
Abstract
Introduction
Obesity is a growing public health concern in Lebanon. Angiotensin-converting enzyme (ACE) plays a critical role in the renin-angiotensin system, affecting blood pressure and metabolism. Genetic variations in the ACE gene, particularly the insertion (I)/ deletion (D) polymorphism, have been linked to obesity risk in various populations. This study aimed to investigate the association between the ACE I/D polymorphism and obesity in a sample of North Lebanese population.
Materials and methods
A total of 192 participants were enrolled and categorized into “obese” and “non-obese” groups. Genomic DNA was extracted from peripheral blood, and the ACE I/D polymorphism was identified using polymerase chain reaction. Data were further stratified by age and exercise frequency. Statistical analyses were performed using SPSS version 27.
Results
Genotype frequencies were D/D (45.8%), I/D (39.6%), and I/I (14.6%), with a minor allele frequency of 0.34. No significant association was found between the ACE I/D polymorphism and obesity in terms of genotypic and allelic distributions, even after adjusting for confounding factors and stratifying the data. No significant gender-related differences were also observed.
Conclusions
These findings suggest that the ACE I/D polymorphism may not significantly influence obesity risk in this population. Larger studies are needed to clarify the genetic basis of obesity in Lebanon.
Introduction
Obesity has emerged as a major public health concern worldwide. In 2022, 43% of adults aged 18 and above were classified as overweight, while 16% were living with obesity. 1 This condition arises from complex interactions between genetic, lifestyle, and environmental factors,2,3 associating with numerous medical complications that adversely impact quality of life. 4 Over the past two decades, obesity rates in the Middle East have been steadily increasing. 5 Latest national studies conducted between 2008 and 2009 report that among Lebanese adults aged 20 and above, around 36.8% were overweight and 26.1%–28.2% were obese.6,7 Also, among children and adolescents aged between 6 and 19 years, about 34.8% were overweight and 13.2% were obese. 8
Extensive research has focused on polymorphisms in multiple obesity-related genes 9 ; among them is the angiotensin-converting enzyme (ACE) gene. 10
The ACE gene, located on chromosome 17q23, displays a remarkable polymorphism in both its promoter and coding region, most notably the well-studied insertion/deletion (I/D) of 287-base pair Alu repeat sequence within intron 16 that showed significant implication in several health conditions, particularly hypertension, coronavirus disease 2019, and neurological disorders, among others.11–14 Not so far, this polymorphism emerges as a focal point of research due to its association with obesity risk in different populations, with conflicting evidence.15–24 The mechanism centers on the fact that the D allele is associated with higher ACE activity, which increases angiotensin II production both locally and systemically in adipose tissue. 25 Animal studies showed that this hormone promotes adipocyte hypertrophy and hyperplasia, further contributing to fat accumulation. 26
While the polymorphism alone is not a definitive predictor of obesity, it contributes to the complex genetic architecture underlying obesity susceptibility and may help identify individuals at higher risk, especially when considered with other genetic markers and lifestyle factors, highlighting gene-environment interactions, where individuals with high genetic risk are more likely to develop obesity in obesogenic environments, but healthy lifestyle choices can reduce this risk, even among those genetically predisposed. 27 This underscores the need for personalized prevention and management strategies that consider both genetic and environmental factors.
Given the high prevalence of obesity among Lebanese adults and the inconsistent findings regarding the association of ACE I/D polymorphism with this condition, this study aims to investigate the potential influence of ACE I/D gene polymorphism on obesity risk in a representative sample of the indigenous population of northern Lebanon.
Materials and methods
Study population
This case-control study included 192 individuals, comprising 74 males and 118 females. Inclusion criteria consisted of participants aged between 18 and 65 years, presenting or not general obesity defined as body mass index (BMI) ≥ 30 Kg/m² according to the World Health Organization criteria; thus, volunteers were categorized as non-obese (BMI < 30 kg/m², n = 104) or obese (BMI ≥ 30 Kg/m², n = 88). Exclusion criteria included pregnancy or lactation, presence of genetic syndromes associated with obesity, and current use of medications affecting weight, including weight-management medications or obesity-promoting drugs.
Ethical approval and participant consent
The current study was conducted in accordance with the Declaration of Helsinki and received approval from the Institutional Research Ethics Committee of Jinan University, Lebanon. All participants provided written informed consent prior to enrollment, acknowledging their understanding of the study objectives, procedures, and potential risks associated with genetic testing. Confidentiality of genetic and clinical data was strictly maintained through coded identifiers and secure data storage. Participants were informed of their rights to withdraw consent at any time without penalty. The collection and analysis of biological samples were performed under stringent ethical guidelines.
Data collection
This study was conducted between March 2024 and January 2025. Baseline characteristics, including age, gender, physical activity level, stress level, and smoking status, were collected using a structured questionnaire. Anthropometric measurements—weight and height—were obtained using a calibrated digital balance and a stadiometer, respectively. BMI was calculated as weight in kilograms divided by height in meters squared.
Blood withdrawal and DNA extraction
Whole blood sample (2 ml) was drawn from each participant in EDTA tube for genomic DNA extraction. DNA was isolated from 200 µL of each sample using the GenElute™ Mammalian Genomic DNA Miniprep Kit (Sigma-Aldrich, St. Louis, MO, USA), according to the manufacturer protocol. The purity and concentration of the extracted DNA were assessed by measuring absorbance at 260 and 280 nm using a spectrophotometer (Thermo Fisher Scientific, catalog number 840-208100, USA). DNA integrity was evaluated by agarose gel electrophoresis (Bio-Rad Mini Sub-Cell GT, USA).
ACE I/D polymorphism genotyping
Genotyping for ACE I/D polymorphism was carried out by polymerase chain reaction (PCR) using a thermal cycler (Bio-Rad, C1000, USA), following previously described protocol. 28 All primers were confirmed using Basic Local Alignment Search Tool (BLAST).
PCR products were separated on a 2% agarose gel and visualized with ethidium bromide. The presence of D and I alleles was indicated by 190-bp and 490-bp bands, respectively.
Power analysis and sample size considerations
A power analysis confirmed that a sample size of 192 participants is adequate for detecting medium effect sizes with 80% power at a 0.05 significance level. This includes chi-square tests for categorical variables (Cohen's w = 0.3), ANOVA for continuous variables (Cohen's f = 0.25), and regression analyses with 2–3 predictors (Cohen's f² = 0.15). The sample size ensures sufficient statistical power to detect meaningful differences and associations.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics for Windows, version (IBM Corp., Armnok, N.Y., USA). The Hardy–Weinberg equilibrium for the genotypic distribution was assessed using a Chi-square goodness-of-fit test with one degree of freedom. Data were expressed as mean ± standard deviation, frequency (n) and percentage (%), or median with interquartile range (median, Q1–Q3), as appropriate. Continuous variables were compared across groups using one-way analysis of variance (ANOVA). Categorical variables were analyzed using Chi-square test; when expected cell counts were less than five, Fisher's exact test was applied as appropriate. Independent samples t-test was used to compare the means of a continuous variable between two independent groups. Binary logistic regression model was performed to adjust ORs and P-values for potential confounding factors. A P-value < 0.05 was considered statistically significant.
Results
The association between baseline characteristics and BMI categories was investigated in a sample of 192 participants, divided into non-obese (BMI < 30 kg/m², n = 104) and obese (BMI ≥ 30 kg/m², n = 88) groups. The study population comprised 118 females and 74 males. Detailed characteristics are presented in Table 1.
Baseline characteristics and lifestyle factors of the studied BMI categories

Data are presented as mean ± standard deviation, median and interquartile range, or frequency (%). P-values were calculated using the Chi-square test to examine associations between categorical variables, or independent samples t-test to compare the means of continuous variables. * Differences are considered statistically significant (P < 0.05).
As shown, there were no significant differences between the two BMI groups regarding gender distribution (62.5% vs. 60.2% females; P = 0.768), average height (1.67 m vs. 1.65 m, P = 0.073), positive smoking status (47.1% vs. 46.6%, P = 1.000) or reported stress cases (31.7% vs. 27.0%, P = 0.223). However, significant differences were noticed in age, body weight, BMI, physical activity frequency, and education level. The obese group was older (median age: 30.0 vs. 22.0 years; P < 0.001), and had higher mean weight (95.5 kg vs. 66.0 kg; P = 0.001) and BMI (35.2 kg/m² vs. 24.0 kg/m²; P < 0.001), engaged less in regular physical activity (15.9% vs. 31.7%, P = 0.012), with a smaller proportion having attained higher education (51.1% vs. 72.1%, P = 0.004).
The presence or absence of the ACE 287-bp insertion/deletion (I/D) polymorphism was confirmed by separating PCR products on a 2% agarose gel (Figure 1).

Agarose gel electrophoresis of PCR products for the ACE I/D polymorphism. Lane 1: DNA marker; Lane 2: negative control; Lanes 3,4,6, and 7: samples with I/D genotype; Lanes 5 and 9: samples with D/D genotype; Lane 8: sample with I/I genotype
The distribution of the studied polymorphism varied across the population, with the D/D genotype being the most prevalent (45.8%), followed by the I/D genotype (39.6%), and the I/I genotype being the least represented (14.6%). The allelic distribution showed a higher frequency of the D allele (0.66) compared to the I allele (0.34).
The distribution of ACE I/D genotypes by obesity status, and various sociodemographic and lifestyle factors was further analyzed. Results are summarized in Table 2.
Distribution of ACE I/D genotypes by obesity status, sociodemographic characteristics, and lifestyle factors

Data are presented as mean ± standard deviation or frequency (%). P-values were calculated using the Chi-square test or one-way analysis of variance (ANOVA). * Differences are considered statistically significant (P < 0.05). BMI: Body mass index; D: Deletion; I: Insertion.
As shown, no significant differences in genotype distribution were observed with respect to all studied characteristics.
Given the presence of statistically significant differences in several BMI-related confounders-including age, physical activity frequency, and education level- between the obese and non-obese groups, further adjustments were considered necessary to control for potential bias. However, despite controlling for these covariates, significant differences in age and physical activity frequency persisted (Table 3).
Logistic regression analysis to predict variables related to BMI

OR: Odds ratio, CI: Confidence interval, a P-value: Adjusted P-value for body mass index confounders;
D: Deletion; I: Insertion. * Differences are considered statistically significant (P < 0.05).
Consequently, stratified analyses were subsequently conducted based on physical activity frequency (regular vs. irregular) and age (< 30 years vs. ≥ 30 years). The distribution of ACE genotypes across the four resulting strata (S1-S4) is presented in Table 4.
Genotypic distribution of ACE 287-bp I/D polymorphism across stratified groups
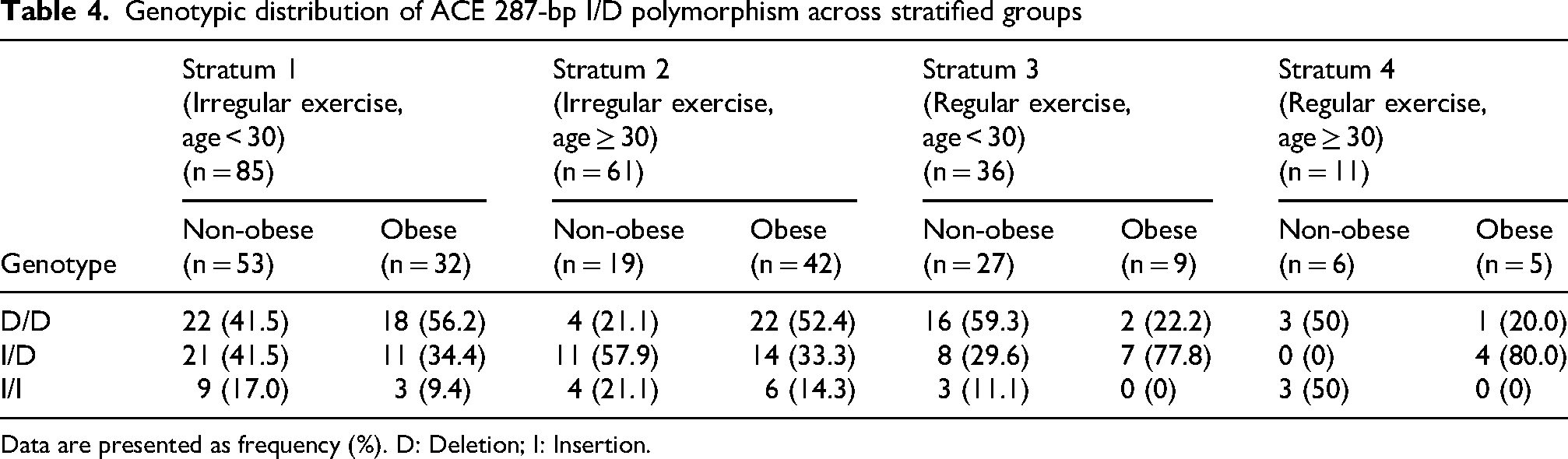
Data are presented as frequency (%). D: Deletion; I: Insertion.
Due to the limited sample size in Stratum 4 (S4), it was excluded from subsequent analysis. Logistic regression models were then applied to Strata 1, 2, and 3, adjusting for all registered BMI confounders, including gender, smoking status, education level, and stress. Results are illustrated in Table 5.
Logistic regression analysis of variables associated with BMI, adjusted for confounding factors

a P-value: Adjusted P-value for body mass index confounders. D: Deletion; I: Insertion; OR: Odds ratio; CI: Confidence interval.
*: Differences are statistically significant (P < 0.05).
As presented, adjusted P-values for all confounders exceeded 0.05 across all strata, indicating that these variables did not significantly influence genotype associations. Results were consistent, particularly in strata 1 and 2. Adjusted odds ratios (ORs) and corresponding P-values for the comparison between D/D and I/D genotypes indicated no statistically significant associations across all strata: S1 (OR: 1.75, aP = 0.476), S2 (OR: 1.75, aP = 0.476), and S3 (aP = 0.999). Similarly, D/D vs. I/I genotype analysis revealed no significant associations after adjustment: S1 (OR: 3.34, aP = 0.117), S2 (OR: 3.79, aP = 0.120), and S3 (aP = 0.999). Likewise, none of these values reached statistical significance in the recessive genetic model D/D vs. (I/D + I/I), where adjusted statistical analyses were as follows: S1 (OR: 2.43, aP = 0.108), S2 (OR: 3.79, aP = 0.120), and S3 (aP = 0.999). Overall, the findings indicate no significant association between ACE 287-bp I/D genotypes and obesity status.
Correlation and logistic regression analyses were then performed to assess whether the studied variables differed by gender prior to further exploration of the potential gender-based association between ACE I/D polymorphism and obesity. Results are presented in Table 6.
Correlation and logistic regression analyses for identification of potential sex-dependent variables

**: P < 0.01; *: P < 0.05; NS: Not significant; aP-value: Adjusted P-value for potential sex-dependent variables. a P < 0.05 are considered statistically significant.
Age was significantly positively correlated with sex in both females (r = 0.300, p < 0.01) and males (r = 0.443, P < 0.01), indicating age differences by gender. Physical exercise frequency showed a significant positive correlation only in females (r = 0.210, P < 0.05), whereas in males the correlation was not significant. Education level was negatively correlated with sex for females (r = −0.216, P < 0.05) but not significantly correlated in males. Smoking status and stress level did not exhibit significant correlations in either group. Logistic regression model adjusting for these variables demonstrated significant associations for physical exercise frequency, education, and stress levels. Consequently, stratified analyses were conducted based on physical activity frequency and education level, with adjustment for stress level. Four strata were generated (S1: irregular exercise, higher education, n = 82), S2 (irregular exercise, pre-tertiary education, n = 63), S3 (regular exercise, higher education, n = 38), and S4 (regular exercise, per-tertiary education, n = 9). Only the first three strata were included in further gender-based analyses of the association between ACE I/D polymorphism and obesity, adjusting for stress levels. Results are presented in Table 7.
Analysis of ACE 287-bp I/D polymorphism with gender across stratified groups

Data are presented as frequency (%). P-values, OR and 95% CI were calculated using the Chi-square test.
P-value: Adjusted P-value for stress levels; D: Deletion; I: Insertion; OR: Odds ratio; CI: Confidence interval; NA: Not applicable. a P < 0.05 are considered statistically significant.
No significant association was also reported between gender and genotype in any subgroup. In S1—the largest subgroup—the D/D and I/D genotypes showed non-significant differences by gender (aP = 0.842 and P = 0.918, respectively). Similarly, allele frequencies did not differ significantly between males and females (P = 0.595 for D allele, and P = 0.402 for I allele).
Lastly, a comparative analysis of the association between ACE I/D polymorphism and obesity across different populations was carried out and is summarized in Table 8.
Comparative analysis of ACE I/D polymorphism and obesity association across different populations

CC: Case-control; CS: Cross-sectional; MA: Meta-analysis; M: Male; F: Female.
Overall, the findings suggest that the ACE I/D polymorphism contributes to obesity risk, particularly among individuals of African and European descent. However, these associations remain inconsistent, as also reflected in the present study and other investigations involving Middle Eastern and Asian populations.
Discussion
This study investigated the association of ACE I/D polymorphism in 192 northern Lebanese residents, categorized into obese and non-obese groups. While gender, smoking status, and self-reported stress did not differ significantly between groups, other variables showed marked differences. As expected, the obese group had significantly higher mean weight (95.5 kg) and BMI (35.2 kg/m²) compared to the non-obese group (66.0 kg and 24.0 kg/m², respectively; P < 0.001). Notably, two major BMI-related confounders—age and physical activity— along with the education level, differed significantly between both groups. The median age was higher in the obese group (30 vs. 22 years, P < 0.001), and regular physical activity was less common (15.9%) compared to the non-obese group (31.7%, P = 0.012). Participants with higher education degrees were also more frequently observed in the non-obese group compared to the obese group (72.1% vs. 51.1%, P = 0.004). These findings emphasized the necessity of adjusting for these covariates in subsequent analyses, as they could independently influence obesity outcomes, potentially confounding the effect of the studied ACE polymorphism on obesity risk. Initial logistic regression analyses failed to fully adjust for these confounders- except for education level- therefore, a stratification analysis based on age and physical activity was subsequently performed.
The present study revealed a predominant D allele frequency of 0.66, with genotype distributions of DD (45.8%), I/D (39.6%), and I/I (14.6%). Similar trends have been reported in Lebanese baseline studies, with the D allele along with D/D and I/D genotypes also being predominant.29,30 Compared to other populations, notably Arabs and Africans, the dominance of the D allele in Lebanon aligns with findings in various South, Southeast Asian and Middle Eastern countries, where its frequency ranges from 0.56 in Malaysia to 0.78 in Egypt.15,23,31–34 In contrast, South American populations show a more balanced allelic distribution, with the I allele frequency at 0.44 and a 20.5% prevalence of the II genotype. 25 East Asian populations, including Koreans and Japanese, display an even higher I allele frequency (> 0.50) with the II genotype being most common.35,36 These findings underscore regional variations, with the Lebanese population, like other Middle Eastern groups, exhibiting a high prevalence of the D allele,31–33 reflecting a shared genetic landscape that may contribute to the burden of metabolic, cardiovascular, and infectious diseases in the region. 37
To control for BMI-related confounding factors, logistic regression analysis was performed after stratifying participants by age and physical activity frequency. Despite adjustments for covariates, results remained non-significant in all three strata in terms of allelic and genotypic distributions between obese and non-obese groups. Gender-specific associations were also not observed in this study population. These findings suggest that, within the northern Lebanese population, the ACE I/D polymorphism is not associated with obesity even when confounding factors are properly considered.
Few studies have investigated the association between obesity and ACE I/D polymorphism in Asian and African populations. A meta-analysis of 14 case-control studies (3371 overweight/obese cases and 4490 controls) across African, Caucasian, and Asian populations found a significant association between the ACE gene DD genotype and increased risk of overweight/obesity overall (P = 0.014), with a stronger effect observed in individuals of African descent (P = 0.010). Additionally, the D allele was linked to a higher risk in Africans (P = 0.026), while the II genotype showed no protective effect in any population. 10 Moreover, a case-control study in a Tunisian population (259 overweight/obese and 369 controls) found significant associations between ACE I/D polymorphism and BMI (P ≤ 0.001) with the I allele being linked to a lower BMI, suggesting a potential protective effect. 20 Additionally, in Pakistan, the DD genotype was significantly more prevalent among obese adults than in normal-weight or overweight groups, supporting the role of the D allele in adipogenesis and adipocyte metabolism. 23 A study conducted on middle-aged Caucasians showed a gender-based association where the I allele of the ACE I/D polymorphism was significantly correlated with higher BMI in men but not in women. 22 However, in Egypt, a case-control study among 80 females reported no significant association between ACE I/D genotypes and obesity or common related conditions, 15 with similar findings across Saudi, 16 Malay, 17 Korean, 18 and Indian 19 subjects. Research in pediatric populations also highlights the potential of ACE I/D polymorphism as a predictive indicator of obesity. Among Brazilian schoolchildren, findings indicate that the combined analysis of specific genetic polymorphisms, including the ACE I/D variant, may be a useful genetic marker for predicting the risk of severe obesity in children, suggesting that genetic profiling may help in identifying children at higher risk for developing obesity. 21 Collectively, the evidence indicates that the ACE I/D polymorphism plays a role in obesity risk, with the D allele and DD genotype generally associated with an increased susceptibility, particularly among individuals of African10,20 and European descents.21,22 In contrast, the I allele has been suggested to exert a protective effect against obesity and its comorbidities in certain contexts.20,38 Nevertheless, both associations appear inconsistent, as demonstrated in the present study and in other investigations from Middle Eastern and Asian populations.15,17,18 Such discrepancies may reflect differences in genetic background, environmental exposures, sample size, or study design.
Although no association was found between the ACE I/D polymorphism and obesity in this study, it is important to recognize that dietary and cultural factors in Lebanon can interact with genetic background, reinforcing the concept of gene-environment interplay. For instance, traditional Lebanese diets—rich in fruits, vegetables, legumes, and fish—are linked to lower risks of overweight and obesity, while westernized dietary patterns high in fast food and sugary beverages are associated with increased obesity risk among both children and adolescents.8,39,40 Cultural influences such as maternal education, family eating habits, and urbanization further shape dietary choices and lifestyle behaviors, which can either mitigate or exacerbate genetic predispositions to obesity.8,39,40 Additionally, the Lebanese genetic structure has been shaped and maintained by historical, religious, and geographic factors, suggesting that the interaction between inherited traits and environmental exposures is particularly relevant in this context, 41 ,42 highlighting the importance of considering both genetic and environmental factors in studies related to obesity and associated health outcomes in Lebanon.
This study is subject to certain limitations, including a relatively small sample drawn from a single Lebanese region and a higher proportion of female participants, which may affect generalizability and introduce gender bias. The lack of standardized stress and physical activity assessments could also reduce measurement consistency. Despite these limitations, the findings offer valuable insights and a foundation for larger, more balanced studies using validated tools. Future Lebanese research should focus on integrating genetic data with biochemical and metabolic markers to clarify the role of ACE I/D polymorphism in metabolism.
Conclusion
These findings establish reference data for ACE I/D genotype frequencies in northern Lebanon (D/D 45.8%, I/D 39.6%, I/I 14.6%) and demonstrate that, despite the high prevalence of the D allele, no clear association with obesity was observed. This underscores that obesity risk is likely influenced more by polygenic factors and environmental or lifestyle determinants rather than a single gene variant, providing important baseline information for future genetic studies in the Lebanese population.
Footnotes
Acknowledgements
The authors would like to thank Dr. Mohamad Kilani and Mrs. Faten Kamzoul for their assistance in blood collection, as well as all volunteers who contributed to this study.
Ethical considerations
The study received approval from the Ethics Committee of Jinan University of Lebanon. All procedures followed were in accordance with the Helsinki Declaration of 1964 and later versions.
Consent to participate
A written informed consent form was obtained from all volunteers prior to data collection.
Author contributions
Alaa Matar: Conceptualization, supervision, formal analysis, and manuscript writing.
Rim Al-Hallak: Investigation and resource provision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data accessibility statement
All data are available from the corresponding author upon reasonable request.