-2823).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The qualitative data supporting the findings associated with consultation phase of this study are not publicly available due to privacy restrictions.