
Abstract
The prevalence of dementia among Black families of African descent in Canada is projected to rise by 507%, according to The Many Faces of Dementia in Canada report. Despite this forecast, there remains a significant empirical gap regarding the lived realities of Black individuals with dementia and their care partners. This study addresses that gap by exploring the everyday realities of dementia care within Black communities in the Greater Toronto and Hamilton Area, particularly during the COVID-19 pandemic. Utilizing a qualitative interpretive lens, the study purposively sampled 24 participants (12 older adults with moderate dementia and their 12 care partners) for in-depth, dyadic interviews. Data were analyzed thematically using a reflexive lens. Findings indicate that care partners, whether care partners or healthcare professionals, take on extensive responsibilities in decision-making, daily care provision, and emotional support, which are shaped by pre-existing systemic inequities, including exposure to racial discrimination, and inadequate access to culturally responsive services. The pandemic further intensified these stressors, yet participants demonstrated resilience by drawing on communal resources and informal networks. The findings revealed that care-partners of people with dementia operate within a system that both relies on and marginalizes their labour. Yet, care-partners resisted these exclusions through collective resilience and community-based strategies. This study advocates for improving equitable access to services, reducing systemic barriers that delay recognision, and acknowledging the essential contributions of Black care-partners in Canadian caregiving framework.
Introduction
Alzheimer’s disease and other related dementias is a pressing global health concern, disproportionately impacting older adults and placing significant care duties on the responsibility of their care-partners who take on the emotional, physical, and financial aspects of care (Farina et al., 2024). In Canada, roughly 700,000 individuals currently live with dementia, a figure projected to continue rising alongside the country’s shifting demographics (Alzheimer Society of Canada, 2024). However, this burden is not evenly distributed across populations. The Alzheimer Society of Canada’s report The Many Faces of Dementia in Canada projects a staggering 507% increase in the prevalence of dementia among Black Canadians by 2030a statistic that signals an impending crisis (Alzheimer Society of Canada, 2024). This alarming projection has not been met with commensurate research or policy attention. While studies from the United States and the United Kingdom offer some insights into dementia experiences in Black communities, their applicability to the Canadian context is limited due to lack of race based health data collection and gaps in studies on the experiences of dementia in the Black community in Canada (Alexander et al., 2022; Berwald et al., 2016; Bonds Johnson et al., 2022; Hussain et al., 2009; Lawrence et al., 2008). This gap left a knowledge gap in the way Black Canadians experience the dementia trajectory, as people living with the disease and care partners, including navigating the healthcare system. Consequently, the experiences of care giving for dementia in the Black context remains largely neglected in empirical research, leaving care-partners of Black older adults who already face systemic inequities with inadequate institutional support (Alzheimer Society of Canada, 2024; Tong et al., 2022).
Within many Black communities, caregiving roles are deeply rooted in familial and communal responsibility; however, stigma surrounding dementia can amplify care partners emotional distress, creating a dual burden of duty and isolation (Alexander et al., 2022; Bonds Johnson et al., 2022; Oliver et al., 2022). Moreover, these challenges are compounded by a healthcare system that remains fragmented, exclusionary, and largely unresponsive to the diverse caregiving needs of Black families.
The COVID-19 pandemic starkly exposed and amplified these, and other systemic disparities. Racialized care-partners, particularly Black women, were disproportionately represented among both formal and informal care partners, bearing the brunt of pandemic-related hardships (Boatswain-Kyte et al., 2025; Mahabir et al., 2021; Phillips-Beck et al., 2020). Lockdowns and disruptions to health and social services exacerbated social isolation, emotional stress, and financial strain, while creating new barriers to essential dementia care (Chyu et al., 2022; Dourado et al., 2020; Elugbadebo et al., 2022). These impacts further marginalized Black care-partners who were already struggling to access culturally competent support for their loved ones. The healthcare system’s failure to accommodate such intersectional challenges reflects broader systemic inequities, leaving Black families underserved, and forcing care-partners to act as liaisons between their loved ones and the medical system.
Despite growing advocacy efforts and media reports highlighting racial disparities in dementia care, empirical research on how race, culture, and immigration status shape the caregiving experiences of Black families in Canada remains scant (Iroanyah et al., 2021). This persistent knowledge gap perpetuates a one-dimensional, Eurocentric understanding of aging and caregiving by overlooking the unique experiences and needs of Black older adults and their care-partners. Without targeted research and policy interventions, these inequities will continue, reinforcing cycles of exclusion in Canada’s healthcare and social support systems.
In response to these challenges, the present study addresses this critical gap by exploring the lived experiences of care-partners of Black older adults with dementia in Canada during the COVID-19 pandemic. This study offers timely insights and represents an important step toward developing equitable healthcare policies and community-based, culturally responsive dementia care services that reflect Canada’s multicultural landscape.
Methods
A qualitative interpretivist lens was used in this study to explore the lived experiences of Black care-partners supporting individuals with dementia. This constructivist approach encourages researchers to attend to and use their own expertise to develop rich and meaningful interpretations of the data to guide practice (Thorne, 2016). This approach provided avenues for applying our collective lens to the experiences of black care-partners of people with dementia to the research process. . Interpretive qualitative research seeks to provide a rich, comprehensive account of the meaning-made from participants’ experiences, shaped by their everyday realities, social contexts, and cultural identities.
Data collection and analysis were designed to capture the multiple truths and interpretations of care-partners as they navigated caregiving during the COVID-19 pandemic. This approach prioritizes participants’ own language and categories of meaning, allowing for a nuanced and authentic representation of their experiences. This study focused on what participants expressed and how they described their roles, emotions, and strategies. The analysis provided insight into the specific challenges they faced such as systemic racism, cultural insensitivity in healthcare visits, and limited access to resources, the culturally grounded practices they employed to sustain care. Centering care-partners’ voices within their socio-cultural contexts, the interpretive qualitative design illuminated how race, culture, and caregiving intersect, offering critical implications for more equitable, culturally responsive health and social care policies.
Sampling and Recruitment Strategy
Recruitment was conducted by the research assistant (RA) with assistance from the research team and members of the Advisory Committee through purposive sampling. Purposive sampling was used to ensure that the sample was representative of diverse Black people living with dementia, including diversity based on two or more of the following: culture, citizenship status (immigrant or Canadian-born), gender identity, sexual orientation, age, disability, income, and socio-economic status. The following strategies were used to recruit participants: (1) the RA reached out to organizations in the GTHA to discuss the study with their clients during their programs; (2) The Alzheimer Society of Canada provided access to participants through their research portal, where researchers may post participant recruitment ads; (3) recruitment material (posters, for example) was sent to organizations in the GTHA (including members of the advisory committee for this study) for them to share the recruitment material via email, their website, and social media; and (4) the research team shared the recruitment material with their own networks via email and social media. Due to the sensitivity of the topic and the high visibility of our research PI’s (each have conducted numerous presentations and talks in the Black community) each potential and actual participant was assured that their participation was completely voluntary without any impact on their healthcare or social care access. A total of 24 participants were recruited using a dyadic approach: 12 Black Canadian individuals living at home in the Greater Toronto and Hamilton Area with moderate or middle-stage dementia and their 12 care partners.
Data Collection
Data collection involved dyadic interviews with twenty-four (24) participant pairs, consisting of individuals living with dementia and their care partners. Non-Standard interview guides, developed in collaboration with our research team and community discussion meetings with care partners and people living with dementia, were used to conduct the interviews. The second author and third authors interviewed the person with dementia using the non-standardized interview guide, which allowed for an open-ended, conversational approach that captured participants lived experiences in depth. Given the constraints of the COVID-19 pandemic, all interviews were conducted via Zoom and were digitally recorded for accuracy. The interviews were transcribed verbatim and analyzed using NVivo qualitative software, which facilitated a structured yet interpretive exploration of the narratives. Interviews with individuals living with dementia focused on their perceptions, beliefs, and attitudes toward dementia, their lived experiences with the condition, and the ways in which COVID-19 shaped these experiences. Participants discussed the supports, services, and activities they engaged with to maintain their health and well-being, particularly in relation to physical activity, nutrition, sleep, and social interactions all within the evolving context of the pandemic.
A separate, non-standardized interview guide was used for care partners, centering on their experiences providing care to individuals living with dementia. These discussions explored the emotional, cognitive, social, and physical dimensions of caregiving, as well as care partners’ interactions with health and social support systems. Particular attention was given to the barriers and challenges they encountered in accessing services for both themselves and the individuals they supported, especially in light of the disruptions caused by COVID-19. The interpretive narrative approach provided a nuanced understanding of how care partners navigated these complexities, offering insight into the structural and relational dimensions of caregiving during a period of heightened vulnerability and systemic strain.
Data Analysis
All interviews were audio-recorded, transcribed verbatim, and analyzed using reflexive thematic analysis (Braun & Clarke, 2019) within an interpretivist paradigm. NVivo 12 was used to organize data. We followed a careful, iterative process to move from raw transcripts to final themes. We began by immersing ourselves in the interview data. Each researcher (O.O. and B.M.) read transcripts several times to become familiar with participants’ tone, emotions, and emphasis. During this stage, we made initial notes about striking phrases such as “I had to get him vaccinated” and “I’m like his personal assistant” which signaled duty, advocacy, and identity work.
Next, we completed line-by-line coding, labelling segments of text that reflected key ideas or actions. Early codes included: protecting loved ones through vaccination, convincing elders to trust care, stepping into medical roles, being physically present at all times, and providing emotional reassurance. We kept long excerpts to preserve context and meaning. After individual coding, we met to compare interpretations, clarify meanings, and refine code boundaries. Once an initial code list was developed, we grouped similar codes together into broader analytic categories, such as ethical duty and protection, care as clinical extension, and emotional steadfastness. We revisited transcripts repeatedly, testing whether these categories fit the data and adjusting where needed. From these categories, we developed final themes that captured the deeper story of the data. Themes such as Vaccination as Relational Labour, Health Mediation as Everyday Resistance, Full-Time Embodied Caregiving, and Emotional Support as Core Care Work emerged. We selected quotes that best illustrated participants’ experiences and the cultural and structural forces shaping them. Throughout the process, we engaged in ongoing reflexive conversations—questioning how our experiences as Black scholars and practitioners might influence interpretation and remaining attentive to participants’ intended meanings (Naeem et al., 2023). Pseudonyms protect participant identities.
Reflectivity
As researchers engaged in examining the experiences of Black dementia caregivers during the COVID-19 pandemic, we recognize that our social locations, identities, and professional backgrounds shape the questions we ask, the relationships we build, and the ways we interpret data. Members of the research team identify as racialized scholars with lived and/or professional experience working with immigrant, African and Caribbean communities, aging populations, and dementia care systems in Canada. Our proximity to these communities provided cultural insight and relational sensitivity that strengthened participant trust, enhanced culturally nuanced interpretation, and informed our understanding of caregiving values grounded in reciprocity, collective responsibility, and intergenerational care (Braun & Clarke, 2019).
At the same time, shared cultural and racial identities while fostering rapport carried risks of assumptions, over-identification, and interpretive bias. We remained aware that our own experiences with racism, caregiving, and healthcare institutions could influence how we understood and prioritized participants’ narratives. To address these risks, we engaged in continuous reflexive practice throughout the research process by maintaining analytic memos, engaging in team-based coding discussions, and intentionally questioning taken-for-granted cultural meanings. We also critically reflected on how our academic training and location within Canadian research institutions may inadvertently reproduce dominant frameworks, even as we critique them. Additionally, our professional stance as social worker, health and aging-care researchers positioned us as advocates for equity in dementia care. This advocacy lens may have predisposed us to highlight systemic failures and resilience narratives. To mitigate this, we prioritized grounding interpretations in participants’ voices and contextual realities, acknowledging variation in experiences across migration histories, socioeconomic status, and care arrangements. We recognize that knowledge production is relational, and we view this study as co-constructed with participants who entrusted us with their experiences. Our reflexive stance aims to honor these voices, foreground structural analysis, and contribute to scholarship that challenges deficit perspectives and advances justice-centered dementia care.
Ethical Considerations
This study received approval from McMaster University: MREB#: 6403. Where institutional ethics approval was not required, verbal consent was obtained from eldest family member. In some ethnic communities in greater Toronto area and Hamilton, close family friends or neighbors are considered part of the caregiving team and may provide emotional or practical support.
Demographic Information of the Study Participants
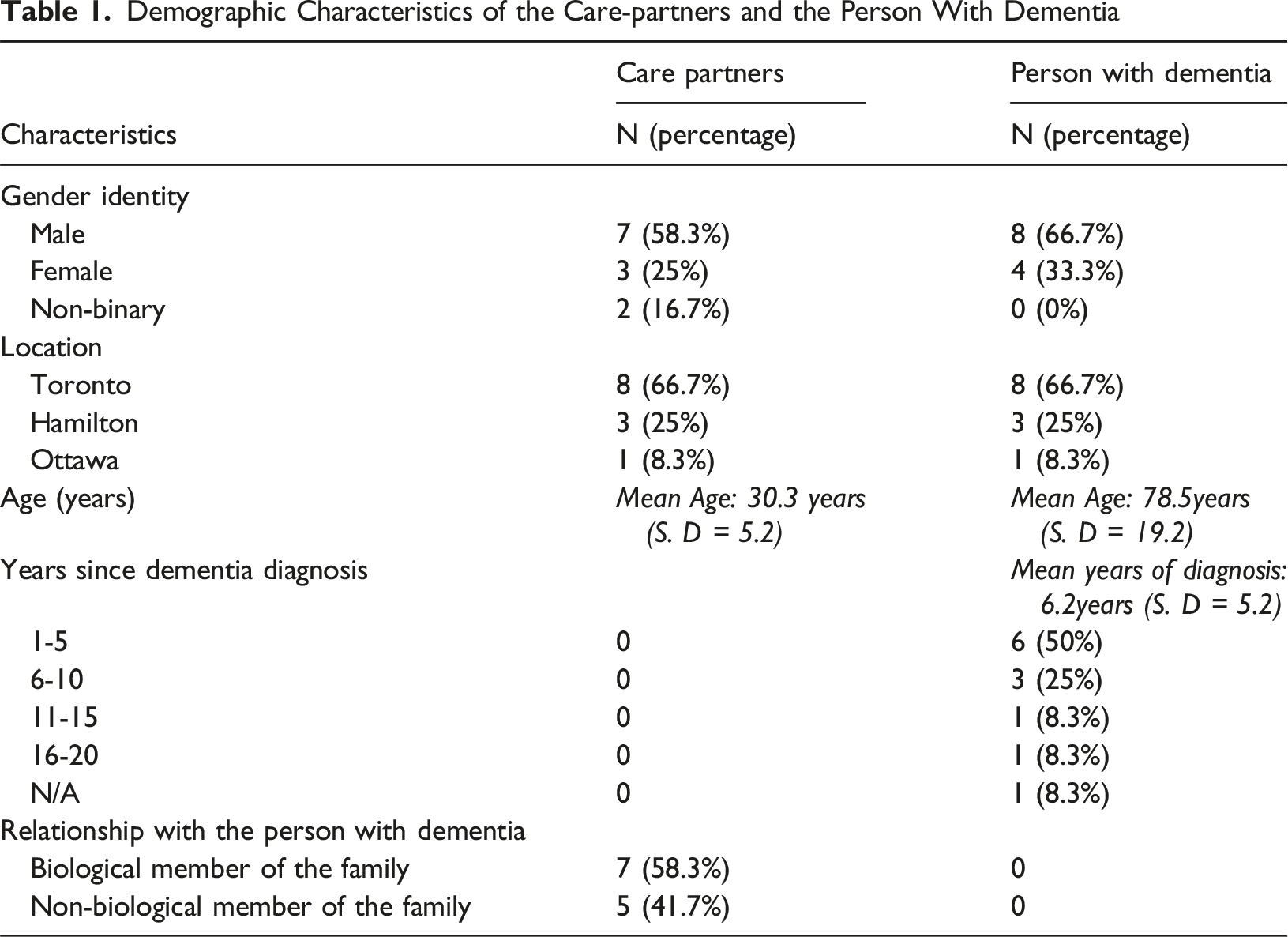
The demographic analysis of the participants includes person with dementia (66.7%) and their care partners (58.3%) are male. Geographically, most participants (66.7%) were recruited from Toronto, followed by 25% from Hamilton and 8.3% from Ottawa. The mean age of care partners was 30.3 years, while the mean age of individuals with dementia was 8.8 years. On average, participants had been living with dementia for 62.2 years, with nearly half receiving their diagnosis within the past 1 to 5 years. In terms of caregiving relationships, 58.3% of care partners were biological relatives, whereas 41.7% were non-relatives.
Overview of Findings
Demographic Characteristics of the Care-partners and the Person With Dementia
Vaccination as Moral Responsibility and Relational Negotiation
Vaccination as Protection Against Systemic Risk
For some care partners, vaccination was understood as an ethical imperative and as a way of shielding vulnerable loved ones from a healthcare system historically inattentive to Black health outcomes. Care partners (Care partners (2) reflects: “Yeah, I had to get him vaccinated. Yeah, we had to get vaccinations. And always kept cautious that everyone who came close to us would have, you know, protected themselves.” (Care partners 2)
The phrase “had to” emphasizes an unspoken but deeply felt obligation. The decision-making process is situated within a broader context of heightened exposure to COVID-19, compounded by histories of underdiagnosis and lack of culturally appropriate care for dementia.
Vaccination as Relational Labour
For some care partners, caregiving extended into the domain of health negotiation and relational persuasion, particularly in contexts marked by justified medical skepticism. As Care partners 6 reflects: Care partners 6 explains: “With the help of the staff, they really educated me on it. And I had to convince him that we get the shots for the vaccine. And he didn't hesitate much. So that's what I had to do.” (Care partners 6)
The care partner occupies a dual position first as a recipient of institutional knowledge, then as a cultural and relational mediator responsible for translating that knowledge into action within the family. The repeated use of “had to” conveys both moral obligation. The phrase “convince him” signals the emotional and interpersonal labor involved.
Health Mediation as Everyday Resistance
Acting as De Facto Medical Professionals
In a healthcare system where Black patients often face underassessment and miscommunication, care partner can fill critical knowledge and care gaps. Care Recipient10 describes: “I think he was literally the one playing the role of a doctor… he did any kind of little assessment… Or anything that involved any casual assessments, he was able to carry it out and give feedback.” (person with dementia 10)
Even seemingly small tasks, like booking appointments, required persistence and resilience. Care partners 9 shares: “Maybe setting up dates for appointments for doctors.” (Care partners 9)
Although understated, this quote reflects the invisible labor of ensuring continuity of care, and managing stress around possible delays and cancellations in the healthcare systems. The logistical tasks are compounded by digital divides, bureaucratic inefficiencies, linguistic or cultural disconnects, and outright racism in healthcare.
Full-Time Embodied Caregiving
Caregiving as 24/7 Physical and Emotional Presence
The pandemic intensified the already demanding nature of dementia care. Care partners 10 describes their role: “I’m like his personal assistant… My role is to personally care for [him]. Anything he wants, his food, his clothing, everything. It’s more like I should just be physically available when he needs me.” (Care partners 10)
Describing oneself as a “personal assistant” evokes a professionalized but emotionally sanitized image. Yet, the elaboration reveals the immersive and constant nature of care, rooted in proximity and attunement.
Medication Management as an Invisible Discipline
Medication adherence, particularly for older adults with cognitive decline, can be a high-stakes task involving attunment to personal feelings and rationale around compliance to takin medication. Care partners 2 reflects: “I would say most of the time I would make sure that he is taking up his meds.” (Care partners 2)
The phrase “most of the time” implies a constant vigilance, and overseering role that includes a quiet discipline embedded into ensuring a daily routine is followed. . For Black families, improper medication adherence can be attributed to many factors, including communication breakdowns with health professionals on how to take medications properly and lack of culturally adapted instructions.. Thus, care partners take on a gatekeeping role, ensuring safety and continuity in a fragmented and racialized health system.
Emotional Support as Core Care Work
Caregiving as Emotional Anchoring
Dementia is an emotional and social condition that reshapes relationships and renders care partners emotional stabilizers. Care partners 2 shares: “If I’m realizing that he has problems, I tried to be there for emotional support… Sometimes he may have some breakdowns. And it’s very important that you be there because breakdowns can be very, very bad.” (Care partner 2)
This statement captures the emotional labor of caregiving. The repeated emphasis on “you have to be there” aligns with the necessity of constant attentiveness, culturally grounded ethic of care, where being emotionally available is tied to familial duty and moral responsibility.
Cognitive Engagement as Resistance to Decline
One of the care-partner shared that intimate strategy for keeping their Care Recipient mentally active: “On my own way, I just tried to engage her with some games at home, chat, movies, and the rest.” (Care partners 1)
The phrase “on my own way” speaks to the creativity and resourcefulness care partners employ in the absence of formal cognitive stimulation programs. These everyday acts, including games, chatting, and sharing.
Discussion of Findings
This study being the first empirical report exploring the lived experiences of Black families support people with dementia during in Canada during the COVID-19 pandemic. Findings demonstrated that caregiving in this context is an embodied, racialized practice shaped by historical mistrust, systemic inequities, and cultural norms of familial responsibility. Across the themes of vaccination, health mediation, embodied caregiving, and emotional support, participants described relational labor extending beyond routine care to encompass advocacy, negotiation, and resistance against systemic neglect.
Our findings showed securing vaccination for the person with dementia was regarded as a moral imperative. As one care partner explained, “Yeah, I had to get him vaccinated,” vaccination was framed as non-negotiable amid heightened vulnerability. This aligns with the disproportionate COVID-19 burden in Black communities in Canada, linked to structural determinants such as crowded housing, frontline work, and inequitable healthcare access (Dryden & Nnorom, 2021; Kemei et al., 2023; Olanlesi-Aliu et al., 2024). In a context where culturally responsive dementia care is limited, vaccination became an act of self-protection and familial survival (Idorenyin Imoh & Charity, 2023; Yang et al., 2021).
For others, vaccination required persuasive emotional labor due to intergenerational mistrust of healthcare institutions, a mistrust rooted in historical abuses and ongoing discrimination (Bazargan et al., 2021; Dryden & Nnorom, 2021). Care partners acted as cultural mediators, leveraging trust-based relationships and selectively integrating healthcare advice. This supports evidence that Black care partners frequently serve as “health translators” between misaligned services and family needs (Fabius et al., 2020; Heath et al., 2023; Scharff et al., 2010).
Participants also described assuming quasi-professional roles, “playing the role of a doctor” by conducting assessments, monitoring symptoms, and advocating for medical attention, tasks intensified by the pandemic. Such informal medical labor, often borne by Black women, reflects systemic gaps in dementia diagnosis and culturally safe care and represents both care ingenuity and everyday resistance (Findley et al., 2023; Lwi et al., 2023). Even logistical tasks, such as scheduling appointments, were complicated by limited digital access, long waits, and poor provider communication, requiring care partners to navigate fragmented systems to ensure continuity of care (Feng et al., 2024; Oliver et al., 2022).
Caregiving was described as immersive and constant, often without respite or formal supports. Statements such as “I’m like his personal assistant… physically available when he needs me” reflect both the task-oriented and emotional dimensions of care. Consistent with prior research, participants framed caregiving as a moral and familial duty (Dilworth-Anderson et al., 2020), often providing more hours of care than White counterparts but with fewer resources (Fabius et al., 2020; Yoshikawa et al., 2023).
Emotional support emerged as a critical dimension, with care partners mitigating distress, monitoring mood changes, and maintaining relational stability. For families facing systemic racism, economic strain, and immigration precarity, this emotional labor functioned as a survival strategy (Alzheimer Society of Canada, 2024; Olanlesi-Aliu et al., 2024). In the absence of formal cognitive supports, participants relied on culturally grounded engagement strategies such as storytelling, music, shared activities, reflecting adaptive, “home-grown” interventions shown to benefit people with dementia when aligned with cultural and relational contexts (Fels & Astell, 2011).
Overall, our findings highlight the intersection of racialized structural inequities and culturally grounded ethics of care in shaping the experiences of Black families supporting people with dementia the COVID-19 pandemic. Black care partners’ capacity to integrate advocacy, health system navigation, and culturally responsive engagement signals both the resilience and the systemic burden disproportionately placed on visible minority families. Addressing these inequities requires structural reform to ensure equitable, culturally safe dementia care in Canada.
Conclusions
Black care partners of people with dementia in Canada provide care far beyond the bounds of familial support, enacting a layered praxis of care and resistance forged within systemic inequities and cultural obligations. What is often described as “duty” operates both as kinship responsibility and adaptive response to institutional neglect, racialized health disparities, and fragmented systems of care. Their work integrates medical mediation, advocacy, and emotional anchoring forms of labor that sustain loved ones while simultaneously exposing structural gaps. This resilience, however, must not obscure the inequities that necessitate it. Current Canadian caregiving framework has effectively transfer the costs of institutional failure onto Black families, normalizing unpaid, invisible labor. Dementia care could therefore be reimagined through frameworks of equity, cultural safety, early recognition of symptoms and collective accountability, advancing policies and practices that redistribute responsibility, adequately resource care, and honor the cultural ethics that have long sustained Black caregiving communities in Canada.
Limitations
This study had several limitations, and we took deliberate steps to mitigate their effects. First, the sample focused on Black older adults with dementia and their care partners in the Greater Toronto and Hamilton Area, which may not capture regional variations in Black caregiving experiences across Canada. To enhance transferability, we purposively recruited participants with diverse migration histories, caregiving arrangements, and socioeconomic backgrounds, and we provided thick contextual description to support interpretation beyond this setting. Second, as a descriptive interpretive qualitative study, the findings are not intended to be statistically generalizable. Instead, our goal was depth of insight. We strengthened credibility through prolonged engagement with the data, iterative team discussions, and triangulation between dyadic perspectives. Third, self-reported narratives carry risks of social desirability and recall bias. We minimized these risks by creating culturally sensitive interview environments, using open-ended prompts, and inviting participants to revisit or clarify their accounts throughout the interview. While dyadic interviews may have constrained disclosure of sensitive perspectives, they also allowed us to observe relational dynamics and cross-validate shared accounts.
Finally, researcher positionality may have influenced interpretation. To address this, we engaged in reflexive memoing, team-based coding, and questioning of assumptions throughout analysis. These steps helped ensure analytic transparency and rigor. Future research across varied geographic, linguistic, and cultural contexts within Black communities in Canada is needed to build on these findings.
Footnotes
Acknowledgement
We would like to express our gratitude to all those who contributed to this study, which was funded by the Labarge Catalyst Grant in Mobility and Aging at McMaster University, Hamilton, Ontario.
Ethical Considerations
Ethical clearance was granted for this study by the McMaster University: MREB#: 6403.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: However, the research upon which the manuscript is based was funded by a Labarge Catalyst Grant in Mobility in Aging from McMaster University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.