
Abstract
Introduction
The World Health Organisation (WHO) has developed iSupport for Dementia, a self-paced online training programme for caregivers of people with dementia which is adaptable to different cultural contexts. This scoping review aims to understand the iSupport adaptation process in different countries and provide recommendations for future adaptations.
Methods
A systematic search was done in electronic databases such as Pubmed, MEDLINE, APA PsycINFO, and EMBASE to obtain relevant publications up to 18 February 2024. Only full-text publications describing iSupport cultural adaptation process were included. The publications obtained were reviewed using the Cultural Adaptation Process framework.
Results
Thirteen publications from ten studies were eligible for inclusion. Based on the Cultural Adaptation Process framework, the steps undertaken in the studies were grouped into: (i) setting the stage, (ii) initial adaptation, and (iii) adaptation iterations. The three significant players in this process are the intervention developer (researchers), the cultural adaptation specialist (researchers, caregivers, and dementia care professionals), and the target community (caregivers). In the publications reviewed, cultural adaptation was mostly undertaken using a co-design process between researchers, caregivers, and dementia care professionals deciding on necessary modifications.
Conclusion
iSupport for Dementia is a versatile programme to support caregivers and is readily available for adaptation to different cultural settings. It is essential to engage caregivers early in co-designing its cultural adaptations to ensure their needs can be met by this online tool.
Introduction
Dementia is a major cause of disability which can hugely impact quality of life. In 2019, an estimated 57.4 million people were living with dementia worldwide, and projected to grow to over 152.8 million in 2050 (Nichols et al., 2022). Most of this increase in dementia prevalence will occur in low-and-middle-income countries (LMICs) due to their ageing demographics (Global status report on the public health response to dementia, 2021). In addition, the economic burden of dementia is substantial, estimated at US$1,313.4 billion in 2019 (Wimo et al., 2023), which means the projected rise to US$2 trillion by 2030 (Prince et al., 2015) will most likely increase. In the UK, the costs of health and social care for dementia are equivalent to the combined costs of cancer, heart disease, and stroke (Luengo-Fernandez et al., 2010; Prince et al., 2015).
Apart from direct medical and social care costs, unpaid care costs of dementia are also significant. In LMICs, unpaid care costs amounted to US$220.6 billion in 2019, constituting the majority (64.7%) of dementia care costs. This cost is also substantial in high-income countries, reaching US$430.8 billion (44.3% of total dementia cost) (Wimo et al., 2023).
Most dementia care is provided by unpaid family caregivers who have very little training for the task (Burgdorf et al., 2019). Studies have shown that dementia education and psychosocial support for caregivers could be effective in addressing changes in behaviour, improving quality of life, and promoting caregiver well-being (Livingston et al., 2017; Livingston, Huntley, et al., 2020). Family caregivers’ experience in caregiving has been shown to influence the quality of life and well-being of the person living with dementia (Quinn et al., 2020); therefore, the provision of support for family caregivers of people with dementia is critical. Many caregiver interventions with psychological components have been developed, but the availability and quality of evidence are variable. However, effective interventions are usually structured, systematic, multimodal, and involve caregiver education (Livingston et al., 2017).
Caregiver education can reduce behavioural and psychological symptoms of dementia, caregivers’ depressive symptoms, and caregivers’ burden (Livingston et al., 2017; Terayama et al., 2018). One of the first psychoeducation interventions, Coping with Caregiving (CWC), includes ten weekly sessions and eight monthly boosters (Wisniewski et al., 2003). Comprehensively evaluated in the Resources for Enhancing Alzheimer’s Caregiver Health (REACH) study, CWC reduced depression among caregivers from various US ethnic communities (Livingston et al., 2014; Schulz et al., 2003). REACH II developed this into a structured multi-modal intervention (information, education, and phone support) tailored to individual risk profiles, improving caregivers’ quality of life and reducing residential long-term care admission (Belle et al., 2006; Elliott et al., 2010). STrAtegies for RelaTives (START), a UK-developed psychoeducation intervention, consists of eight sessions over 8–14 weeks, often delivered at home. Widely implemented in the UK, START is cost-effective (Knapp et al., 2013) and reduces anxiety and depressive symptoms for up to 6 years (Livingston, Manela, et al., 2020). However, caregivers from different cultures might find these Western-developed programmes unsuitable linguistically or culturally.
Translating, developing, and adapting evidence-based programmes is a lengthy and resource-intensive process. For example, there is a ten-year lag time between the development of START and the adaptation of the programme for other cultures living in the UK (Livingston et al., 2013; Webster et al., 2023). In addition, these programmes have limited reach as they are designed to be delivered by a healthcare professional or support worker. Family caregivers need a resource that they can use at their own convenience at any time.
The World Health Organisation (WHO) launched a Global Action Plan on the Public Health Response to Dementia in 2017 and declared the importance of support for caregivers as one of the action areas (Global action plan on the public health response to dementia 2017-2025, 2017). The WHO recognised the urgent need for easily accessible education-based caregiver interventions and developed the ‘iSupport for Dementia’ to support member countries in providing accessible information and training to strengthen caregivers’ knowledge and skills (iSupport For Dementia. Training and support manual for carers of people with dementia, 2019). This self-paced online training programme for unpaid caregivers of people with dementia is adaptable to different cultures and comprises of five modules (Introduction to dementia, Being a carer, Caring for me, Providing everyday care, and Dealing with behaviour changes). It aims to improve caregivers’ quality of life and minimise health problems resulting from caregiving burdens (Pot AM et al., 2019). Although conceptualised as an online training, a manual book in PDF format is also available to download from the WHO website for areas with low internet coverage (https://www.who.int/publications/i/item/9789241515863) (iSupport For Dementia. Training and support manual for carers of people with dementia, 2019).
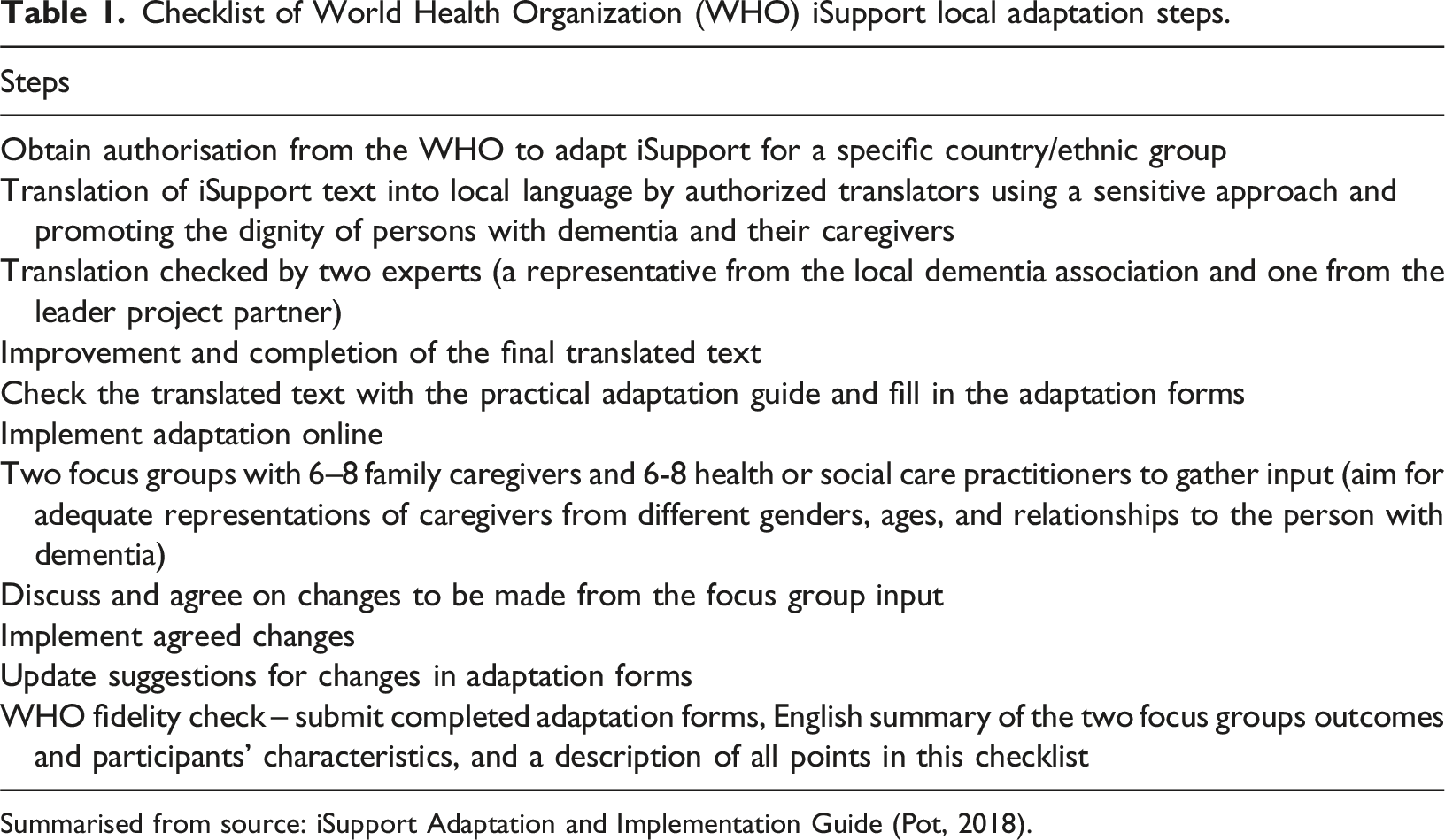
Adapting an intervention to the appropriate context and culture is important to ensure iSupport’s usability in different cultural contexts (Bernal et al., 1995; Gearing et al., 2013; Pot et al., 2019). The WHO recognises the importance of this ecological validity and has provided guidance on adapting iSupport (Pot, 2018). Figure 1 outlines the steps for the local translation, adaptation, and implementation of iSupport based on WHO’s guide. It underscores the iterative nature of the process, involving caregivers and stakeholders in the design. Early collaboration with local stakeholders is strongly recommended to secure local caregivers’ trust and acceptance of the instrument. These may include health practitioners, civil society organisations (including local dementia association), traditional healers, religious and political leaders, and researchers from local universities (Pot, 2018). The WHO provides practical guidance in each module where adaptation may be needed (e.g., names, expressions, local practices, and resources). There are also forms to report changes undertaken in the adaptation process to the WHO (Pot, 2018). Table 1 shows a checklist of the WHO’s recommended steps in translating and adapting iSupport to local cultures, derived from the iSupport Adaptation and Implementation Guide (further referred to as the WHO adaptation guide in this review) (Pot, 2018). Essential steps for local translation, adaptation, and implementation of iSupport based on the WHO adaptation guide. Source: iSupport Adaptation and Implementation Guide (Pot, 2018) Used with permission from the WHO. Checklist of World Health Organization (WHO) iSupport local adaptation steps. Summarised from source: iSupport Adaptation and Implementation Guide (Pot, 2018).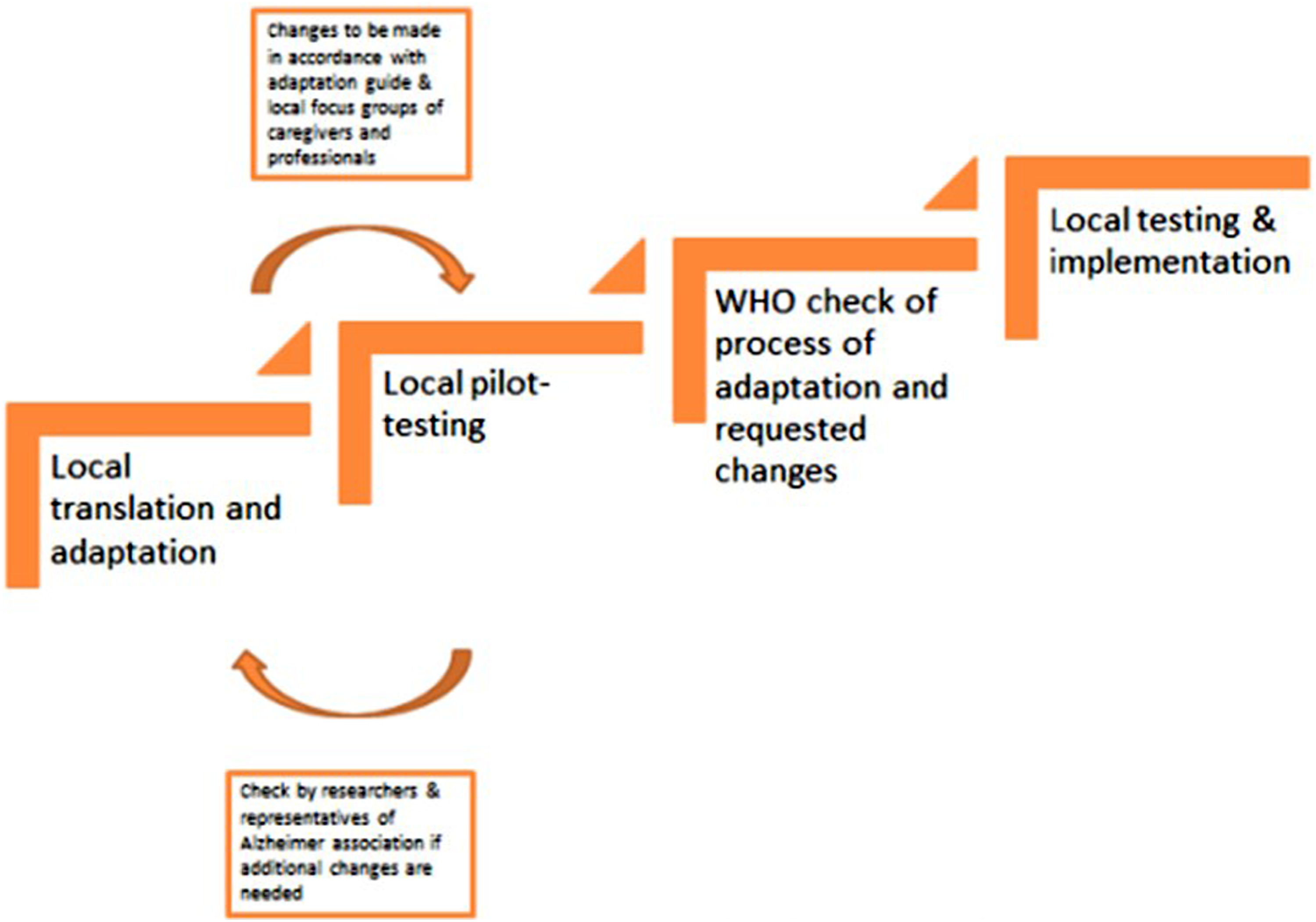
Aim
Research initiatives have taken place in different countries to adapt iSupport to the local context. As of May 2023, adaptation processes of iSupport are taking place in 39 countries, covering 36 languages (Seeher, 2023). This scoping review aims to understand the adaptation process in different countries, explore best practices, and provide recommendations for future adaptations.
Methods
Study design
This scoping review followed the guidelines of the Joanna Briggs Institute (Peters et al., 2024) and the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) Extension for Scoping Reviews (PRISMA-ScR) checklist (Tricco et al., 2018).
Search strategy
TS conducted systematic searches in April 2023 and updated on 18 February 2024 using the following electronic databases: Pubmed, MEDLINE, APA PsycINFO, and EMBASE. Search alerts were set up in all databases to ensure ongoing retrieval of relevant studies. Keywords used were: [‘Dementia’ AND ‘iSupport’] and [‘WHO’ AND ‘iSupport’]. References of included papers were screened manually for other relevant studies. There was no restriction on publication years.
Selection criteria
We included papers describing the cultural adaptation process of the WHO iSupport for Dementia to a specific country/culture. Only papers published in English were included. Exclusion: (1) protocols; (2) conference proceedings without full-texts; (3) papers that only describe implementation stages (such as usability, acceptability, feasibility, or effectiveness studies); (4) other types of papers which do not describe results from an original adaptation study, including but not limited to: literature reviews, letter to editors, opinion paper; (5) adaptation of the derivations of iSupport for Dementia programme, such as iSupport-Lite (educational posters developed based on the iSupport programme).
TS and a research assistant independently examined abstracts without full-texts for the content and manually cross-checked to ensure no duplicated results. The full-texts of all papers meeting the selection criteria were reviewed by TS to decide on inclusion and to extract data.
Data extraction and synthesis
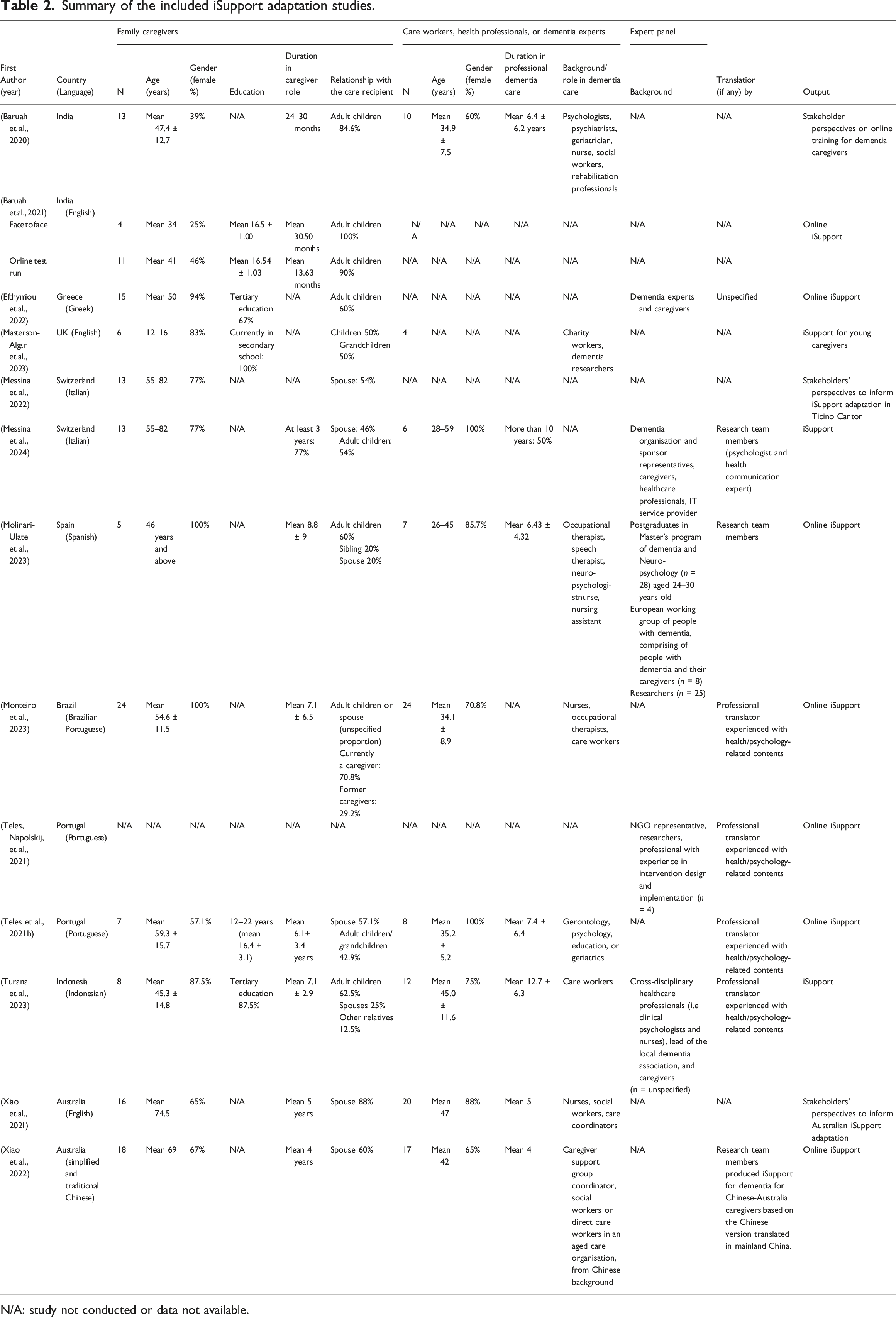
Summary of the included iSupport adaptation studies.
N/A: study not conducted or data not available.
This scoping review was reported using the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. We performed a quality assessment of the studies’ methodologies with the Mixed Method Appraisal Tool (MMAT version 2018), which was developed to appraise studies included in systematic mixed studies reviews (Hong et al., 2018). We reported included studies using the Cultural Adaptation Process (CAP) framework because of the WHO’s emphasis on involving caregivers as target users, and it best reflects the steps described in WHO’s checklist in Table 1.
The CAP describes three significant players in a cultural adaptation work: the intervention developer, the cultural adaptation specialist, and the target community (Domenech-Rodríguez et al., 2011; Domenech-Rodriguez & Wieling, 2004). The CAP framework divides the adaptation process into three phases: (i) setting the stage - the three players are identified and collaboration between them ensued in assessing the needs for adaptation; (ii) initial adaptation - a priori adaptation is done by the intervention developer and the cultural adaptation specialist, then tested by members of the target community; and (iii) adaptation iterations - required changes identified in phase (ii) are realised and iteratively refined. This framework has been used in culturally adapting dementia psychoeducation programmes, such as the START programme for Black and South Indian caregivers in the UK, which has been shown acceptable and feasible to deliver in these communities (Webster et al., 2023).
Results
The search strategy identified 97 records (Figure 2). TS and the research assistant screened the records (titles and abstracts) independently to remove duplicates. After duplicate removal, there were 35 records. Fifteen records were removed due to being book chapters, protocols, or conference proceedings with insufficient information. Full-texts of the remaining 20 records were assessed for eligibility. A total of eight records were excluded for the following reasons: four implementation studies, two non-cultural adaptation studies, one study on iSupport-Lite adaptation, and one letter to editors. During this full-text screen, a reference cited in one of the eligible papers emerged as fulfilling our selection criteria and was included. Ultimately, thirteen articles on adaptation studies were included in the review. PRISMA Flow diagram.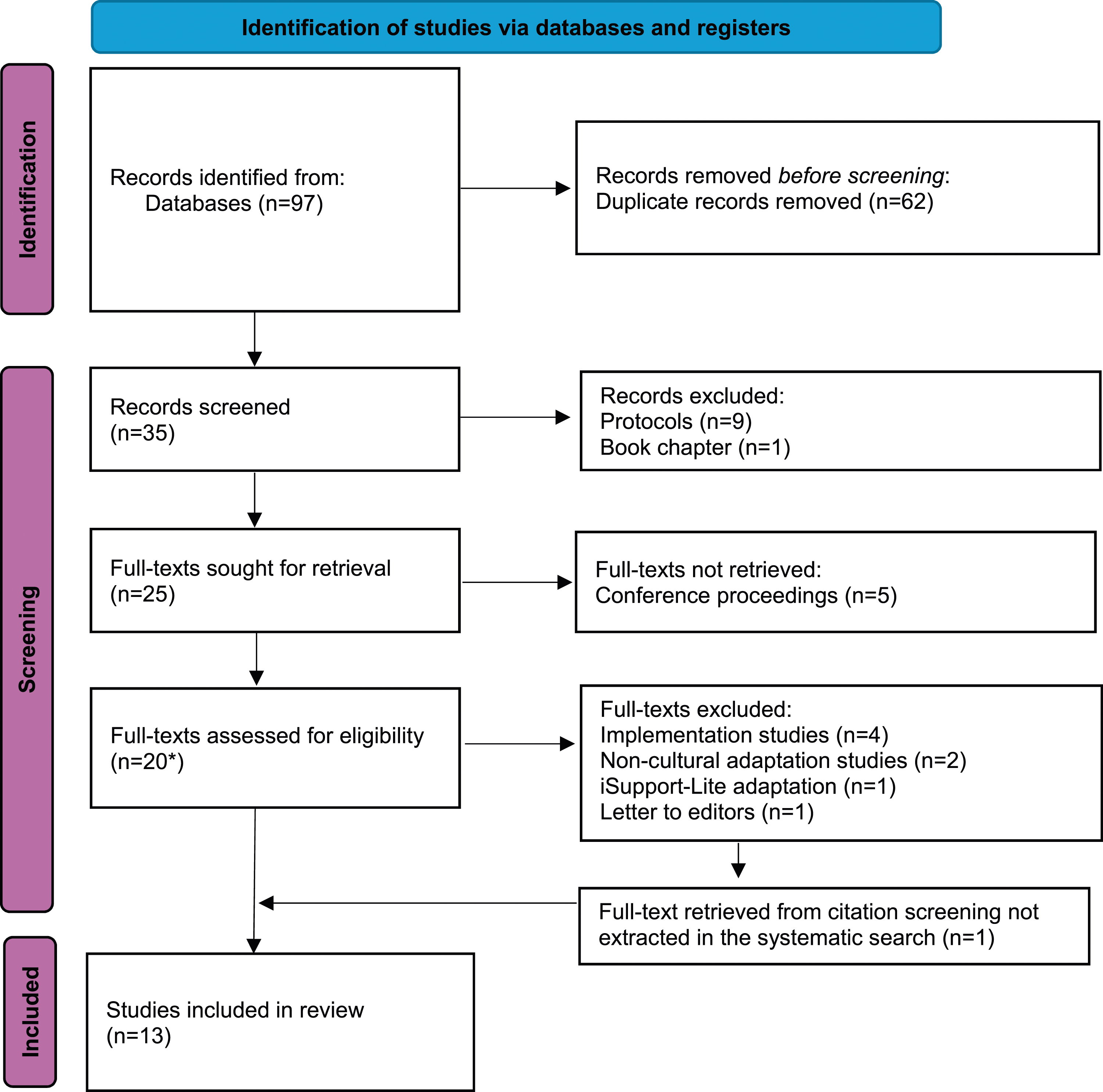
Thirteen publications from ten studies were included in this review. These publications were from Australia (n = 2), Brazil (n = 1), Greece (n = 1), India (n = 2), Indonesia (n = 1), Portugal (n = 2), Spain (n = 1), Switzerland (n = 2), and the UK (n = 1). There were two independent adaptations in Australia, one for English-speaking Australian caregivers (Xiao et al., 2021) and one for Australian-Chinese caregivers (Xiao et al., 2022). All adaptation studies aimed to develop a culturally relevant version for unpaid caregivers of people living with dementia. The studies conducted in India and Switzerland added an additional step where they first assessed local stakeholders’ perspectives on the use of online-based dementia training (Baruah et al., 2020; Messina et al., 2022) then described the preliminary adaptation design, test, and refinement process in the next paper (Baruah et al., 2021; Messina et al., 2024).
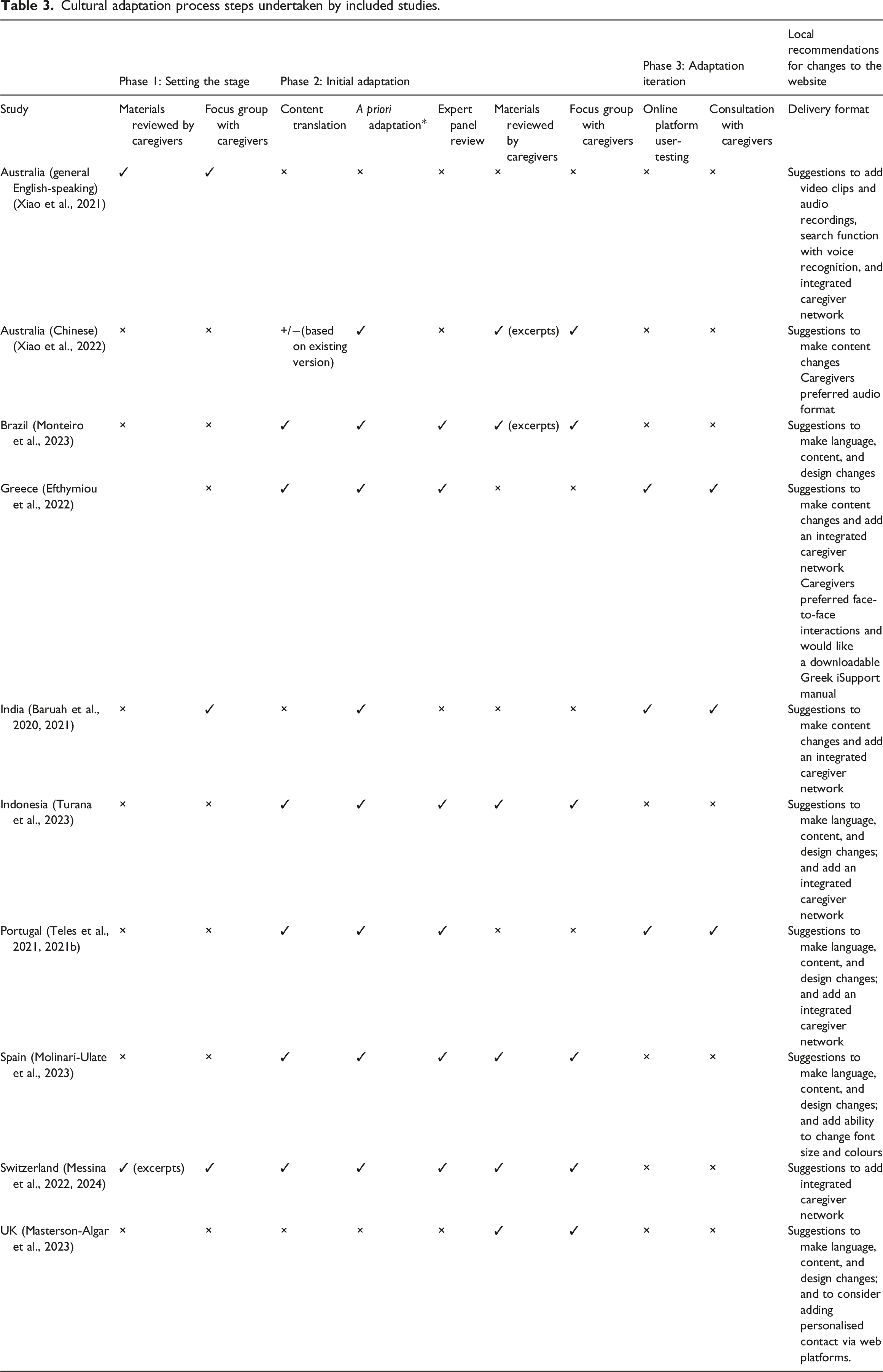
Cultural adaptation process steps undertaken by included studies.
Phase 1: Setting the stage
This stage involves initial work between the intervention developer, the cultural adaptation specialist, and the target community, in identifying the need for adaptation. In the iSupport adaptation studies identified, the intervention developers were researchers. The cultural adaptation specialists varied across studies as this role was undertaken by the co-design process where researchers, caregivers, and in some cases care professionals, came together to decide on necessary changes. The target community was unpaid caregivers, the primary users of iSupport.
Only Australia, India, and Switzerland involved caregivers in setting the stage. In these three studies, the intervention developers set the stage by conducting a needs assessment through focus groups with caregivers acting as cultural adaptation specialists and target users before making any changes to iSupport for their countries. They aimed to identify the local caregivers’ needs and whether adapting iSupport may address these needs. Contrary to the other countries, India did not share iSupport materials with caregivers to be reviewed during this phase. In this stage, India centered their discussion on caregivers’ needs for an online psychosocial intervention in general, without mentioning iSupport. Both the Australian and Indian studies invited caregivers to discuss in focus groups the information that they would like to see available in an online training and support programme for caregivers, facilitating factors and barriers for unpaid caregivers to use such programmes, and their suggestions on the format or additional features to increase user-friendliness (Baruah et al., 2020; Xiao et al., 2021).
In Switzerland, excerpts of iSupport were provided to caregivers as an example of intervention programmes. They assessed caregivers’ perception of the barriers and benefits of seeking help, help-seeking behaviour, and positive experience in getting support. They identified caregivers’ need for a dementia case manager who can help them navigate locally available support and services (Messina et al., 2022).
Other countries did not explicitly mention this stage, except Indonesia and Portugal which conducted a needs assessment by reviewing existing literature and databases and gathering information from local dementia associations (Teles, Napolskij, et al., 2021; Turana et al., 2023).
Phase 2: Initial adaptation
During this phase, the intervention developers and the cultural adaptation specialists co-design the adaptation, making changes deemed necessary for the iSupport to be acceptable to local caregivers (target community).
Content translation
Most countries translated iSupport into their local language except in Australia and UK, where English is the national language. (Masterson-Algar et al., 2023; Xiao et al., 2021). In India, English was chosen as the language of delivery as it had been the main language used for caregiver interventions across India (Baruah et al., 2021). Although the need of translation to other regional languages had been identified in the needs assessment stage, the authors suggested that translation to local languages could take place after preliminary evidence of iSupport effectiveness in India had been established. This was an economic consideration as the translation process was expected to be costly and time-consuming.
Most countries used a professional translator with previous experience in health or psychology, except in Spain, Switzerland, and Australia’s version for Chinese caregivers, where the study researchers translated or edited the content (Messina et al., 2024; Molinari-Ulate et al., 2023; Xiao et al., 2022) and Greece where unspecified translators were involved (Efthymiou et al., 2022). Content development of the iSupport adaptation for Australian Chinese caregivers was based on a previous adaptation study completed in mainland China (Xiao et al., 2022). The bilingual research team in Australia reviewed, discussed, and revised the mainland Chinese version and produced the Australian versions in both simplified and traditional Chinese.
Following the WHO’s guidance, an interpretative-communicative method was used to translate the text into the local language in these countries, which means understanding and recreating the original text without radically changing the meaning. The study from Indonesia also performed back-translation to ensure correct translation of the content (Turana et al., 2023). All studies reported that the research team or an expert panel performed further technical review on the first translation draft, followed by minor revisions.
Cultural adaptation processes
All included studies aimed to adapt iSupport to an online format. Most of the studies used focus groups to gather perspectives and feedback from respondents to inform the adaptation, except in Portugal, where they used expert appraisal through questionnaires (Teles, Napolskij, et al., 2021). India and UK used a mix of different methods (focus groups or co-design workshops, interviews, questionnaires, or workbooks) (Baruah et al., 2021; Masterson-Algar et al., 2023). Prior to data gathering, most studies provided caregivers with materials from the iSupport manual or access to an online platform.
In most countries except the UK, cultural adaptation was to some extent completed prior to caregiver consultations. For example, adapting the language to ensure acceptability by the target group and accuracy of the words/expressions used, changing people’s names to locally relevant ones, using local resources, and using culturally relevant references to the type of activities, food, and habits in the manual (Baruah et al., 2021; Efthymiou et al., 2022; Molinari-Ulate et al., 2023; Monteiro et al., 2023; Teles, Napolskij, et al., 2021; Turana et al., 2023). In India, findings from the “setting the stage” phase were used by the researchers to make a priori changes, which were then reviewed by two senior members of the research team (Baruah et al., 2020, 2021).
In Brazil, Greece, Indonesia, Portugal, Spain, and Switzerland, the a priori adaptations were appraised by a multidisciplinary expert panel or advisory board external from the research team (consisting of representatives from national Alzheimer’s associations, academics, field professionals, and caregivers). They reviewed language sensitivity, content clarity, familiarity of terms used, accuracy of concepts and vignettes, and adequacy of the adapted contents (Efthymiou et al., 2022; Messina et al., 2024; Monteiro et al., 2023; Teles, Napolskij, et al., 2021; Turana et al., 2023). In Spain, three separate expert groups, including a cohort of postgraduate students in dementia, were consulted through focus groups parallel to the consultation process with caregivers and healthcare professionals (Molinari-Ulate et al., 2023).
The Australian-Chinese study involved diaspora residing in Australia who are unpaid caregivers or community age care staff with Chinese background (Xiao et al., 2022). Prior to the focus group discussions, the respondents reviewed excerpts of the adapted Chinese iSupport. Similar approaches were done in Brazil and Switzerland, where the respondents were assigned only parts of the translated iSupport to reduce the amount of reading needed to be done (Messina et al., 2024; Monteiro et al., 2023). In Indonesia and Spain, the respondents were given the whole translated manual to review within at least two weeks before the discussions (Molinari-Ulate et al., 2023; Turana et al., 2023).
The UK study on adapting iSupport for young caregivers involved adolescents who cared for a family member living with dementia and researchers or social care professionals who had worked with young caregivers (Masterson-Algar et al., 2023). Participants were given two months to review and provide feedback on the original iSupport through their preferred method: using a hard copy workbook, attending online meeting sessions with the researchers, or annotating the generic iSupport manual PDF file. Three co-design workshops for young caregivers and professionals were conducted. The first workshop with young caregivers aimed to understand their general thoughts on iSupport and explore support networks and lived experiences. The findings from the first workshop were then brought to the second workshop with healthcare professionals for further discussion regarding content, language and design aspects. The final workshop combined both groups to seek their suggestions on the preliminary adaptation result.
Phase 3: Adaptation iterations
In Phase 3, changes made based on the feedback gathered in Phase 2 were captured in the resulting iSupport adaptation and further field testing and consultations with caregivers (target community) were made. Only three studies (Greece, India, Portugal) described field testing. In Greece and Portugal, caregivers were invited to test the online platform and provide their feedback on the content, delivery, and user-friendliness through online focus group discussions (Efthymiou et al., 2022; Teles et al., 2021b). In India, the field test was done through face-to-face and independent online testing (Baruah et al., 2021). During a face-to-face session, caregivers were asked to complete at least five out of the 23 lessons available and provide feedback around the content, appropriateness to cultural context, and technical aspects. Caregivers who could not attend in person were invited to use the online platform independently for a week. Besides giving feedback on the content and cultural aspects, they were also asked to provide feedback on the process of online consent and assessment and automated e-mails received as participants.
Taking into account the feedback gathered throughout the three phases, these suggestions can be grouped into changes in (i) language, (ii) content, (iii) design, and (iv) delivery format. A summary of the suggested changes can be seen in Table 3.
Language
The WHO suggested that countries could opt out of using the word ‘dementia’ if this was stigmatising in the local culture, and rather use terms such as “memory loss”(Pot, 2018). In Indonesia, they opted for the local translation of the word ‘senile’ (pikun), which unlike the connotation in English, is less stigmatised and associated more with ageing-related memory loss than with mental illness (Turana et al., 2023). This word is more widely accepted and used in dementia awareness campaigns nationally, while ‘dementia’ is seen as a medical term that is unknown to laypeople. Conversely, in Spain, they changed several parts where ‘persons with memory loss’ is used to describe ‘persons living with dementia’ (Molinari-Ulate et al., 2023). In Switzerland, several scientific terms were instead used to retain the accuracy of the description, for example, replacing ‘memory loss’ with ‘memory impairment’ (Messina et al., 2024).
Aligned with the WHO’s guidance, most countries suggested changes in words and expressions to ensure accurate equivalents. This is not always literal, for example, the translation of ‘compassion’ is changed to ‘understanding’ in Portugal and Spain, due to the former’s religious connotation in the target language (Molinari-Ulate et al., 2023; Teles, Napolskij, et al., 2021). Sometimes, there is no equivalent in the target language and the term was explained, such as ‘mindful breathing’ was translated to ‘breathing with complete awareness’ (Indonesia) (Turana et al., 2023).
After translation, word/expression changes were made to ensure understanding based on the average reading level in that country. For example, in Indonesia, the translation of ‘incontinence’ is still viewed as a medical term and thus had to be explained with examples (Turana et al., 2023). In Portugal, “practice listening without negative judgement” was translated into “practice listening without being hard on yourself” to facilitate understanding (Teles, Napolskij, et al., 2021).
The difference between formal/written and informal/spoken language was also considered when adapting the manual. Both Indonesia and Portugal opted to use more informal-style language when giving dialogues or statement examples (Teles, Napolskij, et al., 2021; Turana et al., 2023). In Indonesia, changes were also made in examples to ensure people were being addressed respectfully according to local customs and to aid the dialogue flow (Turana et al., 2023).
In some countries, the use of language had to be changed to ensure a culturally-appropriate approach; for example, in Indonesia, expressions of giving compliments were changed to more culturally-common statements, such as saying “that dress suits you” instead of “you look nice” (Turana et al., 2023). Most respondents in Switzerland found the language used patronising (e.g., ‘you finished the chapter, well done!’), prompting changes in the approach (‘you finished the chapter, let’s go to the next one.’) (Messina et al., 2024). The Portuguese, Switzerland, and UK studies also changed the school-like words and expressions used, for example, replacing the word ‘lessons’ with ‘sessions’ (Masterson-Algar et al., 2023; Teles, Napolskij, et al., 2021) or ‘chapter’ (Messina et al., 2024).
In some countries, more sensitive expressions were used; for example, saying that a person with dementia ‘shows difficulty’ instead of ‘is unable to’ in Portuguese (Teles, Napolskij, et al., 2021); or to use the word ‘difficulties’ instead of ‘limitations’ in Spanish (Molinari-Ulate et al., 2023). Similarly, UK young caregivers suggested rephrasing words that over-generalised the experiences of people with dementia, for example changing the phrase ‘people with dementia experience’ to ‘sometimes, people with dementia experience’ (Masterson-Algar et al., 2023).
Content
Adjustments to cultural habits, traditions, food, and practices are often required. For example, in the original English version, the terms ‘taking a bath’ and ‘showering’ refer to two different concepts, but in Portuguese and Indonesia, both are usually described with the same term (Teles, Napolskij, et al., 2021; Turana et al., 2023). Furthermore, in Indonesia, a shower head is not a standard household item, so they used ‘shower or water dipper’ in the adapted version.
Food, clothing items, and leisure activities were also changed according to their local culture and habit. For example, birdwatching or playing musical instruments are not popular leisure activities amongst older people in some countries, and they were changed to ‘going out to eat’, ‘going shopping’ or ‘watching TV’ in Indonesia (Turana et al., 2023). The activity of drinking tea was changed to drinking black coffee in Brazil (Monteiro et al., 2023), while food and clothing item names in India were changed to locally common ones (Baruah et al., 2021).
Some case examples or vignettes had to be changed as they were not relevant in some countries or in the target users’ group. In India, where paid support was mentioned as an option in the vignette, it was changed to family members’ or neighbours’ support. This was seen as more appropriate, considering in India, caregiving tasks are usually undertaken by the family (Baruah et al., 2021). In the UK, as the target users are young caregivers, the researchers modified several vignettes to focus on the role of a young character with caring responsibilities (Masterson-Algar et al., 2023).
The vignettes in the original iSupport were frequently presented with multiple-answer questions. Participants in Switzerland found some of the answers to be very simplistic, while some reported feeling down due to choosing a wrong answer (Messina et al., 2024). They highlighted that the situations are often not as black-and-white as the vignettes described.
Some vignettes could potentially be interpreted as demeaning to the person living with dementia. In Portugal (Teles, Napolskij, et al., 2021), one of the vignettes showed a multiple-choice answer option on a caregiver threatening to send someone with dementia to a long-term care facility as a consequence/punishment for their (changed) behaviour (Page 151: “they should say to Feng that he should be grateful for the help that he receives and if he continues to behave in this way, he will be sent to a long-term care facility.”) (iSupport For Dementia. Training and Support Manual for Caregivers of People with Dementia, 2019). Even though the vignette was aimed to explain that people with dementia should not be threatened, the expert panel suggested changing this response to avoid amplifying the stigma around long-term care facilities. They also modified some vignettes which heavily placed the care responsibility on female caregivers, even when there were male family members in the vignette. Although this is a plausible situation in Portugal, the expert panel viewed this as potentially conveying an undesirable message that caregiving is solely the responsibility of women and suggested changing it.
Indonesian caregivers found the content on changes in behaviour quite superficial and did not accurately represent what caregivers experienced, which may be more extreme. They suggested adding more case examples to better illustrate the different stages of dementia. They also suggested incorporating a self-assessment questionnaire to help caregivers gauge the stage of dementia their loved ones are currently at and determine which modules should be their priorities (Turana et al., 2023). Portuguese caregivers and professionals also suggested that dementia progression and genetics should be covered, in addition to ‘anticipatory grief’ and preparing and making decisions around moving into residential long-term care facilities (Teles et al., 2021b). Similarly, UK young caregivers suggested adding content on ‘Planning for the future’, which could discuss how to cope if the person with dementia had to move into a facility (Masterson-Algar et al., 2023). Greek caregivers requested more content on communication with paid caregivers, legal and financial aspects, Greek health services, and late-stage dementia (Efthymiou et al., 2022). Indian caregivers suggested the need for information about risk reduction strategies and cognitive stimulation activities (Baruah et al., 2020, 2021).
Design
Caregivers in the Brazilian, Indonesian, Portuguese, Spanish, and UK studies all suggested changing the illustrations, expressing a preference for more relatable human-centred images and photos over cartoon characters.
Delivery format
There are differences in caregivers’ preferences for the delivery format. Indian, Spanish, and English-speaking Australian caregivers suggested adding short video clips and audio recordings to supplement the iSupport material (Baruah et al., 2021; Molinari-Ulate et al., 2023; Xiao et al., 2022). Australian Chinese caregivers expressed their preference for an audio format, which they can listen to while doing chores (Xiao et al., 2022). In Greece, caregivers expressed their preference for a face-to-face interaction and a downloadable option of iSupport as opposed to reading on the screen (Efthymiou et al., 2022).
Features to increase user-friendliness were also suggested, such as a search function with voice recognition to easily access contents when in a hurry (Xiao et al., 2021) or the ability to change font size and colours, and backgrounds (Molinari-Ulate et al., 2023). Caregivers in most studies also proposed an integrated caregiver network to facilitate interaction with other caregivers as well as receive feedback from healthcare practitioners.
Quality assessment
All studies were critically appraised for their quality using the Mixed Method Assessment Tool (MMAT version 2018) by TS. Any queries were managed by consulting the senior author (SC). All included papers received a rating of “yes” for the questions in the relevant domains of the MMAT checklists. No papers were removed from this review due to poor quality. The completed MMAT checklist can be found in the supplementary materials (Table S1).
Discussion
In this review, we attempted to map out the iSupport adaptation process taking place in different countries. We used the Cultural Adaptation Process (CAP) framework to compare and contrast the included studies.
Findings according to the CAP framework
The adaptation processes across the included studies were analysed using the CAP framework, which cover three phases: setting the stage, initial adaptation, and adaptation iterations (Domenech-Rodríguez et al., 2011; Domenech-Rodriguez & Wieling, 2004). The included studies were at different stages of development and therefore cannot be compared head-to-head. However, comparative analysis of the adaptation stages and processes using the CAP framework enabled us to identify key areas for further refinement in adaptation processes.
Setting the stage
The adaptation process ideally starts by setting the stage through a needs assessment. However, only five studies described this step, and only three of them (Australia, India, Switzerland) involved caregivers at this stage. India’s approach stood out by not sharing iSupport as the focus of the discussion at this stage, but focusing on exploring caregivers’ expectations should an online intervention become available. This neutral approach allowed intervention developers to identify local caregivers’ needs and assess how to adapt iSupport to meet these needs. This is a valuable stage as it enables early stakeholder involvement and informs researchers about specific considerations in local adaptations, but it was not explicitly mentioned in the WHO adaptation guide. In a future refinement of the adaptation guide, this stage could be recommended.
Initial adaptation
Most of the initial adaptations for non-English speaking communities started in the translation process. Translation approaches varied, with some studies using professional translators and others using dementia researchers as informal translators. Professional translators are likely to be faster, but dementia researchers may be more informed in preferred terms or expressions in health education. Translation by the research team may also reduce the number of translation reviews needed.
Translations to local languages should be a priority in future research, but a lack of funding and resources is a common problem, especially in LMICs, such as in India’s case. This would be a barrier for caregivers who are not fluent in English (and likely to be less educated) to benefit from iSupport. Advocacy to the local government to seek their political commitment to dementia is essential in making iSupport available in more regional languages.
Another possible solution is utilising the WHO’s network to promote research collaboration between high- and lower-income countries. Developing iSupport adaptations for diaspora is vital to ensure that caregivers across the world can receive culturally relevant support and it is an opportunity for collaboration. For instance, the iSupport adaptation for Chinese diaspora in Australia was built on a previous translation work in China. A reversed approach may be explored. If researchers in another country would like to adapt iSupport for Indian diaspora residing there, they could translate and adapt iSupport-India (English version) to the regional language spoken commonly there. This translated version could then be adapted for use again in India.
Following translation, a priori adaptation, usually on cultural adjustments (food, clothing, and customs), was done in most countries. This, combined with an expert panel review before consulting caregivers, is a good practice that allows caregivers to focus on reviewing the programme content and approach in regard to dementia itself.
Most of the studies used focus groups to gather caregivers’ feedback. Although the WHO adaptation guide suggested aiming to recruit an equal gender proportion of participants, most studies involved more female caregivers than males, reflecting the real-life gender distribution of caregivers (Erol et al., 2015). In some cultures, although women manage the day-to-day caregiving activities, men are the family’s main contact point with society; therefore, it may require more men to attend the focus groups. Balancing gender representation and ensuring the voices of all caregivers are heard is crucial.
Changes often went beyond the language or reference adjustments suggested by the WHO iSupport adaptation guide. For example, vignettes and design changes were sometimes required to align with local customs and prevent stigma. Additional information on risk reduction strategies and planning for the future (including financial and legal matters) are also essential.
Adaptation iterations
Three studies described iSupport manual adaptations as the output, while the rest resulted in the adaptation hosted on an online platform. As internet access can vary across regions, it is important to ensure the adaptation result is available as a manual first before translating it into an online format.
To date, only three studies (Greece, India, and Portugal) have conducted user-testing of the online tool, gaining further feedback from caregivers. The iSupport adaptation process is an iterative process, and user-testing is an important step to ensure the tool’s acceptability and user-friendliness.
Recommendations
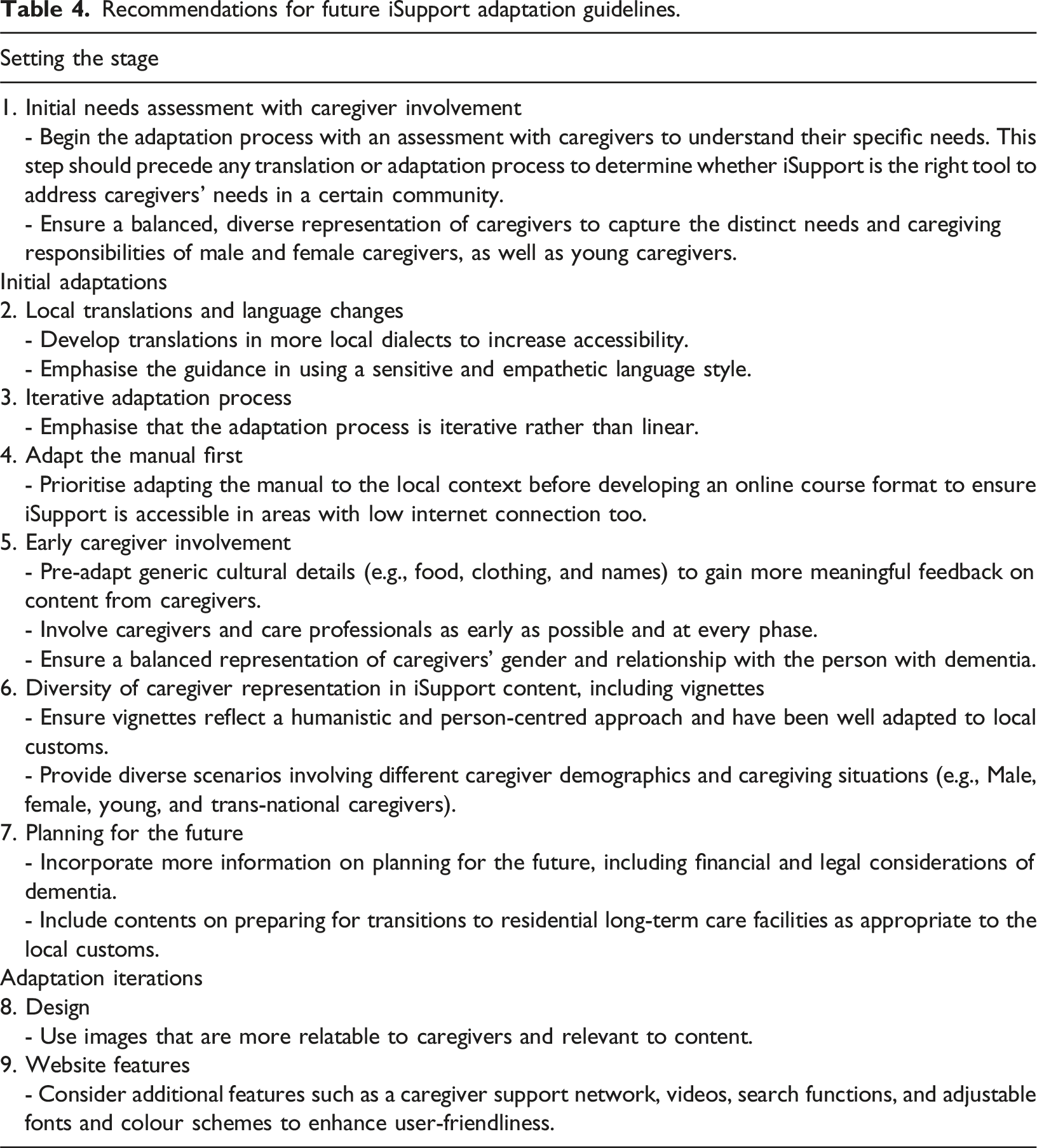
Recommendations for future iSupport adaptation guidelines.
We also suggest that the WHO might wish to update the figure in their guideline to make it clear that intervention developers (researchers) require WHO’s authorisation before adapting the iSupport, as suggested in Figure 3. Recommendations for update in the WHO adaptation guide’s diagram of the essential steps of iSupport translation, adaptation, and implementation. Modified from the source: iSupport Adaptation and Implementation Guide (Pot, 2018) Used with permission from the WHO.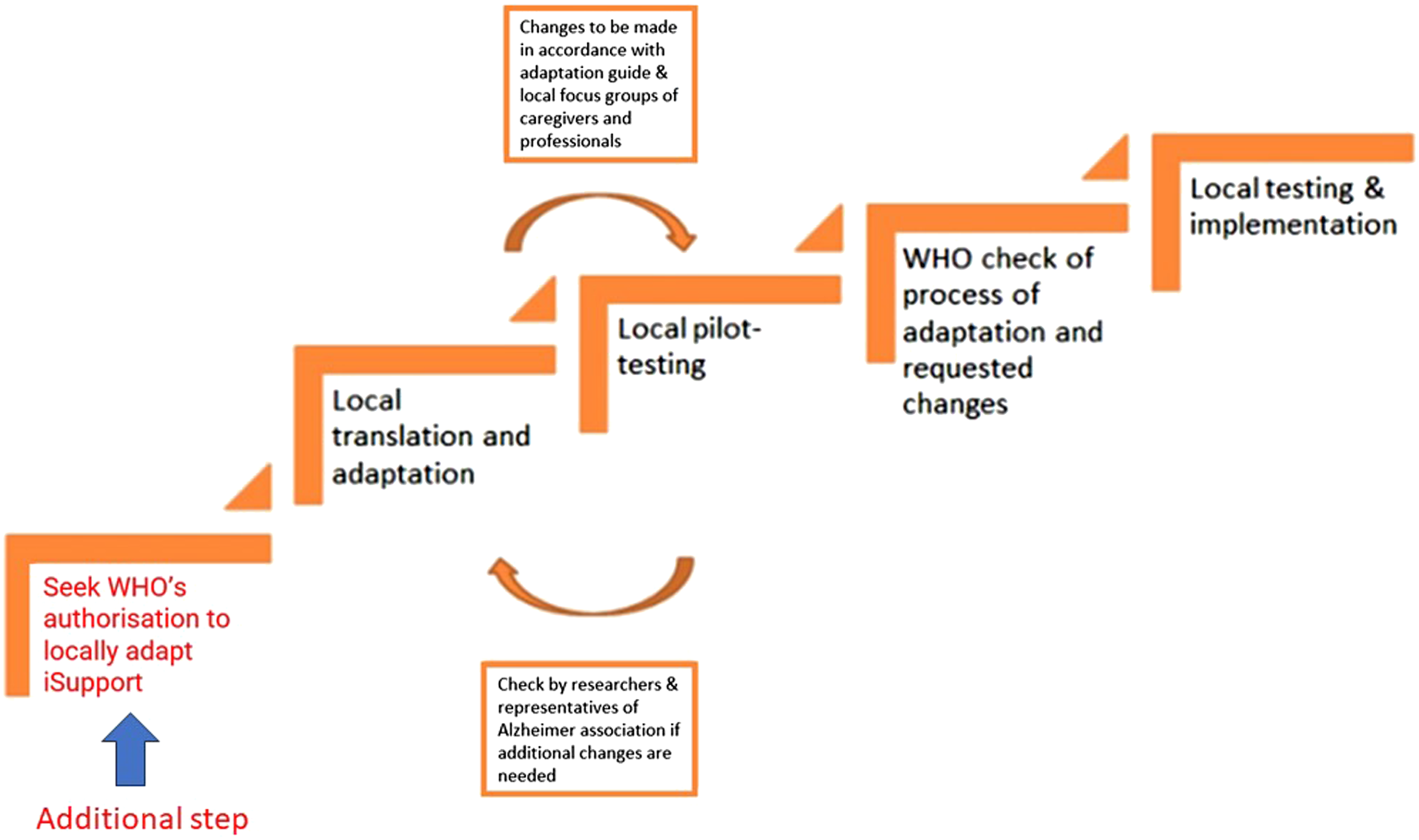
Other psychoeducational interventions
There are very few psychoeducational interventions available for family caregivers of people living with dementia even though they provide the majority of care. Although some interventions have undergone adaptation to different language and culture, not all of these adaptations have been published. For example, the UK-based START programme is available in English, English for UK black community, Urdu, Hindi, Spanish, and Japanese, and for use in India in English, Tamil, and Kannada. However, only the adaptation process for the Black and Urdu communities in the UK was described in detail (Webster et al., 2023). Similarly, the US-based REACH II programme has been translated for use in Germany, but did not undergo a cultural adaptation process. The psychotherapy-based approach used was perceived as independent of cultural differences between North America and Germany (Berwig et al., 2017). Therefore, the iSupport may be the most widely published culturally-adapted dementia psychoeducation programme to date. Thus, in this review, we have focused on iSupport for Dementia.
Strengths and limitations
The WHO iSupport for Dementia is an important first step in providing an easily accessible tool for family caregivers and many countries have started to adapt the tool for their own populations. We believe our review is the first to collate this information in a scoping review that will support future researchers who wish to adapt this tool for their own context.
There are clearly some limitations in trying to summarise and appraise many different studies due to differences in context. The studies described in this review are at different stages of adaptation and thus not directly comparable. We chose to use the CAP framework to facilitate the analysis of these studies as we felt it was the most flexible. However, there are other frameworks that are often used. For example, the WHO’s iSupport adaptation guide referenced the Ecological Validity Model (Bernal et al., 1995). It considers eight aspects of culturally adapting an intervention: language, target persons, metaphors, content, concept, goals, methods, and context. Although useful, it is very researcher-oriented and lacks a clear description of steps in an adaptation process (i.e., the ‘how’). Barrera & Castro (2006) produced a heuristic framework of the cultural adaptation with similar phases but dividing the second phase into preliminary adaptation design and preliminary adaptation test (Barrera & Castro, 2006). Another model, The Framework for Reporting Adaptations and Modifications-Expanded (FRAME), is very comprehensive, considering eight aspects in adaptation works. However, this framework focuses more on the reporting and not the sequence in an adaptation study (Stirman et al., 2019). For these reasons, we used the CAP, but we acknowledge that some of the studies in the review might have included some of the steps in the CAP phases, at different stages of their study, and therefore cannot be captured accurately in the analysis.
Another limitation is that we only included peer-reviewed publications in English. There might have been publications on iSupport for Dementia adaptation in other languages or in grey literature that we did not identify.
Conclusion
This review scoped all published studies on cultural adaptations of iSupport for Dementia. The studies were at different phases of adaptation and varying approaches were used in the adaptation process. Despite not being directly comparable, the phased approach helps gauge and compare early- and mid-stage processes researchers have used in the adaptation of iSupport.
We found that the WHO iSupport for Dementia can be effectively adapted to caregivers from diverse cultural backgrounds. Several recommendations presented in this review offer valuable insights for further refinement of the WHO iSupport adaptation guide. Given its focus on caregivers, engaging them early in co-designing its cultural adaptations is critical. With more iSupport versions in development, this review will need updating in the next 1 or 2 years.
Supplemental Material
Supplemental Material - Cultural adaptations of the WHO iSupport for dementia: A scoping review
Supplemental Material for Cultural adaptations of the WHO iSupport for dementia: A scoping review by Tara P Sani, Gary Cheung, Kathy Peri, Susan Yates, Ngaire Kerse, Hēmi Whaanga and Sarah Cullum in Dementia
Supplemental Material
Supplemental Material - Cultural adaptations of the WHO iSupport for dementia: A scoping review
Supplemental Material for Cultural adaptations of the WHO iSupport for dementia: A scoping review by Tara P Sani, Gary Cheung, Kathy Peri, Susan Yates, Ngaire Kerse, Hēmi Whaanga and Sarah Cullum in Dementia
Footnotes
Author Notes
We declare that this manuscript is original and has not been published before. It is not currently being considered for publication elsewhere.
Authors Contribution
All authors have contributed to the manuscript. TP Sani, S Cullum, and G Cheung formulated the research question and methodology. TP Sani conducted the systematic literature search and wrote the paper. S Cullum, G Cheung, S Yates, K Peri, H Whaanga, and N Kerse assisted in writing the paper. All authors have approved the manuscript and agreed with its submission to Dementia.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project, Empowering Dementia Carers with an iSupport Virtual Assistant (e-DiVA), was funded by the New Zealand Health Research Council (Grant no: 20/1133). TP Sani is a PhD student who receives a scholarship from the HOPE Foundation for Research on Ageing.
Ethical statement
This scoping review article does not involve primary research data collection or experimentation with human or animal subjects. As such, formal ethical approval was not sought nor required.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.