
Abstract
The positive physical, mental, and cognitive health effects of social participation in late life have been well established. However, the facilitators and barriers of social participation among older adults with dementia and the effects of social participation on their psychological well-being have been understudied. Using the cross-sectional 2023 National Health and Aging Trends Studies (N = 7,547; 13.2% of them classified as having possible or probable dementia), we examined the correlates of social participation among older adults with dementia, compared to those among their peers without dementia, the moderating effect of dementia on the associations between social participation and psychological well-being, and the mediation effects of SSNS and depressive/anxiety symptoms on the associations between social participation and psychological well-being among older adults with dementia. Results from linear regression models show negative associations between dementia and social participation (B [SE] = −0.36 [0.07], t = −5.38, p < .001 for possible dementia; B [SE] = −0.31 [0.09], t = −3.42, p = .001 for probable dementia). However, regardless of dementia status, higher education, larger social network, greater neighborhood social cohesion, and engagement in exercise were facilitators of social participation. Perceived health-related and transportation barriers and vision impairment among those with dementia were barriers to social participation. The positive association between social participation and psychological well-being (B [SE] = 0.18 [0.01], t = 13.01, p < .001) was not moderated by dementia status, although both possible and probable dementia were independently negatively associated with psychological well-being. Path model results show that among older adults with dementia, increased social network size (ratio of indirect to total effects = 0.13) and reduced depressive/anxiety symptoms (ratio of indirect to total effects = 0.17) mediated the association between social participation and psychological well-being. Implications of the findings for enhancing social participation among older adults with dementia are discussed.
Keywords
Introduction
Extensive research has shown that social participation, encompassing involvement in interpersonal interactions and community-based activities and meetings, is a significant contributor to maintaining physical and mental health in later life (Dehi Aroogh et al., 2020; Douglas et al., 2017). For example, although different types of social participation may have different effects, social participation in general has been associated with a lower likelihood of disability onset (Fujii et al., 2024; Tomioka et al., 2017); a higher likelihood of physical activity and other health-promoting behaviors, including protection against smoking in the U.S. and U.K. samples, through greater social support and social integration (Abe et al., 2022; Gyasi et al., 2021; Luo et al., 2020; Nishio et al., 2021; Sasaki et al., 2021; Wu & Sheng, 2019); better overall health outcomes and longevity, with little effect coming from educational attainment (Rueda-Salazar et al., 2021); a lower risk of loneliness and depressive symptoms (Chiao et al., 2011; Jiang et al., 2025; Zhao et al., 2023); and higher life satisfaction and quality of life directly and also through the mediating roles of loneliness, depression, anxiety, and cognitive function (Liang, 2024; Lv et al., 2024).
Longitudinal studies have indeed found that social participation predicts cognitive health (memory and executive function) over time, and the relative magnitude of this effect is comparable to the effects of physical health, depression, and physical activity (Bourassa et al., 2017). A review of systematic reviews of observational study evidence has shown that greater social participation in mid and late life is associated with a 30%–50% lower risk of subsequent dementia (Sommerlad et al., 2023). The authors noted that lifetime social participation may affect dementia risk by increasing cognitive reserve and through brain maintenance, which involves reducing stress and improving cerebrovascular health. A meta-analysis confirmed that strong social engagement and frequent social contact were positively associated with decreased risk of dementia (Wang et al., 2023). The 2024 Lancet Commission on Dementia Prevention and Intervention also identified increased social contact through participation in social activities as having a potentially beneficial effect on dementia risk, by building cognitive reserve, promoting healthy behaviors, and reducing stress and inflammation (Livingston et al., 2024).
A growing body of research, including the studies summarized above, has illustrated that the physical, mental, and cognitive health benefits of social participation in later life are mediated through expanded social networks, enhanced social connections, reduced social isolation, and increased instrumental and emotional support. The positive effects of social participation also arise from the physiological and psychological benefits associated with engaging in functional tasks and enjoyable activities (Bath & Deeg, 2005; Flatt & Hughes, 2013; Gardner et al., 2022; Maier & Klumb, 2005). Given emerging evidence on the neurobiological links between social isolation, loneliness, and the onset and progression of dementia (Drinkwater et al., 2022; Oliva et al., 2023; Shafighi et al., 2023; Ávila-Villanueva et al., 2022), social participation as a protective factor against social isolation and loneliness represents a critical, modifiable target for dementia prevention and mitigation. These findings underscore the need to identify both facilitators and barriers to social participation among older adults at varying stages of dementia.
Among older adults in general, research has identified several factors that facilitate initiating and maintaining meaningful social engagement, including personal motivation, existing social networks, and neighborhood social cohesion (Townsend et al., 2021). Qualitative studies further suggest that technology use, including among older adults with dementia, can enhance social participation, as opportunities for engagement are increasingly mediated through digital platforms (Gaber et al., 2020; Heins et al., 2021; Pinto-Bruno et al., 2017). Conversely, common barriers to social participation include physical and sensory impairments (e.g., illness, disability, vision and hearing loss), diminished social connections, lack of a supportive or inclusive community, limited access to acceptable social opportunities, and fears of social rejection or exploitation (Cimarolli et al., 2017; Goll et al., 2015; Jin et al., 2019; Zhao et al., 2023).
Among older adults living with dementia, social participation, particularly outside the home, tends to decline as the disease progresses (Chaudhury et al., 2021; Hackett et al., 2019; Thalén et al., 2022). Social withdrawal among these older adults often stems from several factors, including shame and embarrassment as well as fears and experiences of social exclusion, discreditation, and discrimination, when cognitive, emotional, and functional impairments begin to interfere with their ability to maintain social roles and meaningful relationships (Aldridge et al., 2019; Biggs et al., 2019; Birt et al., 2020; Farina et al., 2023; Kłosińska & Leszko, 2024; Singleton et al., 2017; Trindade et al., 2023). In addition to shame and fear, dementia-related behavioral changes, such as apathy, disinhibition, and agitation, can contribute to the avoidance of social interaction and withdrawal from social participation (Hackett et al., 2019; Lozupone et al., 2024).
Despite the importance of supporting social participation among older adults with dementia, limited research has been done on the barriers, facilitators, and the impact of social participation on their psychological well-being. Prior studies have identified loneliness, depression, anxiety, and cognitive function as mediators of the relationship between social participation and life satisfaction or quality of life in the general older adult population (Liang, 2024; Lv et al., 2024). However, the mediating role of these factors in the association between social participation and psychological well-being among older adults living with dementia has not been examined.
In this study, using a nationally representative sample of U.S. Medicare beneficiaries, we addressed the following sequential research questions: (1) What factors are associated with social participation among older adults with possible or probable dementia, and how do these factors compare to those of older adults without dementia? Guided by prior research summarized above, we examined several potential correlates: self-reported health or transportation barriers, sociodemographic characteristics, physical and functional health, vision and hearing impairments, depressive/anxiety symptoms, social support network size (SSNS), perception of neighborhood social cohesion, health behaviors (smoking and exercise), and online social networking site use. (2) Does the presence of possible or probable dementia attenuate the association between social participation and psychological well-being, after accounting for SSNS and depressive/anxiety symptoms? (3) Among older adults with dementia, to what extent is the positive association between social participation and psychological well-being mediated by SSNS and depressive/anxiety symptoms, controlling for dementia type (possible vs. probable)? Figure 1 provides the conceptual framework for the mediation analysis. Conceptual Framework of the Associations Among Social Participation, Social Network, Depression/Anxiety, and Psychological Well-Being. +: Positive Association. -: Negative Association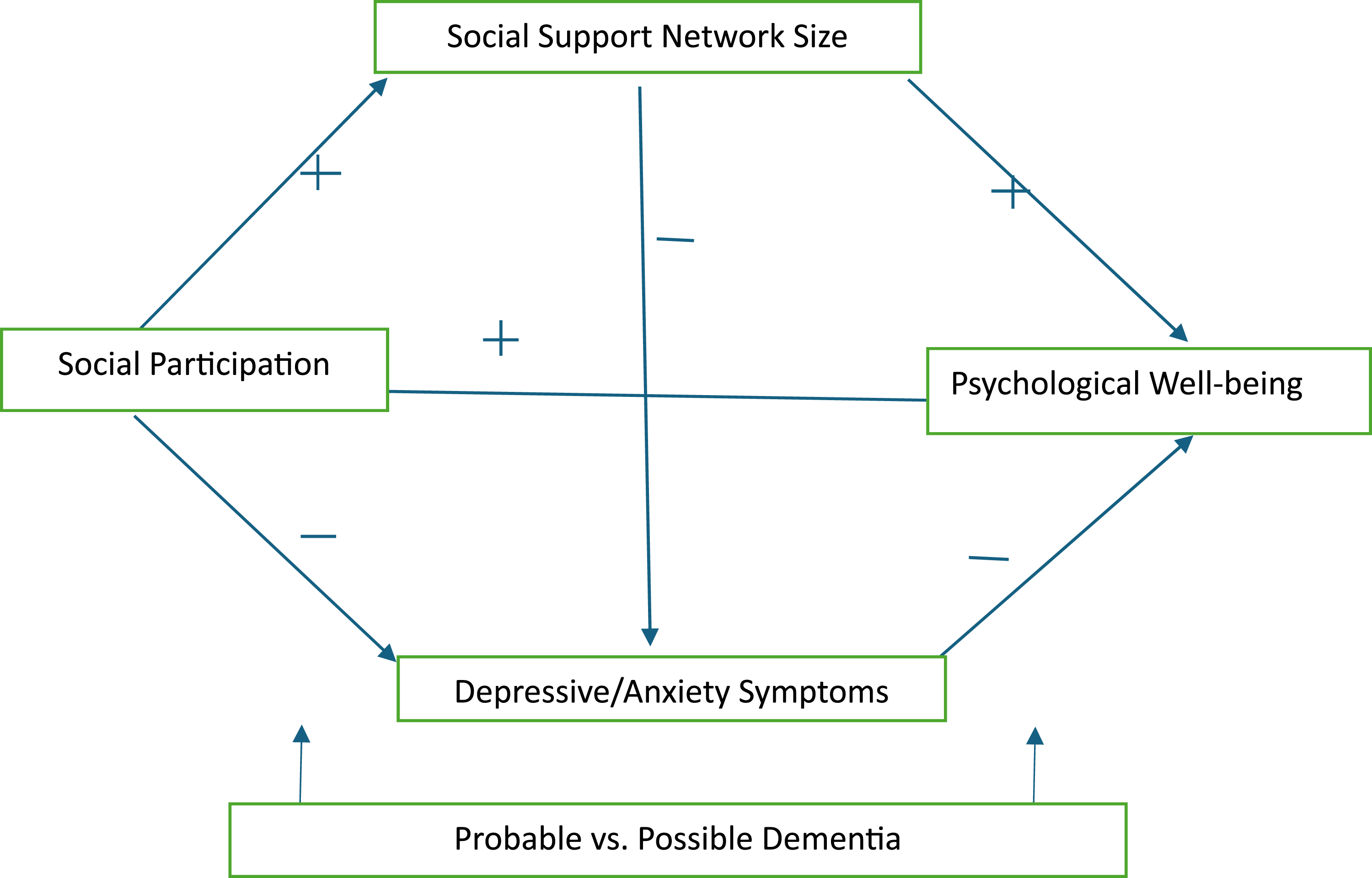
The findings regarding barriers and facilitators of social participation among older adults with dementia, the associations between social participation and psychological well-being, and the mediating effects of SSNS and depressive/anxiety symptoms will be valuable for guiding programs or strategies to enhance social participation among these older adults.
Methods
Data and Sample
Data came from the 2023 National Health and Aging Trends Study (NHATS), which collects data annually from a nationally representative panel of Medicare beneficiaries ages 65 and older (designated as “sample persons”) on their physical, functional, cognitive, and sensory capacities; social, physical, and technological environments; and participation in valued activities. In this study based on the 2023 cross-sectional data, after excluding 390 sample persons (of whom 16 had possible and 340 had probable dementia) who were proxy-interviewed, we focused on 7,547 sample persons residing in their own homes or residential care communities (but not in nursing homes). The NHATS did not collect data on the psychological well-being of the sample persons from their proxy respondents. This study, based on the analysis of de-identified public-use data, was exempt from review by the authors’ institutional review board.
Measures
Dementia status (no dementia, possible dementia, and probable dementia) was determined using the most recently updated NHATS dementia classification algorithm based on two types of information for self-respondents: (1) doctor diagnosis of dementia or AD (yes or no); and (2) scores from cognitive tests evaluating the sample person in the following three domains: memory (immediate and delayed 10-word recall), orientation (date, month, year, and day of the week; naming the President and Vice President), and executive function (clock drawing test). A possible dementia classification was assigned when the person scored ≤ 1.5 SD below the mean in one domain of the cognitive test. A probable dementia classification was assigned when the person was diagnosed with dementia or scored ≤1.5 standard deviations (SD) below the mean in at least two domains of the cognitive tests. Thus, possible dementia is a classification of less severe cognitive impairment than probable dementia. The score cut points for ≤1.5 SDs below the mean on NHATS cognitive domains were ≤3 for memory (score range 0 to 20), ≤3 for orientation (score range 0 to 8), and ≤1 for executive function (score range 0 to 5) (Kasper et al., 2013).
Social participation: This was assessed by the number of the following six social or community activities that the sample person engaged in during the past month: (a) visits with family/friends; (b) religious service attendance; (c) participation in clubs, classes, or other organized activities aside from religious services; (d) working for pay; (e) volunteering; and (f) going out to dinner, a movie, gambling, or to hear music or see a play (i.e., going out for enjoyment). The number ranged from 0 to 6.
Health and transportation barriers to social participation: After each of the social participation questions, the sample persons were asked if (a) health and functioning problems (“In the last month, did your health or functioning ever keep you from doing this [activity]?”), and (b) transportation problems (“In the last month, did a transportation problem ever keep you from doing this [activity]?”). Response options were yes or no. We defined health-related barriers as a positive “health and functioning problem” response to any of the six types of activities (yes = 1, no = 0) and transportation barriers as a positive “transportation problem” response to any of the four types of activities (yes = 1, no = 0), excluding working for pay and volunteering. The NHATS did not ask about transportation barriers for the latter two activities. In this study, we created a 4-category variable: no barrier, health-related barriers only, transportation barriers only, and both health and transportation barriers.
Psychological well-being: In NHATS, this was assessed with the following four items: (a) My life has meaning and purpose; (b) I feel confident and good about myself; (c) I gave up trying to improve my life a long time ago; and (d) I like my living situation very much. The response categories were: 1 = agree not at all, 2 = agree a little, and 3 = agree a lot. These items were similar to those of the Psychological Well-being Scale used in the National Survey of Midlife Development in the United States (MIDUS II) (Freedman et al., 2024; Ryff & Singer, 1996). In this study, we used the combined scores of the four items after reverse coding item (c) (range 3-12). The unweighted Cronbach’s alpha for the four items for the study sample was .56.
Sociodemographic factors: These included age (65-74 [reference category], 75-84, 85+); gender (female vs. male); race/ethnicity (non-Hispanic White [reference category], non-Hispanic Black, Hispanic, all other); residential type (care community vs. own home); education (bachelor’s degree or higher vs. no degree); and low-income status (family income < $43,000 vs. all other categories).
Physical, functional, and sensory health: These were measured with (a) the number of chronic medical conditions (0-8: arthritis, cancer, hypertension, heart disease, stroke, diabetes, lung disease, osteoporosis); (b) activity-limiting chronic pain (yes or no); (c) vision impairment (i.e., cannot see well across the street with or without glasses); and (d) any hearing impairment (with or without hearing aid).
Depression/anxiety symptoms in the past month: In NHATS, depression/anxiety symptoms were assessed with the Patient Health Questionnaire-4 (PHQ-4) (Kroenke et al., 2009). The PHQ-4 includes the first two items (PHQ-2; had little interest or pleasure in doing things, and felt down, depressed, or hopeless) from the 9-item PHQ-9 for depression (Kroenke et al., 2003) and the first two items (GAD-2; felt nervous, anxious, or on edge, and have been unable to stop or control worrying) from the 7-item Generalized Anxiety Disorder Scale (Spitzer et al., 2006). Responses to each PHQ-4 item were based on a 4-point scale (0 = not at all; 1 = several days; 2 = more than half the days; 3 = nearly every day), with the total score ranging from 0 to 12. The unweighted Cronbach’s alpha for the PHQ-4 for the study sample was .77. The PHQ-4 scores were also used to categorize the symptom severity: no symptom (0-2), mild symptoms (3-5), and moderate/severe symptoms (6-12) for descriptive purposes (Kroenke et al., 2009).
Social support network size (SSNS): The sample persons were asked about “who you talk to about important things in your life. This may include good or bad things that happen to you, problems you are having, or important concerns you may have.” Each sample person could list up to five individuals, including their gender and the nature of their relationship to the sample. We used the number of those whom the sample person listed (0-5) in this study.
Online social networking site visit: The sample persons were also asked if they had visited social network sites on the Internet in the past month (yes or no), including sites where they could “keep in touch with friends, such as Facebook or LinkedIn.”
Perception of neighborhood social cohesion: This was assessed using a total score derived from three items—people in this community know each other very well, are willing to help each other, and can be trusted—each rated on a 3-point scale (0 = do not agree, 1 = agree a little, and 2 = agree a lot). These items were adopted from the social cohesion scale originally developed by Sampson (1997). “Community” in NHATS was defined as “the community where the sample person lives.” In previous NHATS-based studies (e.g., Qin et al., 2024), the community was equated to the sample person’s neighborhood. The score ranged from 0 to 6. Unweighted Cronbach’s alpha for the 3-item scale was .76.
Health-related behaviors: These were assessed with: (a) past-month physical activity/exercise (yes or no) based on two NHATS’ exercise variables: walking for exercise, or spending time on vigorous activities such as working out, swimming, running, biking, or playing a sport; and (b) current smoking status (yes or no).
Analysis
All analyses were conducted using Stata/MP 19.5’s svy function (College Station, TX) to account for NHATS’s stratified, multistage sampling design. First, we employed χ2 and one-way ANOVA to describe and compare all study variables by dementia status (no dementia, possible dementia, and probable dementia). We then applied χ2 and t tests to compare the two dementia groups. Second, to address the first research question (correlates of social participation and potential differences by dementia status), we estimated three linear regression models—one for the full sample, one for individuals without dementia, and one for those with possible or probable dementia—with social participation as the dependent variable. Variance inflation factor diagnostics, using a cut-off of 2.50 (Allison, 2012), indicated that multicollinearity among covariates was not a concern. Third, to address the second research question (association between social participation and psychological well-being), we fitted linear regression models for the full sample, with psychological well-being as the dependent variable. We used interaction terms between social participation and dementia status to assess the moderating effect of dementia status, specifically, whether the strength or direction of the associations between social participation and psychological well-being differed by cognitive status. The results of all the above linear regression models are reported as unstandardized coefficients (B) and linearized standard errors (SE) with 95% confidence intervals (CI). Fourth, to address the third research question (mediation effects of SSNS and depressive/anxiety on the association between social participation and psychological well-being among individuals with dementia), we fitted a path model. Direct and indirect (mediated) effects are reported as B, SE, and 95% CI. To test the statistical significance of the two mediators, we bootstrapped (10,000 repetitions) indirect effect estimates and their 95% CIs. We calculated the proportions of the indirect effects relative to the total effects (the direct effects of social participation on psychological well-being plus the indirect effects of the mediators) and the ratios of the indirect effects to the direct effects. Note that, given the cross-sectional data, while we use terms such as direct and indirect effects from the mediation literature, we do not infer causal relationships, but the findings reflect associations.
Results
Social Participation, Psychological Well-Being, and Other Characteristics by Dementia Status
Social Participation, Psychological Well-Being, and Other Characteristics of Older Adults by Dementia Status
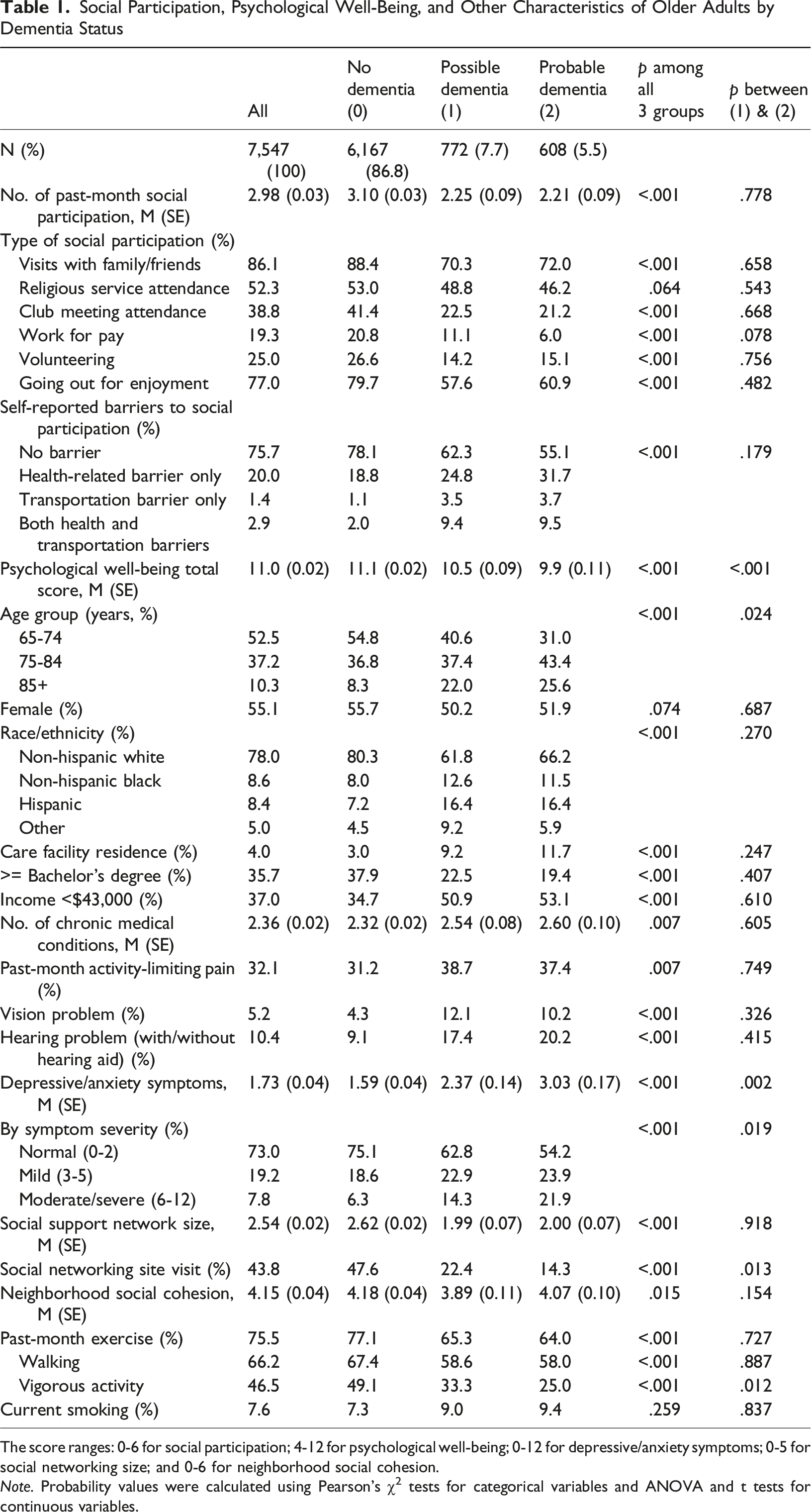
The score ranges: 0-6 for social participation; 4-12 for psychological well-being; 0-12 for depressive/anxiety symptoms; 0-5 for social networking size; and 0-6 for neighborhood social cohesion.
Note. Probability values were calculated using Pearson’s χ2 tests for categorical variables and ANOVA and t tests for continuous variables.
Compared to individuals without dementia, those with dementia were older and included higher proportions of racial/ethnic minorities, care facility residents, and individuals with annual incomes below $43,000. They also exhibited poorer physical, functional, sensory, and mental health; had a smaller social network, reported lower perceived neighborhood social cohesion; and included lower proportions of those who visited online social networking sites and engaged in physical activity. Smoking did not differ by dementia status. Individuals with probable versus possible dementia had higher levels of depressive/anxiety symptoms, with nearly 22% experiencing moderate to severe symptoms, and were less likely to visit social networking sites. Among the two dementia groups, individuals with probable dementia were older, had higher depressive/anxiety symptoms, and were less likely to visit social network sites and engage in vigorous activities. Additional analysis showed that among those with dementia, a higher proportion of care community residents than those living in their own homes reported health and/or transportation barriers (41.7% vs. 23.6%, F (2.90, 162.64) = 28.63, p < .001 for all; 53.4% versus 39.2%, F (2.94, 164.87) = 5.83, p < .001 for individuals with possible or probable dementia).
Facilitators and Barriers of Social Participation: Linear Regression Results
Correlates of Social Participation: Linear Regression Results
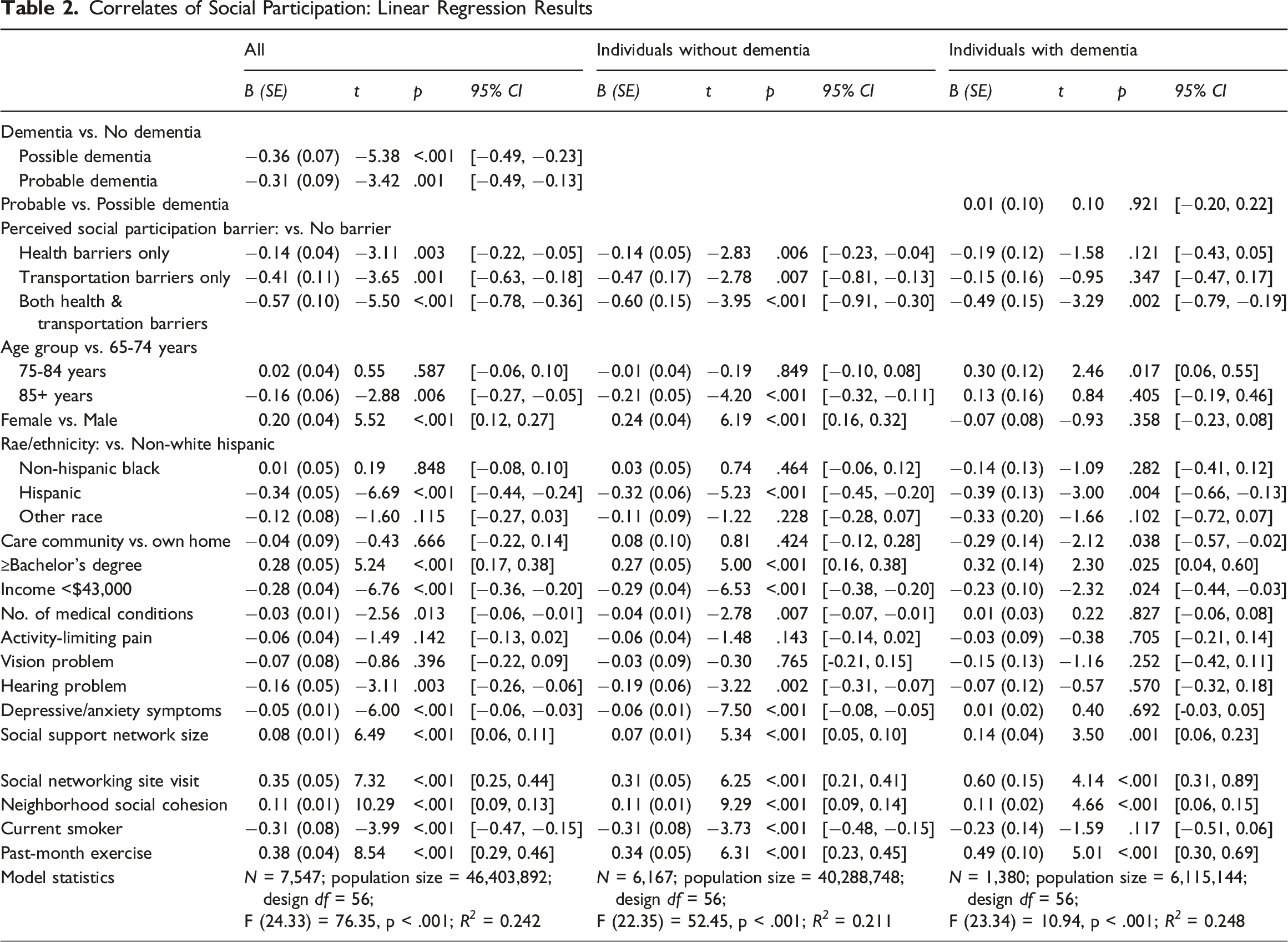
The results for individuals with dementia in the last four columns of Table 2 show no significant difference by dementia type, and most facilitators and barriers were similar to those for individuals without dementia, although there were some differences. The 75-84 age group, compared to the 65-74 age group, was associated with more social participation, while care community residence was associated with fewer social participation. Gender, number of medical conditions, hearing impairment, depressive/anxiety symptoms, and smoking were not significantly associated with social participation.
Associations Between Psychological Well-Being and Social Participation: Linear Regression Results
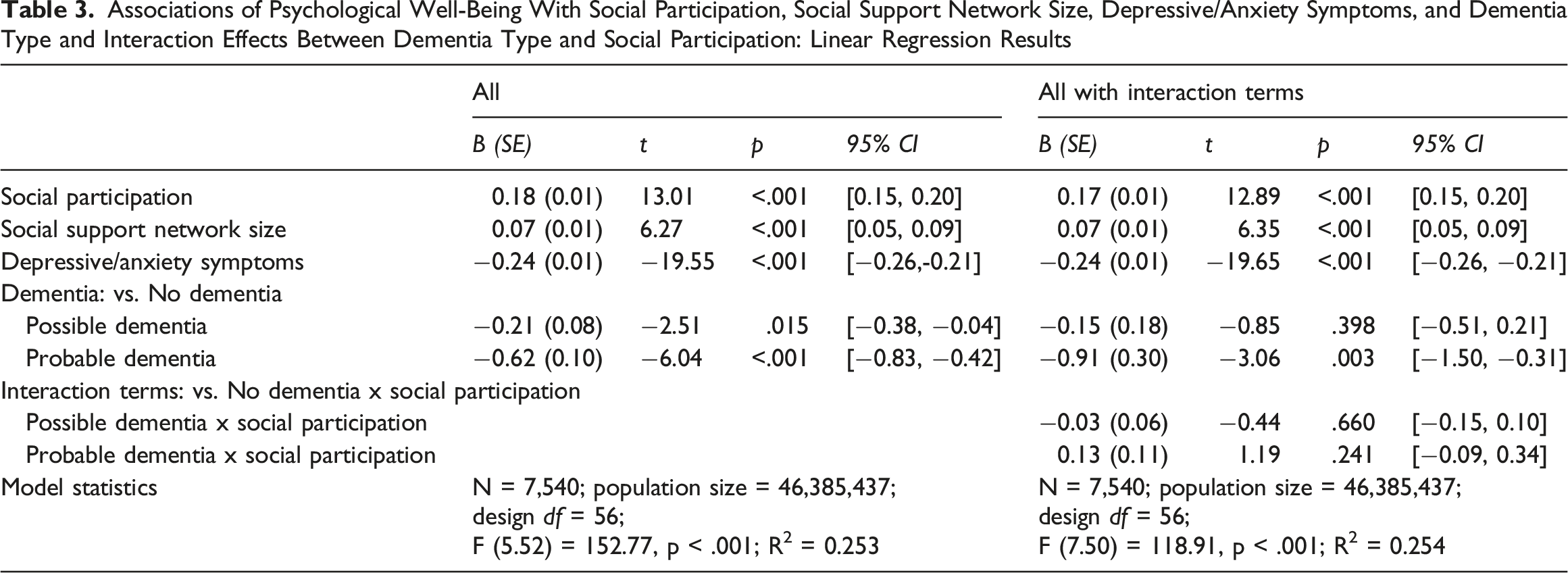
Associations of Psychological Well-Being With Social Participation, Social Support Network Size, Depressive/Anxiety Symptoms, and Dementia Type and Interaction Effects Between Dementia Type and Social Participation: Linear Regression Results
Mediation Effects: Path Model Results for Individuals with Dementia
Effects of Social Support Network Size and Depressive/Anxiety Symptoms on the Association Between Probable versus Possible Dementia and Social Participation Among Those With Dementia: Model Parameters From the Mediation Model Using Path Analyses
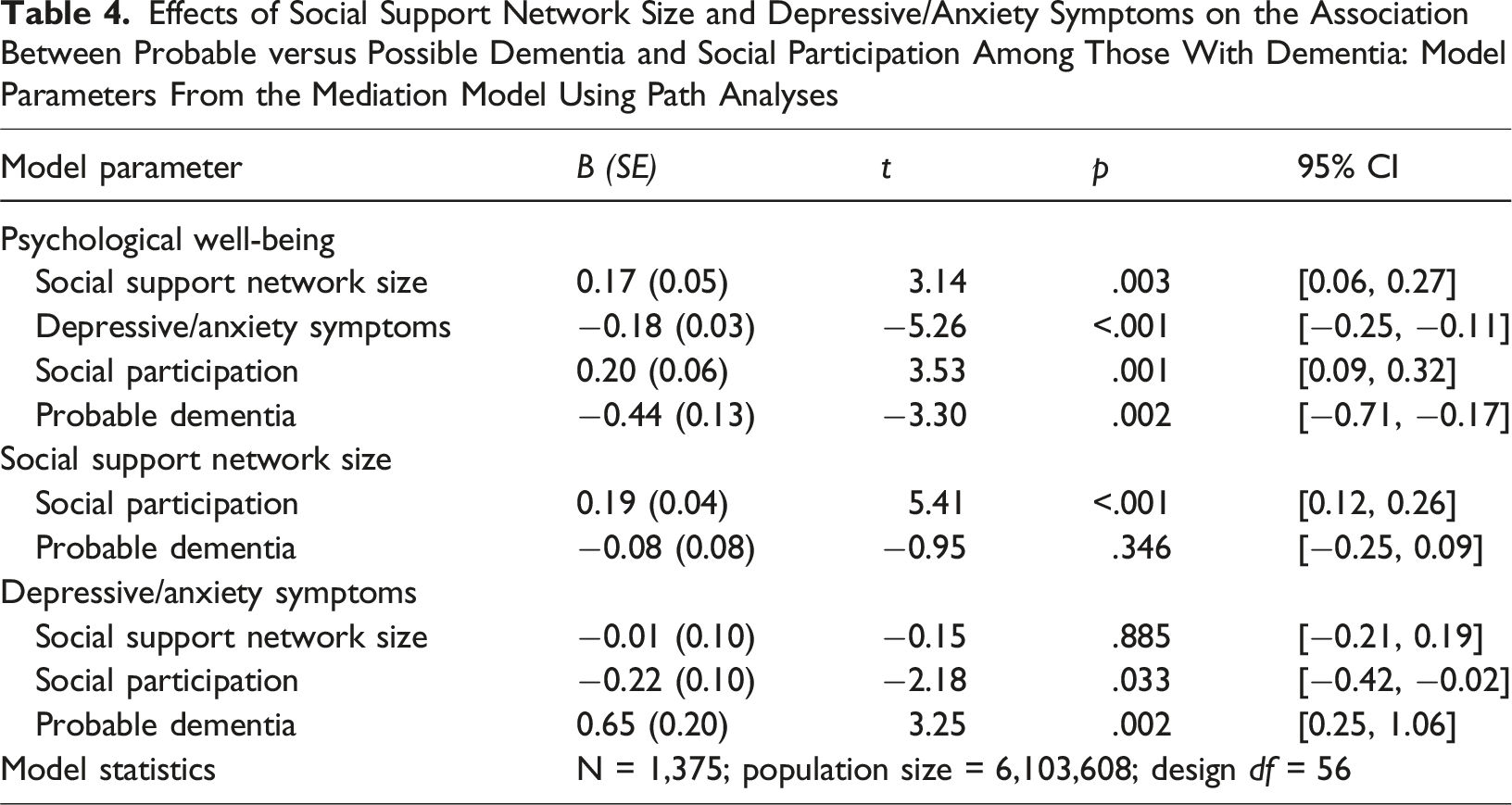
Indirect effects of SSNS and depressive/anxiety symptoms on psychological well-being: Bootstrapped results show a significant indirect effect of social participation on psychological well-being through SSNS (B [SE] = 0.03 [0.01], z = 2.64, p = .008, 95% CI = 0.01 0.06 ) and depressive/anxiety symptoms (B [SE] = 0.04 [0.02], z = 2.34, p = .019, 95% CI = 0.01, 0.07). The proportion of the indirect effect of SSNS on social participation (0.03) relative to the total effect of social participation on psychological well-being (indirect effect [0.03] + direct effect [0.20] = 0.23) was 0.13. The ratio of the indirect effect of SSNS on social participation to the direct effect of social participation on psychological well-being was 0.15. The proportion of the indirect effect of depressive/anxiety symptoms on social participation (0.04) relative to the total effect of social participation on psychological well-being (indirect effect [0.04] + direct effect [0.20] = 0.24) was 0.17. The ratio of the indirect effect of depressive/anxiety symptoms on social participation to the direct effect of social participation on psychological well-being was 0.20.
Discussion
Social participation in later life is widely recognized for its substantial benefits to physical, mental, and cognitive health. However, prior research has found that older adults living with dementia experience a decline in social participation. In this study, using data from the 2023 NHATS, we examined the facilitators and impediments to social participation among older adults with dementia, compared to those without dementia, and the moderating effects of dementia type on the relationship between social participation and psychological well-being. We also investigated the mediating effects of SSNS and depressive/anxiety symptoms on the association between social participation and psychological well-being among older adults with dementia.
More than one in eight NHATS self-respondents in our study met criteria for possible or probable dementia, and these older adults were significantly less likely to participate in various social activities, including visiting family or friends, attending meetings, working or volunteering, and going out for enjoyment, than those without dementia. These findings underscore the significant impact of cognitive impairment on older adults’ ability to maintain social ties and participate in meaningful community roles.
Regardless of dementia status, social participation was positively associated with having a college degree, a larger social network, visiting social networking sites, neighborhood social cohesion, and engaging in exercise, including walking. Conversely, health- and transportation-related barriers, low income, and Hispanic ethnicity were significantly negatively associated with social participation.
These findings align with previous research indicating that higher socioeconomic status (SES), digital connectivity, and neighborhood-level social capital are protective factors for social engagement in later life, while lower SES is a risk factor. For instance, Steptoe and Zaninotto (2020) found that lower SES was associated with broad declines in physical, sensory, cognitive, emotional, and social functioning over time. The significant role of perceived neighborhood social cohesion in social participation is also notable. Prior research has shown that positive perceptions of neighborhood social cohesion buffer against social isolation and loneliness, particularly among lower SES older adults (Choi, 2024; Cornwell & Goldman, 2021). The positive association between exercise and social participation in this study may also suggest that older adults are more likely to venture outside and engage socially when they feel safe in their neighborhood environment. The positive association between visiting social networking sites and social participation suggests that digital connectivity may help maintain or even enhance social engagement in later life. This may be especially important for individuals with physical or cognitive limitations that constrain in-person interactions. Social networking platforms can serve as accessible venues for maintaining interpersonal relationships, accessing community information, and fostering a sense of connection, even in the face of mobility restrictions, cognitive impairments, or reduced local ties. A recent study found that people with dementia utilized social media to maintain continuity between their pre- and post-diagnostic selves, providing a sense of stability amid uncertainty and fostering community connections (Talbot et al., 2025).
Transportation challenges, in particular, remain a persistent systemic obstacle among non-driving, disabled older adults and call for comprehensive public policy solutions (Dabelko-Schoeny et al., 2021). Hispanic ethnicity was also significantly associated with lower social participation, even after adjusting for other factors. While limited research has focused specifically on Hispanic older adults with dementia, previous studies suggest that family-oriented engagement may be more common in this group, and that language barriers and lower education levels may restrict broader social involvement (Rodríguez-Galán & Falcón, 2010). These findings highlight the importance of considering cultural and linguistic contexts when designing interventions to promote social engagement.
Among those without dementia, chronic medical conditions, hearing impairments, depressive/anxiety symptoms, and smoking were negatively associated with social participation; however, these associations were not observed in individuals with dementia when accounting for other factors. This may suggest that dementia itself poses such a dominant constraint on social participation that other factors exert relatively weaker effects. The fact that the residence in a care community was a significant barrier to social participation only among those with dementia likely reflects a higher burden of physical and cognitive impairment in this group, coupled with environmental constraints that limit opportunities for meaningful engagement. Targeted interventions in residential care settings are needed to promote social connection and psychological well-being in residents with cognitive impairment.
While vision and hearing impairments were not independently associated with reduced social participation among those with dementia in the adjusted models, a substantially higher proportion of this group experienced sensory impairments compared to their cognitively unimpaired counterparts. This is consistent with prior research demonstrating that sensory impairments not only co-occur with dementia but may exacerbate its progression and functional consequences (Chen et al., 2021; Kuo et al., 2021; Livingston et al., 2024). Furthermore, vision loss can restrict mobility, limit technology use, and increase dependency, all of which undermine social engagement (Jaiswal et al., 2020; Patel et al., 2020). These findings underscore the importance of early detection and treatment of sensory impairments as a strategy to preserve social participation and autonomy among older adults with dementia.
As expected, social participation and SSNS were positively associated with psychological well-being, while depressive/anxiety symptoms were negatively associated. Interaction terms between social participation and dementia status were not statistically significant, indicating that the relationship between social participation and psychological well-being did not differ by cognitive status. This finding underscores the universal importance of social participation for supporting psychological well-being among older adults, regardless of whether they have dementia. Nonetheless, probable dementia was independently associated with lower psychological well-being, highlighting the psychological vulnerability of individuals with more advanced cognitive impairment.
Among older adults with dementia, path analysis further confirmed that the association between social participation and psychological well-being was partially mediated through its influence on SSNS and depressive/anxiety symptoms. Specifically, greater social participation was linked to larger SSNS and lower levels of depressive/anxiety symptoms, both of which were associated with higher psychological well-being. These findings suggest the multifaceted pathways through which social participation can promote mental and emotional health, even in the context of cognitive decline. Although the cross-sectional nature of the data limits causal inference, the relationship between social participation and SSNS is likely reciprocal. Larger social networks provide more opportunities for engagement, while greater social participation fosters social connectedness and relationship building (Townsend et al., 2021). Prior studies have similarly found that participation in community-based activities and technology use enhances perceived social connectedness and associated well-being outcomes (Suragarn et al., 2021). For instance, Ashida et al. (2018) found that older adults with more network members who provided companionship or co-participated in activities reported higher environmental mastery, more positive interpersonal relationships, and greater satisfaction with their social networks.
Although the direct association between social participation and depressive/anxiety symptoms was not statistically significant among older adults with dementia in the linear regression model that adjusted for a wide range of sociodemographic and health-related covariates, our path analysis did find a significant association. This difference may reflect variation in model specification rather than a true contradiction. In the linear model, the inclusion of many covariates may have attenuated the relationship between social participation and depressive/anxiety symptoms, whereas the path model, which emphasized the theoretical relationships among social participation, SSNS, depressive/anxiety symptoms, and psychological well-being, captured this association more clearly. These findings suggest that social participation still plays an important role in psychological well-being among older adults with dementia, particularly through its influence on social connectedness and depressive/anxiety symptoms. This interpretation aligns with prior research showing that socially active older adults, especially those engaged in diverse and meaningful activities, tend to report lower levels of depression/anxiety (Chiao et al., 2011; Choi et al., 2021; Shiba et al., 2021). Given the high prevalence of emotional distress in dementia (Leung et al., 2021), promoting social participation remains a promising nonpharmacological strategy to support psychological well-being in this population.
Our study had some limitations due to the short measures of key constructs in the NHATS. Social participation was not captured in terms of activity frequency, and depressive/anxiety symptoms and psychological well-being were assessed with only four items each. The Cronbach’s alpha for the psychological well-being measure was less than optimal. Also, the SSNS was limited to the number of strong relationships and did not include peripheral support from weak ties, which may provide informational and instrumental support. The other limitations are that only correlation, not causation, can be derived from cross-sectional survey data, and that self-reports of social participation, depression/anxiety, and psychological well-being may have been subjected to recall, especially among those with dementia, and social desirability bias.
Despite these limitations, this study provides valuable insights into social participation among older adults with dementia and offer several implications for enhancing their social engagement. First, health and transportation barriers to social participation, which are common among both individuals with and without dementia, must be addressed through expanded transportation programs tailored to the needs of older and disabled adults. Dementia-friendly transportation services must include increased accessibility and availability as well as training on using mass public transit and mobility management (Lanthier-Labonté et al., 2024). Escort and buddy services, which assist older adults in attending events and activities, are also an option (Silverstein & Turk, 2016). Second, given the positive associations between social participation, exercise engagement, and use of social networking sites, efforts should be extended to involve older adults with dementia in group exercise and technology training, ideally offered in accessible community venues such as neighborhood-based recreational or senior centers. Virtual social programs have also shown promise in increasing social interactions among older adults with dementia (Dai & Moffatt, 2023; Sun et al., 2024). Third, social activities should be intentionally designed to foster connectedness, reduce depressive/anxiety symptoms, and potentially slow cognitive decline among older adults living with dementia. To name a few, memory cafés (Protoolis et al., 2022), group-based cognitive stimulation therapy (Orfanos et al., 2021), reading groups (DeVries et al., 2019), choir-singing (McDowell et al., 2023; Ridder et al., 2025), and reminiscence groups (Syed Elias et al., 2015) have been shown to increase social connectedness and psychological well-being. Fourth, considering the lower likelihood of social participation among Hispanic older adults and those with lower income or education, targeted efforts are needed to provide culturally responsive and accessible support. Adopting a public health approach to dementia care will be critical to reducing disparities and promoting equitable opportunities for social participation.
In conclusion, this study highlights both common and dementia-specific correlates of social participation in later life. While structural and socioeconomic factors play a central role across all older adults, cognitive impairment amplifies barriers and alters the relevance of certain health-related predictors. Our findings also showed that, among individuals with dementia, social participation was positively associated with psychological well-being, both directly and indirectly through its associations with larger social support networks and lower depressive/anxiety symptoms. Promoting continued social participation in this population will require comprehensive, multifactorial strategies that address not only individual and environmental constraints but also the cognitive, sensory, and digital inclusion challenges that uniquely affect these older adults.
Footnotes
Ethical Considerations
The University of Texas at Austin’s Institutional Review Board exempted this study based on de-identified public-domain data.
Author Contributions
Study concept and design: NGC, CNM, YZ, MEK. Acquisition of data: NGC. Data analysis: NGC. Interpretation: NGC, CNM. Drafting of the paper: NGC. All authors reviewed and revised it critically for important intellectual content and gave final approval of the version to be submitted.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by grant P30AG066614, awarded to the Center on Aging and Population Sciences at The University of Texas at Austin by the National Institute on Aging.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this study (The National Aging and Health Trends Study) are in the public domain.