
Abstract
Background
E-learning has shown to be an effective intervention in helping informal caregivers of people living with dementia. It has the potential to reach people living in remote areas, increasing service coverage. As a response to the demographic context in Spain associated with a higher percentage of ageing, depopulation, and the complexities of health service delivery in rural areas, this paper describes the cultural adaptation and co-design of the iSupport online training and support programme for Castilla y León, Spain, as a potential e-health intervention to mitigate these constraints.
Methods
The translation and cultural adaptation were performed following the WHO guidelines, with some adaptation due to the cultural context of Spain. Three focus groups were conducted with informal caregivers, health professionals, and a group of experts on cognitive impairment and dementia. The co-design process was performed as a Patient and Public Involvement activity with three groups consisting of people living with dementia, informal caregivers, rural population and experts on technology and dementia.
Results
A total of 435 suggestions were proposed for adaptation associated with erroneous terminology, rewording text/writing, grammatical or punctuation marks errors, and repeated information or need for additional content. Several recommendations were exposed during the co-design process: preference for interactive material such as videos or images, a forum to receive feedback from health care professionals and to leave satisfaction comments, availability in multiple platforms (e.g., tablet, laptop, mobile), slide format for information presentation, and availability to edit letter size and background colours.
Conclusions
A culturally adapted version of the iSupport was developed for Castilla y León, Spain. The need for modification of words and expressions, information links to local resources websites, adjustments of characters’ names and caregivers’ scenarios, and additional content to some sections were recommended. Suggestions for the design should be taken into account for further adapted versions and platform developments.
Keywords
Background
Around 50 million people are living with dementia around the world and it is expected to increase to triple to 152 million by 2050 (Gauthier, Rosa-Neto, Morais, & Webster, 2021; Patterson, 2018). With an increase in the population living with dementia, which exponentially increases with ageing, duplicating the prevalence every five years after the ages between 65 and 69 (Villarejo Galende et al., 2021), it is to be expected a raise in the number of informal caregivers (Waligora et al., 2018).
It is estimated that 80–83% of the care is provided by family members, friends or unpaid caregivers (Alzheimer’s Association, 2016; Coduras et al., 2010), a role that often falls to women (Alzheimer’s Association, 2016; Pérez Diaz et al., 2020), and that 85% of the costs are related to the family (Gauthier et al., 2021; Ministerio de Sanidad, 2019). As the disease progresses, caring for a person with dementia becomes more challenging due to an increasing need for supervision and personal care (Alzheimer’s Association, 2016), which can lead to adverse health and financial effects and lower quality of life (Alzheimer’s Association, 2016; Casal Rodriguez et al., 2019; Waligora et al., 2018).
Supporting interventions for informal caregivers have shown improvements in quality of life and care (Dickinson et al., 2017; Naunton Morgan et al., 2022), reduction in caregiver burden, improve care service delivery or helping to cope with care responsibilities (Alzheimer’s Association, 2016) and have the potential to delay nursing and residential care (Alzheimer’s Association, 2016; Dickinson et al., 2017). E-learning has shown to be an effective intervention in helping informal caregivers of people living with dementia (Naunton Morgan et al., 2022), demonstrating some benefits on dementia knowledge and social support (Murray et al., 2005; Sitges-Maciá et al., 2021). It has the potential to overcome some constraints from in-person interventions, such as costs and transportation for assisting the sessions (e.g., people living in remote areas), inability to leave home because of caregiving role (Hattink et al., 2015; O'Connor et al., 2014; Wasilewski et al., 2017) and might help to increased service coverage (Pot et al., 2019).
The current demographic context in Spain, known as “emptied Spain”, refers to a relatively higher percentage of ageing and depopulation in rural areas and an increasing rural-urban migration, particularly of the youth. Service delivery in rural areas have been diminished and posed increasingly challenges (López González, 2021; Pérez Diaz et al., 2020). One of them is the access to support for informal caregivers of these regions. For this reason, considering the aforementioned benefits from e-learning and its significantly lower cost than other in-person and print modalities (Mitchell, 2011), we considered the adaptation and development of the iSupport online platform for the Spanish population as a potential asset to support and train informal caregivers of people living with dementia living in remote rural areas but also able to support any other regions with access to internet.
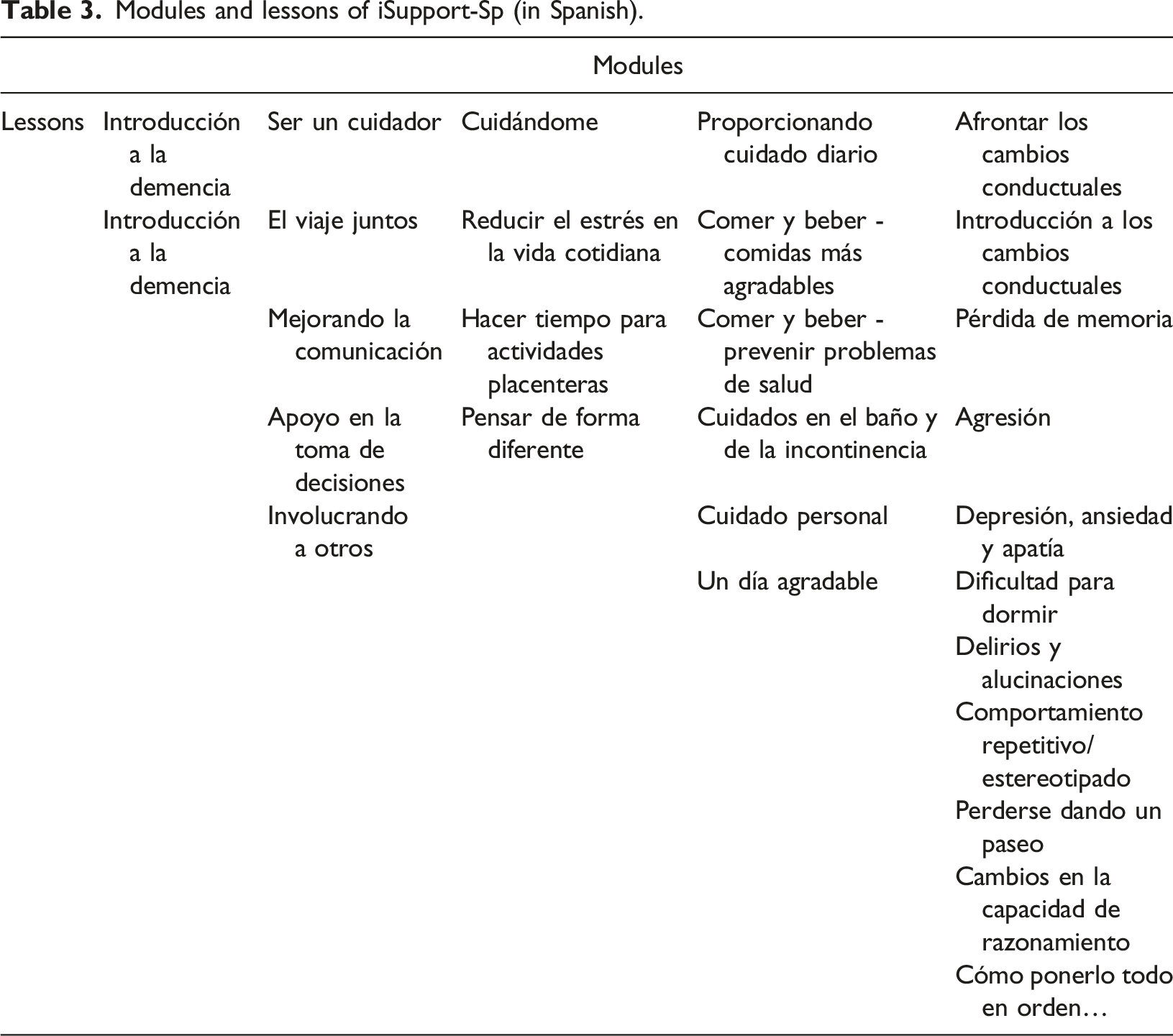
The iSupport is an evidence-based training and support program developed by the World Health Organization. It includes components of psychoeducation, relaxation, behavioural activation, cognitive reframing, and problem-solving (https://accesswho.campusvirtualsp.org/isupport-virtual-course-skills-and-knowledge-training-carers-people-dementia) (Pot et al., 2019; WHO, 2019a). It includes five modules: 1) introduction to dementia (1 lesson); 2) being a carer (4 lessons); 3) caring for me (3 lessons); 4) providing everyday care (5 lessons); and 5) dealing with behaviour changes (10 lessons). The primarily target audience are family members, relatives, friends, and other informal carers of people living with dementia (WHO, 2019a).
iSupport has already been culturally adapted in several countries and languages (e.g., Greek, Portuguese, or Chinese) and some of these projects have been published in the scientific literature (Baruah et al., 2021; Efthymiou et al., 2022; Teles et al., 2021; Xiao et al., 2022). This project aimed to culturally adapt the iSupport and co-design an online platform with people living with dementia, informal carers, and people from the target rural region of Castilla y León, Spain.
Methods
The translation and adaptation methodology was performed following the World Health Organization (WHO) Adaptation and Implementation Guide (available upon request from Translation and adaptation process (WHO, 2019b) and co-design parallel sessions.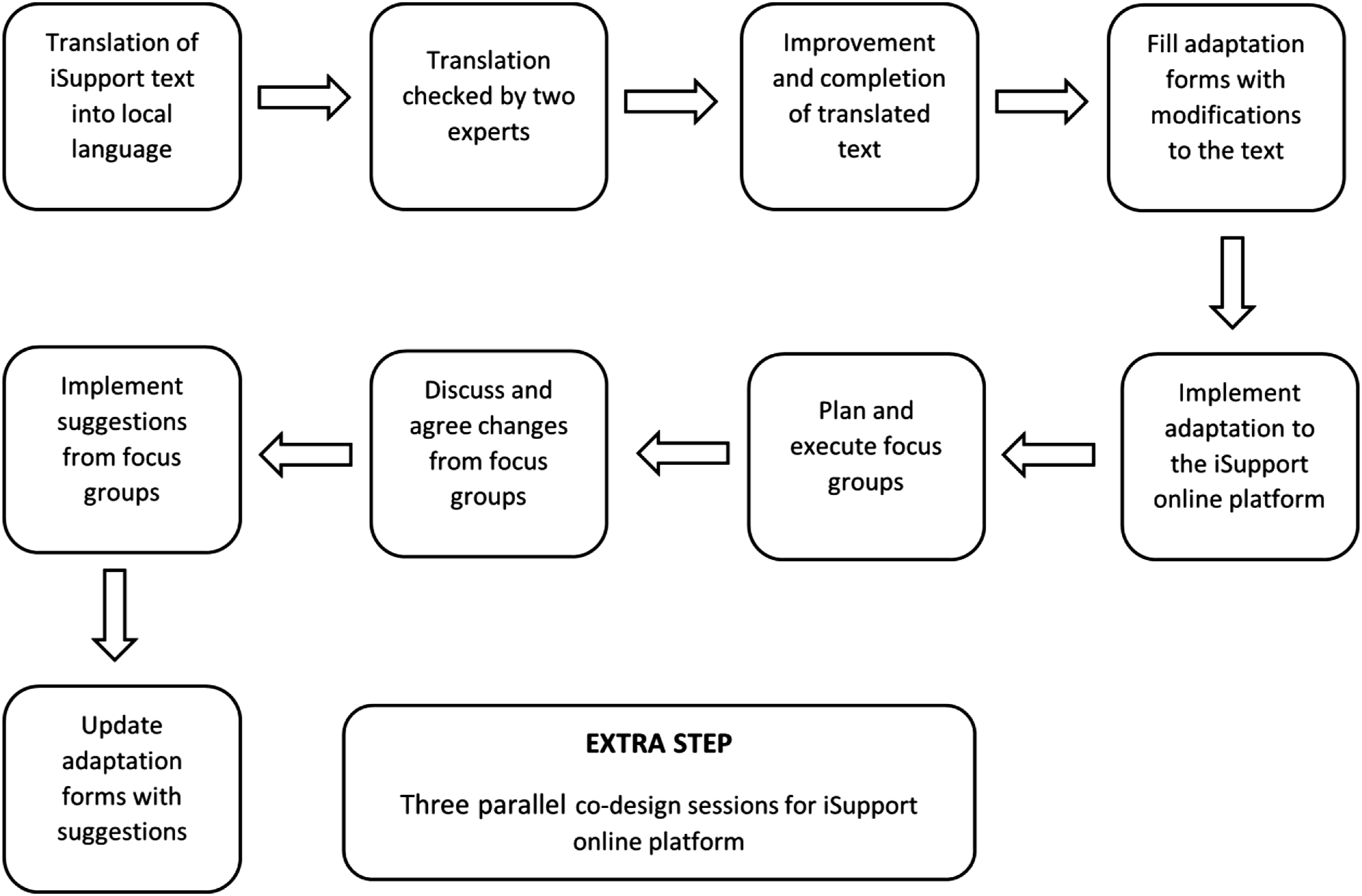
Translation by the authors
The translation was performed by MMU and MFM who have experience in the field of dementia and have previously worked with caregivers, which facilitates the translation of the technical vocabulary. Both authors are native Spanish speakers with a good level of English and familiar with the context of Castilla y León, Spain.
Cultural adaptation
A preliminary adaptation of the content was conducted by MMU and MFM following the Part B of the Adaptation and Implementation Guide, which describes suggestions to actual changes needed in the text or design of the online programme. This first step focused on modifying the words, names, links, and resources included in the iSupport generic version which are recommended by the Guide to be changed according to the local culture and habits. Changes to the text were included in the adaptation forms developed by WHO. Modifications to the content and text were included by the engineers LP and AB into the online version.
The next step was conducted to review the translated and adapted version and involved three focus groups with three different populations: a) informal caregivers; b) formal/professional caregivers; and c) a group of experts on cognitive impairment and dementia. We decided to involve this third group of experts as we consider they would give an extra value on how to adapt the content and the technical vocabulary to a more common use language targeting the population of interest. This step was performed by YGS who was a psychologist and local contact from the State Reference Centre for the Care of People with Alzheimer's Disease and Other Dementias.
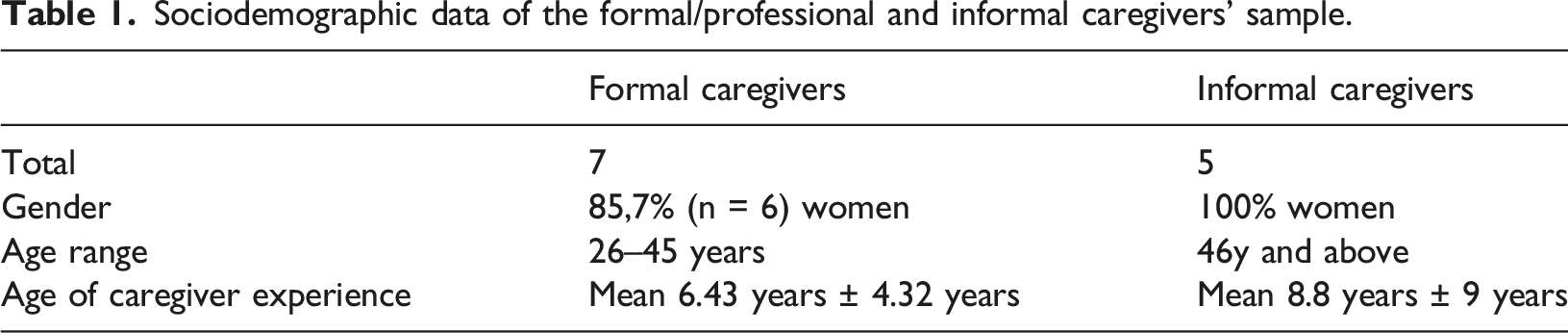
Formal/professional and informal caregivers were recruited from the State Reference Center for the Care of People with Alzheimer’s Disease and Other Dementias (Salamanca, Spain), while the group of experts were recruited from the master’s program of Dementia and Neuropsychology of the University of Salamanca, Spain (postgraduate fellows). The experts’ sample included 28 participants with an age range between 24 to 30 years.
Sociodemographic data of the formal/professional and informal caregivers’ sample.
For the groups of informal caregivers and formal/professional caregivers, two sessions of 90 minutes were performed. The first session included an explanation of the project and how to register the modifications in the adaptation forms; the second session was performed to collect the data from each of the participants and discuss the modifications suggested. For the group of experts, the methodology was slightly different as the data was collected by e-mail after a first session where MFM explained the purpose of the project and how to register the feedback. All participants had a two-week period to go through the iSupport content and fill the adaptation forms with their suggested modifications.
All modifications and changes registered through each participant adaptation form were collected and discussed in the focus groups. The final remarks from each group were collected and included in an adaptation form to compare all the results from the three samples. A thematic analysis approach was chosen for the analysis of the data. Codes were initially obtained according to the results of previously published iSupport cultural adaptations (Baruah et al., 2021; Efthymiou et al., 2022; Teles et al., 2021; Xiao et al., 2022). When new codes were identified, they were included in the analysis. Data were coded by YGS and MMU. When disagreements were identified, a third researcher (MFM) was involved in a final decision. Engineers were once again involved to update the platform according to the final modifications obtained from the focus groups.
All suggestions were analysed and are reported in the results, however, those that were identified as altering the meaning of the text or adding content beyond the original version were not added to the final adapted version. Decisions were made through consensus between MFM and MMU who were familiar with the iSupport content and based on their clinical experience.
Co-design
An additional step to increase the quality level of the design and adaptation process of the iSupport online platform was done in parallel to the translation and adaptation process. Three Patient and Public Involvement (PPI) extra sessions were performed with: a) the European Working Group of People with Dementia (EWGPWD), a group of people living with dementia and their carers with experience in research engagement (n = 3 caregivers; n = 5 people living with dementia); b) the Dementia: Intersectorial Strategy for Training and Innovation Network for Current Technology (DISTINCT), a group of researchers aiming to improve the lives of people living with dementia and their carers through technology (n = 25); and c) a group of people living in a rural area in Salamanca, Spain (n = 16), which eight of them were or used to be caregivers of people living with dementia at the moment of the meeting. Sessions were done individually with each group. The EWGPWD meeting was performed online through Zoom, with the DISTINCT Network and the rural population meetings were in-person. The time for the sessions varied from 20 to 40 minutes.
For the EWGPWD, the iSupport generic version was shown, and through a group discussion, participants gave feedback on how to improve the platform for adapted versions. For the DISTINCT Network and the rural area population, a prototype of the iSupport Spanish adapted version (iSupport-Sp) was shown and feedback from the participants was obtained and registered. All feedback was discussed between the project leaders and engineers to consider its inclusion. Decision for the inclusion of the recommendations were done according to the technological viability and the adaptation guidelines from WHO.
Ethics
This study was not subject to the Medical Research Involving Human Subjects Act. Advice was sought from the Chair of the Research Ethics Committee of Zamora Healthcare Complex. It was considered that REC approval to conduct this project was not required as no patients and vulnerable populations were intervened and because it was approached as a public engagement activity with all participants contributing as experts.
Results
Focus groups
Total suggestions to the content of iSupport, by sample group.
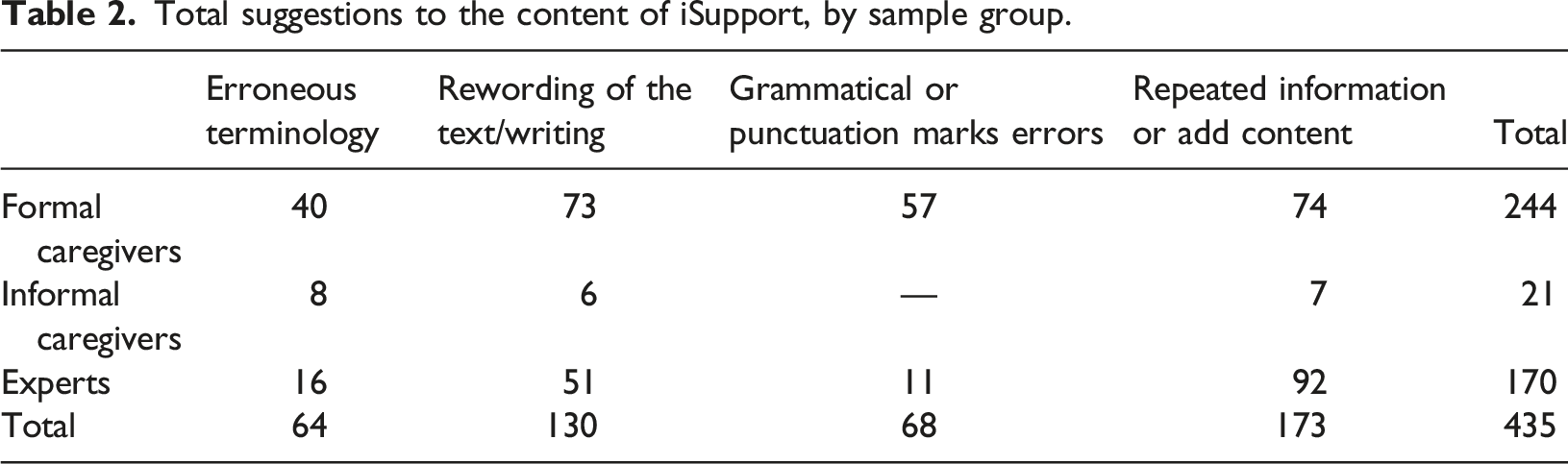
The following categories were used to organize the modifications or recommendations identified by the participants:
Erroneous terminology refers to words, terms, concepts, that when translated might not be the most recommended in the translated language. Some of the examples identified were the use of the word “compassion” or “approach” which had to be modified from the original translation for a more appropriate terminology:
“Delete the word compassion. Substitute for understanding” (FC2, FC4, FC5, FC6) (Lesson 2, Module 2).
“Delete ‘person with memory difficulties’. Substitute for ‘person with dementia/living with dementia’” (FC2, FC5, FC6) (Lesson 3, Module 2).
“Use the word understanding instead of compassion” (IC4)(Lesson 2, Module 2).
“Delete the word limitations. Substitute for ‘difficulties’” (FC5, FC7) (Lesson 3, Module 3).
“Change the word ‘condition’ for ‘situation’” (FC5) (Let’s look at an example, Lesson 3, Module 2).
“Delete the word miserable, it is not appropriate” (IC4) (Jo’s unhelpful and helpful thoughts, Lesson 3, Module 3).
“Delete the word ‘unhelpful’, shouldn’t be used” (FC1) (Lesson 3, Module 3).
Rewording of the text/writing included those sections where the participants considered that the translation is not correct, and writing must be changed for a better understanding. For example, some expressions that needed to be reworded according to the Spanish cultural context or changing the person’s name in the examples (e.g., Jonathan into Juan):
“Delete ‘let know your friends’. Substitute for ‘communicate to your friends/inform when you need to rest” (FC4, FC5, FC6) (Lesson 1, Module 2).
“Change the name Jessica for Juana” (FC5, FC6) (Lesson 1, Module 2).
“Change the name Jonathan for Juan” (FC4, FC2) (Check your understanding, Lesson 2, Module 2).
“Check the verb tenses. Questions have been formulated in a very complex way and are hard to understand” (FC6)(Lesson 1, Module 2).
“Change the time to the Spanish one. Around 10 at night” (FC5) (Activity, Lesson 5, Module 5).
Grammatical or punctuation marks errors are associated with all grammatical errors or erroneous use of the punctuation marks coming from the translation or a different used between English and Spanish. This was first checked during the translation process; however, participants identified some sections that needed to be fixed, such as:
“Check punctuation marks at the end of the first phrase” (FC3) (Check your understanding, Lesson 2, Module 2)
“Delete the commas after the word ‘father’” (FC5) (Check your understanding, Lesson 2, Module 2)
“Check punctuation marks. Some commas are in the wrong position and others are not needed) (FC6) (General remark to Lesson 2, Module 2)
“Use bullet points or dashes for better understanding” (FC1, FC3) (Check your understanding, Lesson 3, Module 3)
Repeated information or add content refers to the feedback associated to a perceived repetition of the information along the text and the modules, and the perceived lack of information in several sections of the modules or the need to include relevant information according to the Spanish context or another presentation modality of the information (e.g., video or image instead of text), for example the use of links to the local public health services or associations working with people living with dementia. Another example was to include videos and audio material to help the users with the relaxation activities. In terms of additional information for clarification of the section, an example is the need for more information explaining the section of “repetitive behaviours”. Some examples are:
“Write an introduction about relaxation in the section (relaxation section) before reading the example directly, to put the reader in context” (FC2) (The importance of relaxing, Lesson 1, Module 3)
“Add more information to this section, it is incomplete” (FC3) (Which of your activities can you do today, Lesson 2, Module 3)
“The design could be presented through audio, videos or illustrations that facilitate the understanding and execution (relaxation exercise) of the person who will implement the activity” (Expert 1) (Relaxation Exercises, Lesson 1, Module 3)
Modules and lessons of iSupport-Sp (in Spanish).
For all the modules, repeated information and the need for additional content was the most prominent suggestion. Module 2 received the most comments. For Modules 4 and 5, no comments were recorded from informal caregivers.
Co-design
Summary of suggestions made during the Co-design step.
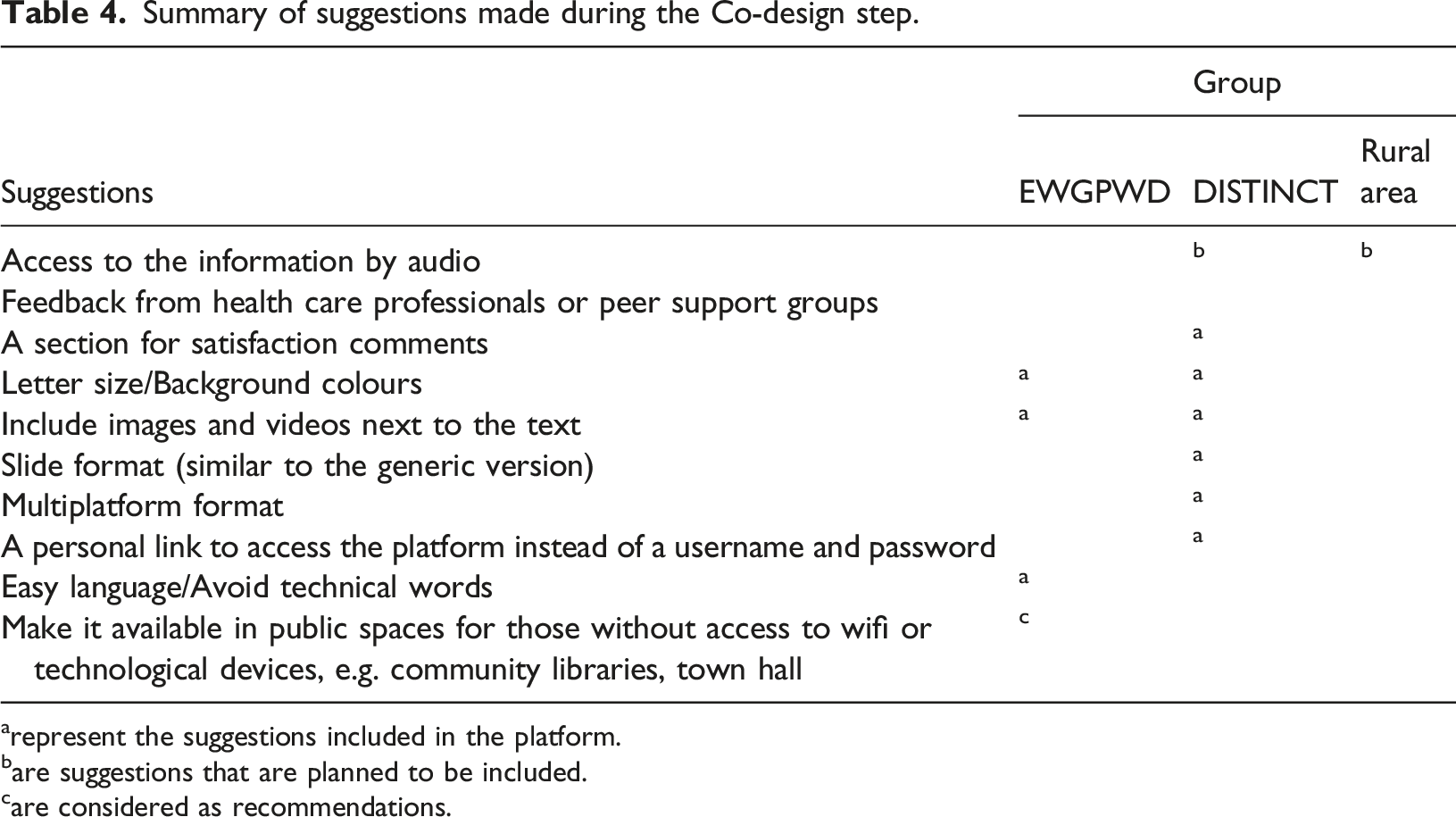
arepresent the suggestions included in the platform.
bare suggestions that are planned to be included.
care considered as recommendations.
Experts, people living with dementia and caregivers suggested to include the ability to change the colours and font, allowing the users to select the best combination to their own preferences. They mentioned that a standard black and white combination might not be the best selection for everyone. Additionally, they considered that information can be offered in video format besides the written material or just video instead of text, as some carers mentioned to prefer videos over reading. Similarly, the experts and the rural area group considered, as an added value, if the information can be accessed also by audio.
Additional recommended features were the possibility to exchange feedback with health care professionals or a peer support group, to leave satisfaction comments regarding the use and content of the online platform, and to make it available for multiple platforms (e.g., mobile, tablet, laptop) as it was difficult to navigate in other devices other than a laptop. Also, experts considered important to keep the slide format presentation of the generic version instead of the continuous text to avoid an overload presentation of information.
Two recommendations, one from the experts and the other one from the EWGPWD, were considered as relevant for future implementations due to other technological requirements or because it depends particularly on the region it will be implemented. The use of a personal link, instead of username and password, could facilitate the access to the content and avoid difficulties remembering the required information. In terms of making the platform accessible in community facilities (e.g., libraries, hall) it came as suggestion for those lacking access to technological devices or Wi-Fi, which can be implemented according to each community.
iSupport-Sp online platform
Considering the previous results, we came up with the iSupport Spanish online version (iSupport-Sp). The platform is provided by a Learning Management System which allows creating and integrating course materials, articulate learning goals, align content and assessments, get users feedback, and track studying progress to make it easier for the learner and facilitator. It also incorporates dashboards to track users’ progress. Therefore, it can then report on key items such as completion rates, attendance data and success likelihood. Utilizing these metrics can help facilitators better understand gaps in user knowledge.
iSupport-Sp is carried out via the consumption of text in slideshows format with customized activities in the form of a variety of different question types such as: one/multi-line answer; multiple choice answer; ordering; free text; matching; essay; true or false/yes or no; fill in the gaps; and agreement scale; and it also includes links to videos for better understand the content of the courses. Thanks to the availability of these resources, it facilitates a self-paced learning process.
iSupport-Sp was developed in WordPress using the online training plugin LearnDash and the Enfold theme. It is hosted in a cloud system (isupport.bluece.eu) following a software as a service model. All data is stored by the facilitator’s own resources and accessed by users through the internet connection. It can be accessed via most electronic devices including a computer, laptop, tablet, or smartphone, making it a versatile and easy way for users to learn wherever they are. iSupport-Sp is available upon request to the authors as it will be under study for its feasibility and usability.
Discussion
As an attempt to offer a support service alternative for informal caregivers of people living with dementia in remote rural areas in Spain, this project aimed to present the cultural adaptation of the iSupport training and support programme for carers of people living with dementia for the region of Castilla y León, Spain. Additionally, it describes the co-design process of the online iSupport platform with people living with dementia, informal carers, and people from the target rural region.
A total of 435 suggestions for modification were done by the experts on cognitive impairment and dementia and the formal and informal caregivers, who provided approximately 5% of all remarks. Most of the adjustments were associated to a) repeated information (e.g., repetitive vocabulary throughout the text) or the need to add more content to introduce some sections, and the lack of information for specific topics; and b) the need for rephrasing the text or the writing to adjust it to the cultural context. Other considerations were related to grammatical or punctuation mark errors and the use of erroneous terminology (e.g., exact translation needed to be modified to a more common term to the culture). Not all suggestions could be added to the final adapted version because some of them would change the text meaning or add more information that differs from the original version. For this reason, it was necessary to filter the suggestions, especially those identified under the code “Repeated information or add content”. Nonetheless, we consider it important to report all suggestions as this could be relevant for further development and improvement of the iSupport lessons and modules.
Similar remarks were provided in previous adaptations to Greek, Portuguese, Chinese-Australian and the Indian culture (Baruah et al., 2021; Efthymiou et al., 2022; Teles et al., 2021; Xiao et al., 2022). Changes associated with definitions, semantic and conceptual expressions, cultural adaptation of caregivers’ scenarios, resources according to the local context (e.g., link to local institutions and websites), characters with common names according to the culture, clarity and precision of concepts and titles, and additional content regarding severe stages of dementia and more scenarios for the behavioural disorders sections, are some of the remarks identified across the previous studies that might account for all (future) adaptations. Even when the implementation is done in the same language (e.g., the English generic version to Indian culture, or the Spanish generic version to Spain culture), it has been recognized the need for several modifications on this regard (Baruah et al., 2021).
Even though WHO provides an adaptation guideline (WHO, 2019b), the adaptation processes have differed slightly between India, Portugal, Greece, Chinese-Australians and the one reported in here (Spain). According to the literature, the Greek and Chinese version (Efthymiou et al., 2022; Xiao et al., 2022) and our adaptation process have followed the recommended step of conducting two focus groups, one with informal caregivers and one with health or social care professionals caring for people living with dementia. This step aims to review the translated and adapted first attempt to obtain a better result according to the local context. For the Indian version, they performed face to face interviews and an online test run with caregivers (feedback was sent to the research team through emails) (Baruah et al., 2021) and in Portugal, this step was performed only by a group of experts on ageing, dementia and psychosocial and/or psychological support for informal caregivers of people living with dementia (Teles et al., 2021). These slight diversion between the adaptation processes is something to consider for better results on the new adapted versions. The differences might not be relevant in terms of the core components of the iSupport generic version. However, they might have an impact on the adequate process to obtain an appropriate local version. For example, the absence of either a focus group of local informal caregivers or health and social care professionals could omit the view from the important stakeholders to whom the intervention is addressed, that could improve the cultural adaptation and make the content of the iSupport more valuable for the target users. This limitation was already mentioned by Teles et al. (2021) as they lack from the informal caregivers’ perspective during the review of the first cultural adapted attempt of the Portuguese version.
Consequently, for providing a more standardized version of the iSupport across countries, aiming to perform a cross-cultural study on its efficacy and effectiveness on several outcomes of informal caregivers, it is important to follow the adaptation guide provided by WHO. Nonetheless, the counterpart of this suggestion is the lack of flexibility if one of the steps is not feasible in a specific region because of lack of resources or cultural reasons. In this project, for example, the representation of male informal caregivers did not follow the recommendation of the Guide (50/50 male to female ratio) as the care responsibility mainly falls on women according to the context of caregivers in Spain (Pérez Diaz et al., 2020).
Regarding the co-design of the online iSupport platform for Spain, several recommendations not included in the generic version were exposed (Table 4). Some of them are aligned to the suggestions proposed by the focus groups in the Greek and Chinese-Australians version, such as a preference for interactive versions that include videos and a forum to receive feedback from health care professionals or a peer support group (Efthymiou et al., 2022; Xiao et al., 2022) or for satisfaction comments (according to our results), changes to the navigation style, which associates to our recommendation on keeping a slide format style to present the content instead of scrolling down the text (Efthymiou et al., 2022), the possibility to develop an alternative audio format, or facilitating the access to the platform by using voice recognition or key words search (Xiao et al., 2022), similar to our suggestion of using a personal link without the need of a password. No other recommendations were identified in other studies regarding the design of the platform.
The iSupport-Sp introduced by this project is provided via e-learning which has numerous advantages in terms of enhancing the health care service provision and enabling remote areas to access them, as otherwise it would be needed to incurred in travel costs or leave aside, in this case, caregiver responsibilities (Klimova et al., 2019; Ritterband & Tate, 2009). Also, they have shown to be cost-effective in comparison to other modalities (Dickinson et al., 2017; Mitchell, 2011) and they have the potential to offer multimedia information delivery (e.g., videos and links to access relevant websites), which has been considered relevant to potentiate learning and making more engaging content (Ruiz et al., 2006).
These advantages are especially beneficial for informal caregivers as often they are limited and restricted in time, cannot leave caregiver responsibilities or undertake other several daily duties such as employment, caring for other family members (e.g., children) or housework (Serafini et al., 2007). The only requirement is an internet connection to be able to access iSupport learning materials through a web browser and in a slide-based format at any place and time removing the geographical obstacles often associated with traditional classrooms and education.
Despite of these benefits, we are also aware of some limitations that must be considered for future versions. The most effective interventions in supporting caregivers consist of multiple components, such as cognitive behavioural therapy and relaxation strategies, educational resources, online peer support groups, and also sessions with person tailored elements (e.g., telephone contact) (Naunton Morgan et al., 2022) and interaction with health professionals (Sitges-Maciá et al., 2021). This mixture of interventions and methods delivery seems to be a key for better results, however, the iSupport-Sp is lacking elements such as online peer support, contact with health care and more personal elements. These considerations should be taking into account to incorporate in future adapted versions of the iSupport.
Strengths, limitations, and further research
The strength of this project relies on the diverse populations included during the different stages which enriches the suggestions and recommendations either for the cultural adaptation or the co-design of the online platform. Along the process, the views, and insights from people living with dementia, informal caregivers, health professionals, experts on cognitive impairment and dementia, caregivers and residents from a rural population in Spain, and experts on novel technologies to improve quality of life of people living with dementia and informal caregivers, were considered for the final adapted version of the iSupport-Sp. We hope that this diversity of perspectives offers a more feasible and user-friendly training and support programme to informal caregivers in Spain.
Regarding the population involved in the project, there are three remarks to notice. First, informal caregivers were least represented in the cultural adaptation (n = 5). This underrepresentation may have affected the inclusion of the perspectives of informal caregivers during the review of the first translated and culturally adapted content. In fact, Table 2 shows that informal caregivers’ suggestions were far fewer than the other stakeholder groups, leading to an imbalance between the perspective of the three groups involved in this adaptation. Second, the same group was not representative for a rural population, which is the main target group for this adaptation. Nonetheless, the participants were residents of the region where this iSupport version has been adapted for. A rural representation was involved in the co-design of the platform. Third, the representation of male caregivers during the focus groups for the cultural adaptation was very limited (n = 1). However, this is very much representative for the context of caregivers in Spain, where the care responsibility falls mainly on women (Pérez Diaz et al., 2020).
The adaptation guide provided by WHO (2019b) includes an adaptation template to register all suggestions and modifications that must been delivered once the process is finalized for a fidelity check by the responsible of WHO. Despite the usefulness of these templates, it is difficult to manage and train participants in the focus groups to register the feedback in the templates, while also checking the content of the iSupport. For this reason, we provided a printed version of the iSupport and the templates, considering that filling the registrations by hand might be easier for some subgroups than digitally. We assumed that digitally filling the forms might especially burdensome for informal caregivers, and care professionals with lower computer literacy. It is important to notice that by the time this project is published, a Spanish generic version of the iSupport was developed by WHO (https://www.campusvirtualsp.org/es/curso/isupport-capacitacion-sobre-aptitudes-y-conocimientos-para-quienes-cuidan-de-personas-con). This version was not used for this adaptation as was not available at the time this project started. Considering this, the whole process of translation was required and the adaptation to the context of Spain, specifically for Castilla y León, is unique for the version presented in this project.
The culturally adapted iSupport-Sp on the new online platform will be tested in a usability/feasibility study with informal and formal and professional caregivers. Subsequently, a pilot study with pre- post-test assessments will be executed. The results of this pre-experimental design will serve the design of a future randomized controlled trial.
Conclusion
This study describes the Spanish cultural adaptation process of the online iSupport training and support programme. A diverse group of stakeholders was involved in the adaptation and co-design process, which impacts the quality of the adaptation to the local standards.
The cultural adaptations published in the literature in other countries and the one provided here converge on the need for modification of words and expressions, information links to relevant websites, characters’ names and adjustments of caregivers’ scenarios, and additional content is recommended for some sections. Some deviations were identified from the methodologies advised for the cultural adaptation. It is recommended to stick to the adaptation guideline provided by WHO for a more standardized version of the iSupport across countries.
Relevant recommendations for the design of the online platform were identified. More interactive sessions including videos and audio, a forum to receive feedback from health professionals, the option to leave satisfaction comments, availability on multiple devices (e.g., tablet, laptop, mobile), slide format for information presentation, and the option to change letter size and background colours, were some of the suggestions recorded.
Further research should study the usability and feasibility, and efficacy and effectiveness of the iSupport-Sp platform in informal caregivers.
Footnotes
Acknowledgements
Special thanks are due to the members of the EWGPWD, the DISTINCT Network, and the residents of the rural town from Salamanca who were engaged during the co-design of the Spanish version of the iSupport online platform.
Authors’ contribution
MMU, the executive researcher of the project wrote the first draft of the manuscript. MMU, MFM and YGS substantially contributed to the study design and to the acquisition, analysis, and interpretation of data. LP and AB contributed to the development and improvement of the iSupport online platform according to the suggestions from the results. All authors substantially contributed to the conception of the work and the final revised version of the manuscript. All authors have approved the submitted version that involved the author’s contribution to the study and have agreed on both to be personally accountable for the author’s own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the the European Union’s Horizon 2020, as part of the Marie Skłodowska Curie Actions - Innovative Training Network, H2020-MSCA-ITN [under grant agreement number 813196]; and the Spanish Ministry of Science and Innovation under the PeaceOfMind project [ref. PID2019-105470RB-C31].
Ethical approval
This study was not subject to the Medical Research Involving Human Subjects Act. Advice was sought from the Chair of the Research Ethics Committee of Zamora Healthcare Complex. It was considered that REC approval to conduct this project was not required as no patients and vulnerable populations were intervened and because it was approached as a public engagement activity with all participants contributing as experts.